


Micromesh Dual-Layer Technology for Carotid Artery Stents
VASCULAR DISEASE MANAGEMENT 2016;13(10):E222-E229
Abstract
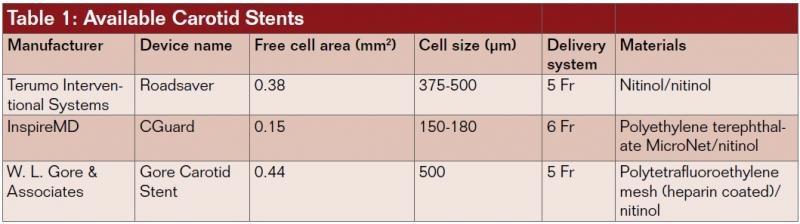
Based on lesion location and vessel characteristics, various carotid artery stent designs are available with different attributes like flexibility, conformability, radial force, and plaque penetration, making carotid artery stenting an attractive option in the treatment of carotid artery disease. However, despite improvements in patient selection and endovascular set-up, the risk of late embolization remains. The purpose of this review is to evaluate the performance and effectiveness of micromesh dual-layer technology as a new option for stent-protected angioplasty and to present it as part of the portfolio of carotid artery stents. The micromesh carotid stent is characterized by an external self-expanding layer for scaffolding and an internal micromesh layer for plaque coverage, combining the advantage of an open- and closed-cell stent design. The currently available FDA-approved double-layer micromesh stent is the Roadsaver stent (Terumo Interventional Systems). This self-tapering stent is composed of two nitinol interwoven mesh layers, creating a flexible scaffold completed through an internal fine meshwork with an extremely small cell size (0.381 mm2), designed to prevent plaque prolapse. The CGuard Carotid Stent System (InspireMD) is built using MicroNet, a biostable mesh woven from a single strand of 20 μm polyethylene terephthalate. The Gore Carotid Stent (W. L. Gore & Associates) consists of an open-cell nitinol frame supplemented with an outer closed-cell 500 µ lattice, which is coated with hemocompatible heparin. Ongoing trials and preliminary results are discussed.
Despite the variety in available carotid artery stents, developments and technical improvements are still occurring. In lesion-specific carotid artery stenting (CAS), matching the suitable technology to each disease, the interventionalist can choose among an array of different stent designs.1,2
Although CAS has been proven a minimally invasive alternative to endarterectomy, there are unsolved challenges, such as late thrombosis due to plaque prolapses. Approximately two-thirds of CAS-related stroke or transient ischemic attack (TIA) occurs post procedure, likely caused by late emboli through the struts of the stents.3 With increasing experience and technical skill of operators in high-volume centers regarding patient selection and pretreatment, there has been a shift from intra- to postprocedural complications.3,4 Lin et al detected that operator experience increases the technical success rate after 50 CAS procedures. The 30-day stroke and death rate falls to 8% after 50 interventions, to 2% after 100 cases, and to 0% after 150 procedures (P<.05). Procedural success was also enhanced partly by endovascular device refinement and an improved anticoagulation regimen.5
Impact of Stent Design
Although there has been lively discussion about the impact of stent design, there exists no prospective randomized study demonstrating the superiority of one specific cell design.6 Nevertheless, several studies have revealed that stent design can play an important role in preventing distal embolization.2,7 Current studies and subanalyses show a trend toward using a closed-cell design.8
Tailored stents may improve clinical outcomes.1,2,4 Whereas straight lesions may favor rigid stents, elongated vessel anatomy may require stents offering more flexibility. On the other hand, soft plaques may result in greater tissue prolapse though the stent struts, requiring more wall coverage.
The ideal stent should combine attributes like flexibility, conformability, bending stiffness, and radial force with wall adjustment to prevent plaque penetration. Due to the potential risk of stent collapse and low flexibility, balloon-expandable stents, first used in 1995, were abandoned. Today, only self-expanding stents with different materials and underlying design are used for CAS.9 Depending on the density of the bridge connection between ring segments, stents are classified as having open-cell, closed-cell, or hybrid-cell design, which is a combination of open-cell and closed-cell design.
Open-Cell Stents
Open-cell stents are characterized by a larger free cell area between struts, which offers a high flexibility and conformability in tortuous vessels. The RX Acculink Carotid Stent System (Abbott Vascular) has the largest free cell area (11.48 mm2) of all open-cell stents.6 This self-expanding nitinol stent consists of a nested ring design with three longitudinal spins. In descending order in respect to free cell area, Protege RX Carotid Stent System (Covidien; 10.71 mm2), Exponent RX Self-Expanding Carotid Stent (Medtronic; 6.51 mm2) and Precise Pro RX Nitinol Stent System (Cordis; 5.89 mm2) are mentioned.10 The main criticism is the risk of higher plaque penetration increasing with greater cell size and fish scaling at the concave surface.11
Closed-Cell Stents
Closed-cell stents have fewer bridge interconnections, which offer smaller free cell areas. The prototype of the closed-cell design, the Wallstent endoprosthesis (Boston Scientific), is characterized by higher bending stiffness (291.1 N/mm2) and higher collapse pressure (0.48 bar).9 Further benefit is derived from more plaque coverage, which minimizes plaque protrusion. The mechanical break-up of arteriosclerotic plaque material is one of the main risk factors during a CAS procedure. Plaque coverage characterizes how tight the stent cells cover the plaque material within the stenosis, protecting it from dislodging. One of the potential problems with handling closed-cell stents applied in vessels with tortuosity is the risk of displacing the curves to the end of the struts, leading to distal kinking.
Tietke et al retrospectively analyzed 358 unprotected CAS procedures and demonstrated that unprotected CAS with small-cell stents results in a very low procedural overall peri-interventional complication rate (0.8%, 3/358). Only 20% (3/15) of all complications occurred peri-interventionally. They concluded that the use of a protection device is dispensable.8
Hybrid Technology
Hybrid technologies have recently been developed, including the Cristallo Ideale stent (Medtronic) and the cylindrical and conical Sinus Carotid RX stent (Optimed) with a closed-cell design in the middle segments combined with open-cell design in the proximal and distal segments. In an in-vitro experiment of stent design, Müller-Hülsbeck et al described the lowest particle penetration (1.5 mm) for the Cristallo Ideale stent compared to the open- and closed-cell stents.11 In another experimental investigation, Wissgott et al found that the Sinus Carotid RX and the Cristallo Ideale stent had the best wall adjustment, with comparable radial force and high flexibility compared to open- or closed-cell designs.9 Cremonesi et al, in a prospective multicenter study of 124 patients, reported no technical failure in CAS procedures with Cristallo Ideale stents and a rate of 1.6% device- and procedure-related TIAs within 30 days of follow-up.4 Despite promising results, hybrid technology has not become a standard CAS therapy.
Dual-Layer Micromesh Technology
Based on the idea of sustained embolic protection, a new concept of stent-protected angioplasty has been established. Embolic protection starts with implantation of the stent into the lesion and continues with the process of neointimalization.12 The prototype of a membrane stent (MembraX) consists of a self-expandable nitinol stent with a membrane bonded to the inner side of the stent. The porous membrane is made of a biocompatible silicone-polyurethane copolymer Elast-Eon (AorTech Biomaterials)12 The MembraX stent system has not yet been studied in vivo and has not received the CE Mark for use in treating carotid artery disease.
However, the new double-layer micromesh design is characterized by an external self-expanding nitinol layer for scaffolding and an internal micromesh layer for plaque coverage, combining the advantage of both open- and closed-cell stent designs. The three available double-layer mesh stents are detailed in Table 1.
Micromesh Stent Design Overview and Study Data Roadsaver
The Roadsaver stent (Terumo Interventional Systems) currently is the only FDA-approved, CE-marked, commercially available double-layer micromesh stent. This self-tapering stent is composed of two nitinol (nickel titanium) interwoven mesh layers, creating a flexible scaffold. The inner mesh has an extremely small cell size (0.381 mm2), which is designed to prevent release of emboli. The internal fine meshwork should prevent plaque prolapse.17 A number of micromesh cells fit into one macromesh cell, acting like a metallic covered stent.
Data from the manufacturer show that the stent tapers according to the anatomy, without overstretching the vessel wall. The radial force decreases with decreased pressure, so that no tapered version should be needed.
The device is compatible with a 5 Fr sheath or 6 Fr guiding catheter. Up to the point of 50% deployment, the push-and-pull stent delivery system is full resheathable and repositionable. The low profile (5 Fr) enhances the crossability for primary stenting. The double-layer micromesh scaffold should enable sustained embolic protection by tight plaque coverage. The feasibility, efficacy, and safety of performing carotid angioplasty and stenting with the Roadsaver stent has been demonstrated in two studies.15,16 Kedev et al used transradial slender 5 Fr techniques to implant the Roadsaver stent in the left and right carotid arteries with promising results.16
Patient enrollment for the prospective, multicenter CLEAR-ROAD trial (Physician-Initiated Carotid TriaL Investigating the Efficacy of Endovascular Treatment of Carotid ARterial Disease with the multilayer ROADsaver stent) closed in February 2016. The primary endpoint, major adverse events (MAEs) at 30 days, was defined as the cumulative incidence of any periprocedural (≤30 days post procedure) death, stroke, or myocardial infarction (MI). Of all patients, 31% were symptomatic, and in 58% of the patients embolic protection devices were used. Technical success was achieved in all cases. The 30-day MAE rate was 2.1% (one patient experienced MI followed by death; another patient experienced a stroke within the first 30 days after the procedure), making the Roadsaver stent safe and effective for endovascular treatment of subjects at high risk for carotid endarterectomy.17
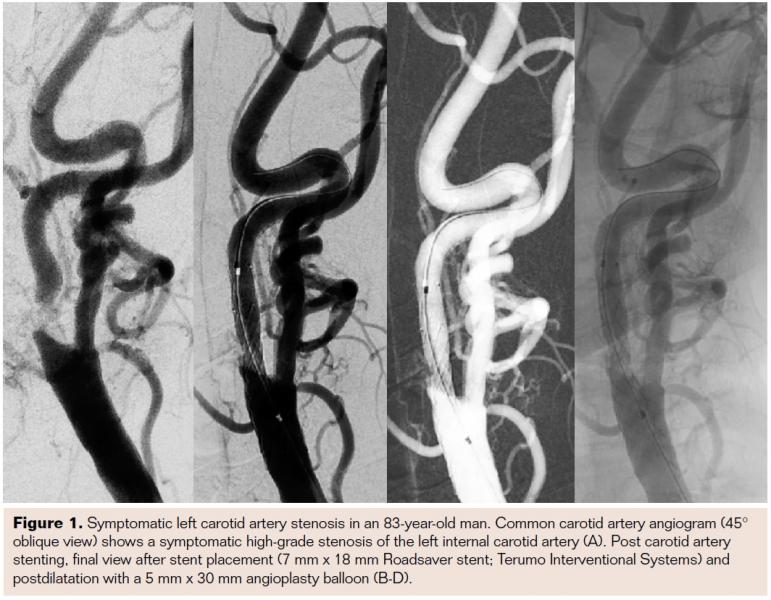
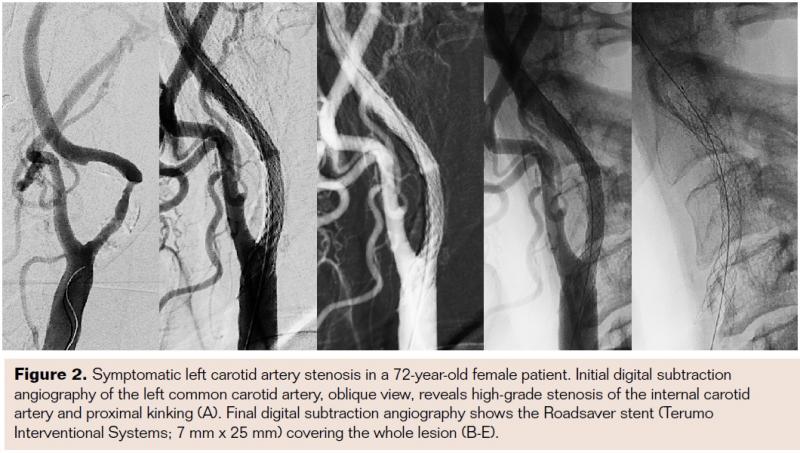
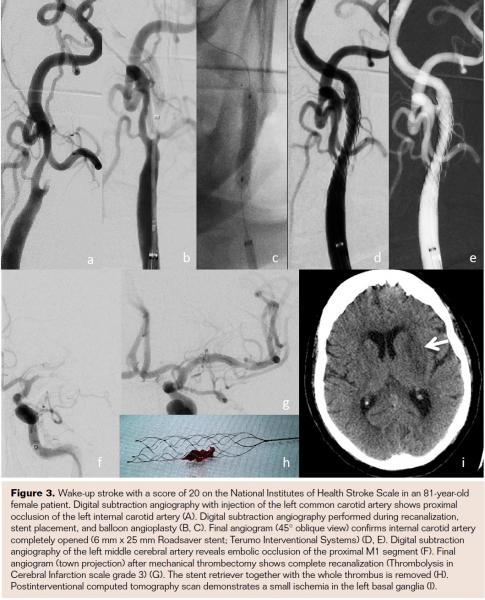
In addition to these first clinical data and experience with the Roadsaver stent, it is necessary to clarify that a certain learning curve for safe and accurate stent placement is warranted. This is because experience is needed to predict the stent length. It is highly recommended to start with larger diameters or longer stent lengths in order to achieve good lesion covering. In Figures 1-3 the Roadsaver stent is shown in 3 different anatomical locations.
CGuard
The CGuard stent (InspireMD) is composed of MicroNet, which is a biostable mesh woven from a single strand of 20 μm polyethylene terephthalate. The MicroNet is sutured to both the distal and proximal crowns of the stent platform. Predilatation is required. The CGuard Stent seems to have flexible structure with minimal foreign body reaction.
The CARENET Trial (Carotid Embolic Protection Using MicroNet) compared postinterventional magnetic resonance imaging (MRI) of lesions treated with CGuard implantation to published diffusion-weighted MRI data of non-mesh-covered carotid stents. The incidence of new detected ischemic lesions in MRI was reduced by almost 50% and the average lesion volume per patient was 10 times smaller.14
Gore Carotid Stent
The Gore Carotid Stent (W. L. Gore & Associates) consists of an open-cell NiTi (nitinol) frame supplemented with an outside closed-cell 500 µm lattice of NiTi frame that is covered with Carmeda BioActive Surface Heparin Surface (CBAS; W. L. Gore & Associates). The CBAS surface is a heparin-based surface-modification technology designed to enhance the hemocompatibility of devices for use in contact with blood. Products for which the CBAS technology has been licensed include vascular grafts, heart-lung machines, ventricular assist devices, coronary stents, and hemodialysis catheters. The delivery system (135 cm) of the Gore Carotid Stent is single handed, and it is available in 5 Fr and 6 Fr (hypotube design).
The first-in-human implantation of the Gore Carotid Stent was published by Schönholz and colleagues in the Journal of Endovascular Therapy in 2014.7 They presented initial clinical experience within a case report as part of the company-sponsored Carotid Stent Clinical Study for the Treatment of Carotid Artery Stenosis in Patients at Increased Risk for Events From Carotid Endarterectomy (SCAFFOLD).7 The case report revealed the easy handling and safety implantation of a 6 mm/8 mm x 40 mm Gore Carotid Stent under cerebral protection using a Gore Carotid Filter. They reported conformability to the wall, protection against embolization, and stent patency with normal flow velocities 6 month after the procedure.
The SCAFFOLD trial is a prospective, multicenter, single-arm clinical study that enrolled 312 subjects in up to 50 investigative sites in the United States, Europe, and Japan with a limit of 40 subjects per site.7 Patients were included who were at least 18 years of age, had either a single de novo atherosclerotic or post-endarterectomy restenotic lesions in the internal carotid artery or at the carotid bifurcation, and had either ≥50% stenosis by angiography if symptomatic (stroke, TIA, or transient monocular blindness within 180 days of procedure), or ≥80% stenosis by angiography if asymptomatic. Patients were also required to have either anatomic or medical comorbidities that placed them at high perioperative risk for carotid endarterectomy.
Conclusion: Switching From Single-Layer to Dual-Layer Stent
Although the ideal stent has not yet been developed, new stent designs may be able to close the gap for sustained protection. It remains to be demonstrated whether this promising concept will translate into a reduction of neurologic events associated with CAS. Differences in clinical outcome need to be demonstrated and trial data are still pending. In addition to the impact of stent design, operators must consider appropriate patient selection, anatomic criteria, stenosis morphology (lesion-specific CAS), as well as operator experience. And considering the use of new stent designs, such as hybrid stents or stents with dynamic tapering, the role of embolic protection devices may need to be re-evaluated.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr. Muller-Hulsbeck reports consultancy to Terumo Europe. The remaining authors report no disclosures related to the content herein.
Manuscript received March 22, 2016; provisional acceptance given June 23, 1016; manuscript accepted July 22, 2016.
Corresponding author: Silke Hopf-Jensen, MD, Diakonissenhospital Flensburg, Knutstrasse 1, D-24939 Flensburg, Germany. Email: hopfsi@diako.de
REFERENCES
- Müller-Hülsbeck S, Preuss H, Elhöft H. CAS: which stent for which lesion. J Cardiovasc Surg (Torino). 2009;50(6):767-772.
- Hopf-Jensen S, Marques L, Preiß M, Müller-Hülsbeck S. Lesion-related carotid angioplasty and stenting with closed-cell design without embolic protection devices in high-risk elderly patients-can this concept work out? A single center experience focusing on stent design. Int J Angiol. 2014;23(4):263-270.
- Bosiers M, de Donato G, Deloose K, et al. Does free cell area influence the outcome in carotid artery stenting? Eur J Vasc Endovasc Surg. 2007;33(2):135-141.
- Cremonesi A, Setacci C, Manetti R, et al. Carotid angioplasty and stenting: lesion related treatment strategies. EuroIntervention. 2005;1(3):289-295.
- Lin PH, Bush RL, Peden EK, et al. Carotid artery stenting with neuroprotection: assessing the learning curve and treatment outcome. Am J Surg. 2005;190(6):850-857.
- Schillinger M, Gschwendtner M, Reimers B, et al. Does carotid stent cell design matter? Stroke. 2008;39(3):905-909.
- Schönholz C, Yamada R, Montgomery W, Brothers T, Guimaraes M. First-in-man implantation of a new hybrid carotid stent to prevent periprocedural neurological events during carotid artery stenting. J Endovasc Ther. 2014;21(4):601-604.
- Tietke MW, Kerby T, Alfke K, et al. Complication rate in unprotected carotid artery stenting with closed-cell stents. Neuroradiology. 2010;52(7):611-618.
- Wissgott C, Schmidt W, Behrens P, Brandt C, Schmitz KP, Andresen R. Experimental investigation of modern and established carotid stents. Rofo. 2014;186(2):157-165.
- Bosiers M, de Donato G, Deloose K, et al. Does free cell area influence the outcome in carotid artery stenting? Eur J Vasc Endovasc Surg. 2007;33(2):135-141.
- Müller-Hülsbeck S, Schäfer PJ, Charalambous N, Schaffner SR, Heller M, Jahnke T. Comparison of carotid stents: an in-vitro experiment focusing on stent design. J Endovasc Ther. 2009;16(2):168-177.
- Müller-Hülsbeck S, Gühne A, Tsokos M, et al. Stent-protected carotid angioplasty using a membrane stent: a comparative cadaver study. Cardiovasc Intervent Radiol. 2006;29(4):630-636.
- Müller-Hülsbeck S, Hüsler EJ, Schaffner SR, et al. An in vitro analysis of a carotid artery stent with a protective porous membrane. J Vasc Interv Radiol. 2004;15(11):1295-1305.
- Schofer J, Musiałek P, Bijuklic K, et al. A prospective, multicenter study of a novel mesh-covered carotid stent: the CGuard CARENET Trial (carotid embolic protection using MicroNet). JACC Cardiovasc Interv. 2015;8(9):1229-1234.
- Hopf-Jensen S, Marques L, Preiß M, Müller-Hülsbeck S. Initial clinical experience with the micromesh roadsaver carotid artery stent for the treatment of patients with symptomatic carotid artery disease. J Endovasc Ther. 2015;22(2):220-225.
- Kedev S, Petkoska D, Zafirovska B, Vasilev I, Bertrand OF. Safety of slender 5 Fr transradial approach for carotid artery stenting with a novel nitinol double-layer micromesh stent. Am J Cardiol. 2015;116(6):977-981.
- Bosiers M, Deloose K, Torsello G, et al. The CLEAR-ROAD study: evaluation of a new dual layer micromesh stent system for the carotid artery. EuroIntervention. 2016;12(5):e671-676.

