DISRUPT PAD III Update: Intravascular Lithotripsy for PAD
In an on-demand session from the International Symposium on Endovascular Therapy (ISET) 2021, Andrew Holden, MBChB, Auckland City Hospital in Auckland, New Zealand, updated listeners on the DISRUPT PAD III randomized clinical trial and observational study.
Calcified peripheral arterial disease (PAD) is a common and increasing problem with not-great solutions, he said. Calcified arteries have reduced compliance that results in poor balloon expansion and a high incidence of residual stenosis, dissection, and acute procedural failure. Atherectomy is another option, but is associated with distal embolization, dissection and perforation.
“We know that patients with moderate to severe calcification have often been excluded from endovascular treatment trials, so we've had, up till now, little evidence on the best method to treat this challenging population,” Holden explained.
Enter lithotripsy. It’s been available for over 30 years for the treatment of kidney stones, which provides good safety data, said Dr. Holden.
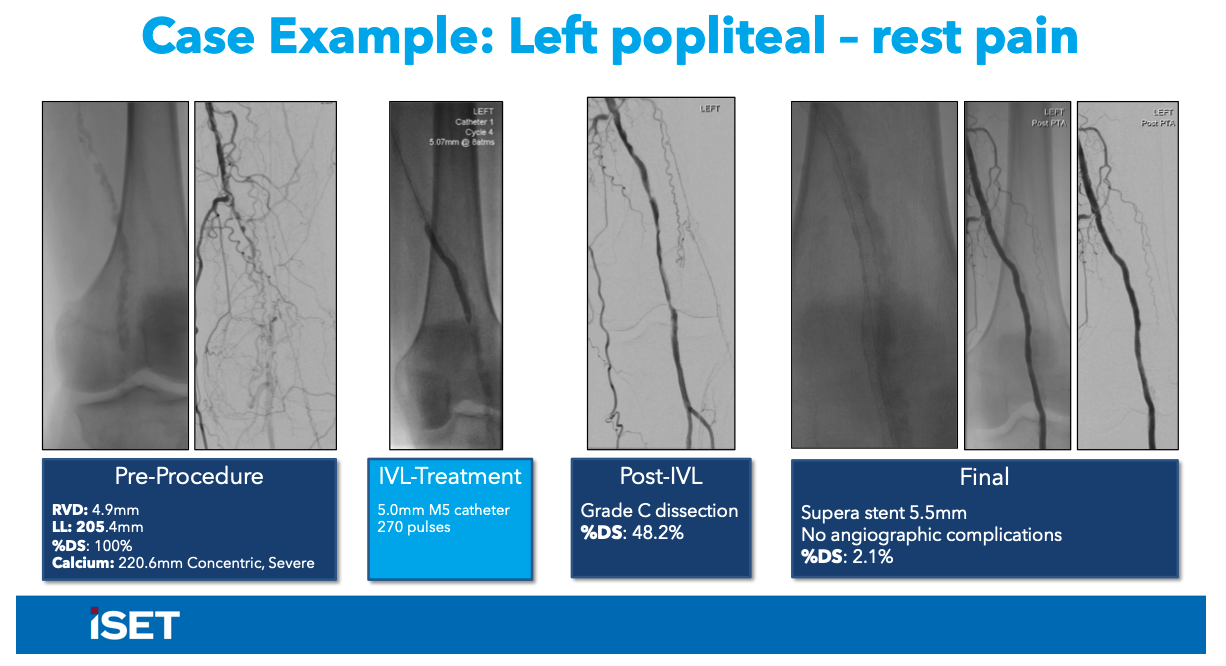
Intravascular lithotripsy (IVL; Shockwave Medical) using uses miniaturized and arrayed lithotripsy emitters for localized lithotripsy at the side of the vascular calcium, fracturing intimal and medial calcium to facilitate safe expansion of the vessel. Single-arm studies have reported promising results with IVL. DISRUPT III PAD is the first randomized trial of peripheral IVL and the largest-ever randomized trial in calcified lesions.
DISRUPT PAD III tested IVL in 306 patients with moderate-severe calcification in de novo femoropopliteal arteries. Participants were from 45 clinical sites in the U.S., European Union, and New Zealand. The study compared acute outcomes in patients receiving vessel preparation with IVL (n=153) or percutaneous transluminal angioplasty (PTA) (n=153), both used prior to drug-coated balloon (DCB) treatment.
The primary effectiveness endpoint of procedural success, defined as core-lab adjudicated residual stenosis ≤30% without flow-limiting dissection prior to DCB or stenting, was seen in 66% of the IVL arm and in 50% of the PTA arm (P=.007).
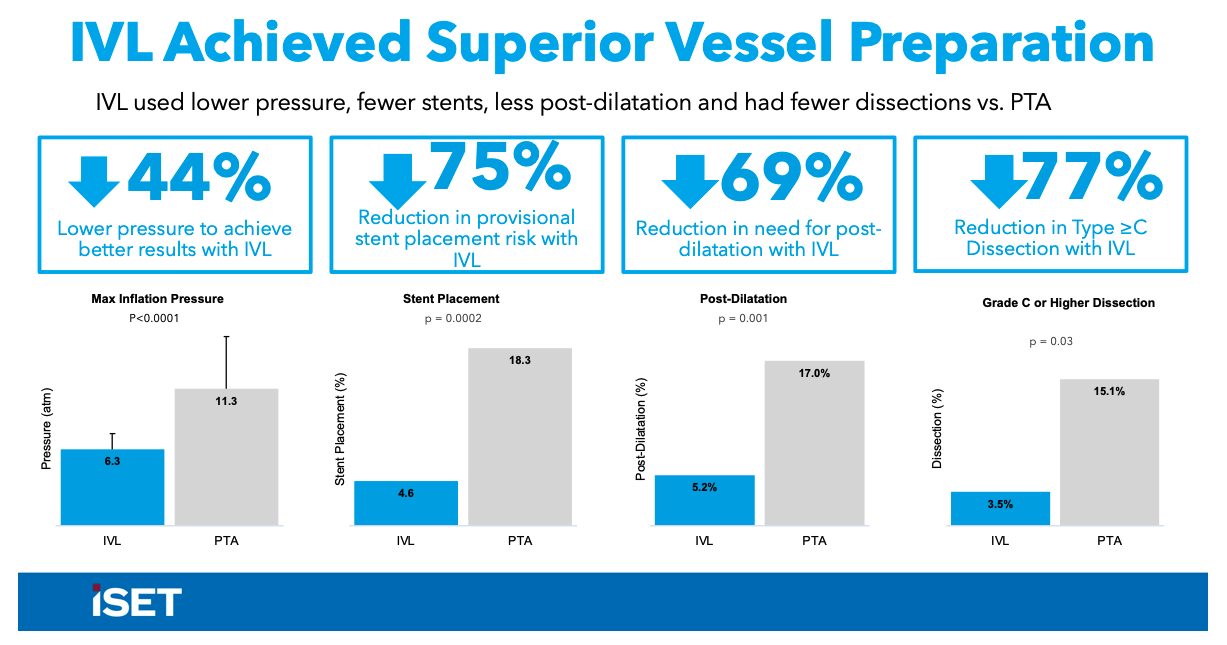
“We can see that IVL achieved a number of features to indicate superior vessel preparation,” said Dr. Holden.
Dr. Holden also shared some new data from the DISRUPT III PAD Observational Study, while plans to enroll 1500 real-world patients requiring treatment of calcified, stenotic, peripheral arteries. Holden presented some subgroup data on 254 long lesions (>15 cm) treated with IVL that showed that in these long and heavily calcified lesions, IVL can achieve low residual stenosis with no distal embolization, abrupt closure, or reflow at the end of the procedure.