

Interview With Nathan Fagan, MD: Using the ARTIS icono in the Interventional Pediatric Space
Interventional Radiologist
Nationwide Children's Hospital
Columbus, Ohio
Vascular Disease Management speaks with Interventional Radiologist Nathan Fagan, MD, from Nationwide Children’s Hospital in Columbus, Ohio, about using the ARTIS icono in the interventional pediatric space.
When we think about pediatric interventional procedures, the first thing that comes to mind is limiting dose and contrast. Can you tell us about your team’s approach at Nationwide?
Given that we are a major, freestanding pediatric hospital, radiation and contrast dose delivered to the patient is always at the forefront of our mind. Limiting the patient dose begins at diagnosis and continues through treatment. In pediatrics, we will often use ultrasound as our imaging of choice to evaluate for disease processes. Take, for example, simple appendicitis. Using ultrasound in this situation is something that is not commonly performed at adult facilities that happen to be seeing pediatric patients. High-quality pediatric ultrasound requires skilled ultrasound technologists who perform the exams routinely. Because these technologists are usually not at adult facilities, computed tomography (CT) is the first-line imaging technique. At pediatric institutions like Nationwide Children’s, ultrasound is often the only exam required for something like simple appendicitis. You can imagine how, over time, this would cumulatively decrease both radiation and contrast dose delivered to not just a single patient, but the entire pediatric population of a community.
If ultrasound can’t cut it and cross-sectional imaging is required, we have worked very hard to maximize magnetic resonance imaging (MRI) use and dial back our CT radiation dose. We are always on the hunt for new technology or techniques that allow us to decrease the radiation delivered during CT while maintaining diagnostic quality. We have also built our MRI protocols such that it can replace CT in some instances. While you should never obstruct a patient from having a study over radiation, we are constantly asking ourselves, “Do they need this?” and “Is there another option?”
Keeping with the same theme, our approach to treatment is different in pediatric interventional radiology. Outside of vascular work, our main workhorse for image guidance is ultrasound. Much like on the diagnostic side, in certain straightforward cases, ultrasound is the only modality used. In more advanced cases where fluoroscopy is required, we have worked with industry to develop protocols and leverage new technologies that allow us to perform our job faster, safer, and with less contrast and radiation. The concept of ALARA (As Low As Reasonably Achievable) is something you will often hear when discussing pediatric radiology. At a children’s hospital like Nationwide Children’s, it’s not just an acronym, it’s an ethos that is built into the very culture of the radiology department.
How does imaging impact your ability to treat pediatric patients safer?
Image quality plays a vital role in our ability to treat pediatric patients in interventional radiology. It is because of this that using techniques and technology that reduce radiation dose while maintaining image quality are of great importance. We treat a wider range of patient sizes in pediatrics, from a tiny infant to a 17-year-old athlete. While this may seem obvious to some, it is these large swings in patient size that make keeping uniform image quality difficult. Therefore, partnering with vendors like Siemens Healthineers, who takes a vested interest in pediatrics, is so important. Together, we can tune the systems and their protocols to help reduce the dose while maintaining image quality. This way, no matter what size patient walks through our door, we know we can rely on our equipment to produce the images we need to get the job done at the lowest dose possible.
syngo DynaCT has become the gold standard for many applications in adult interventional radiology. What role does it play in pediatric intervention?
As it stands, syngo DynaCT is not used as widely in the pediatric population. While it is routine in many adult disease processes, it is mostly used as a problem-solving tool in pediatrics. The main reason why it is limited to problem-solving only in pediatrics is because of the increased dose. In many situations, we can get away with standard 2D fluoro. Where it does become important is in cases where we are trying to define complex vascular anatomy or just can’t see what we need to with standard 2D fluoroscopy. Some examples include complex neurovascular or portal venous hypertension cases. In these cases, syngo DynaCT often allows us to get the information we are looking for that we otherwise wouldn’t be able to or would require multiple 2D runs. So, while the dose of one syngo DynaCT alone is higher than 2D fluoro, the overall dose is decreased. And though it may only be used in limited situations currently, as the technology improves, I only see its use increasing in pediatric interventional radiology.
How are you utilizing MR and CT datasets with fluoroscopy to improve patient outcomes?
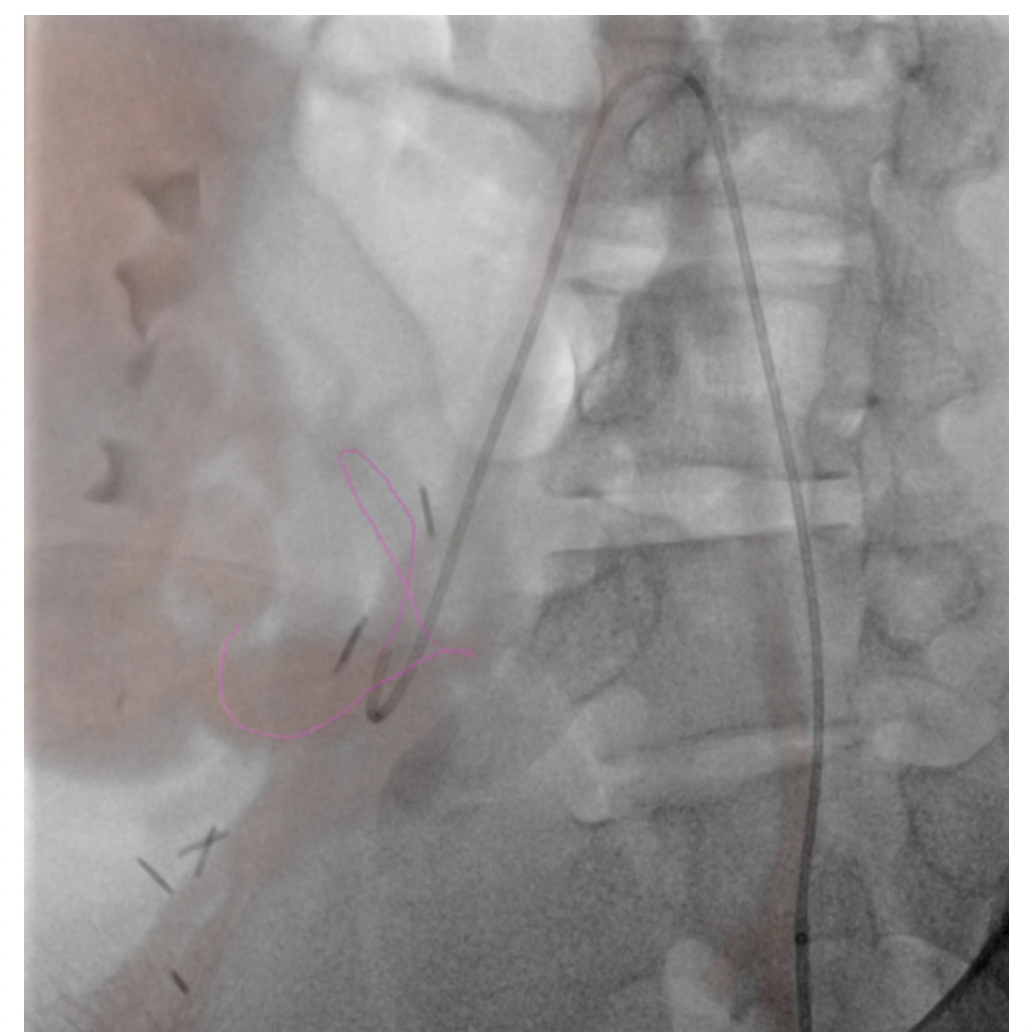
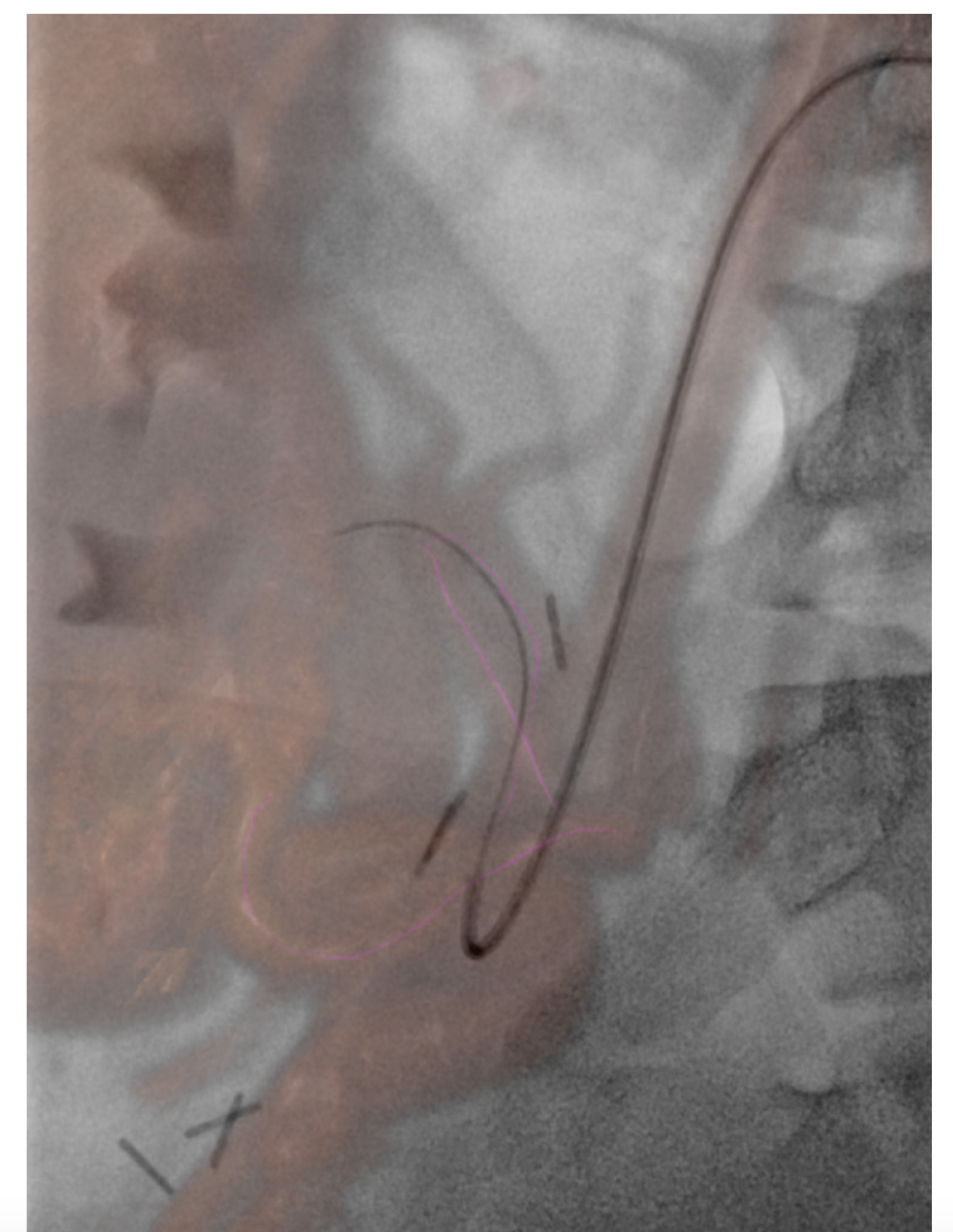
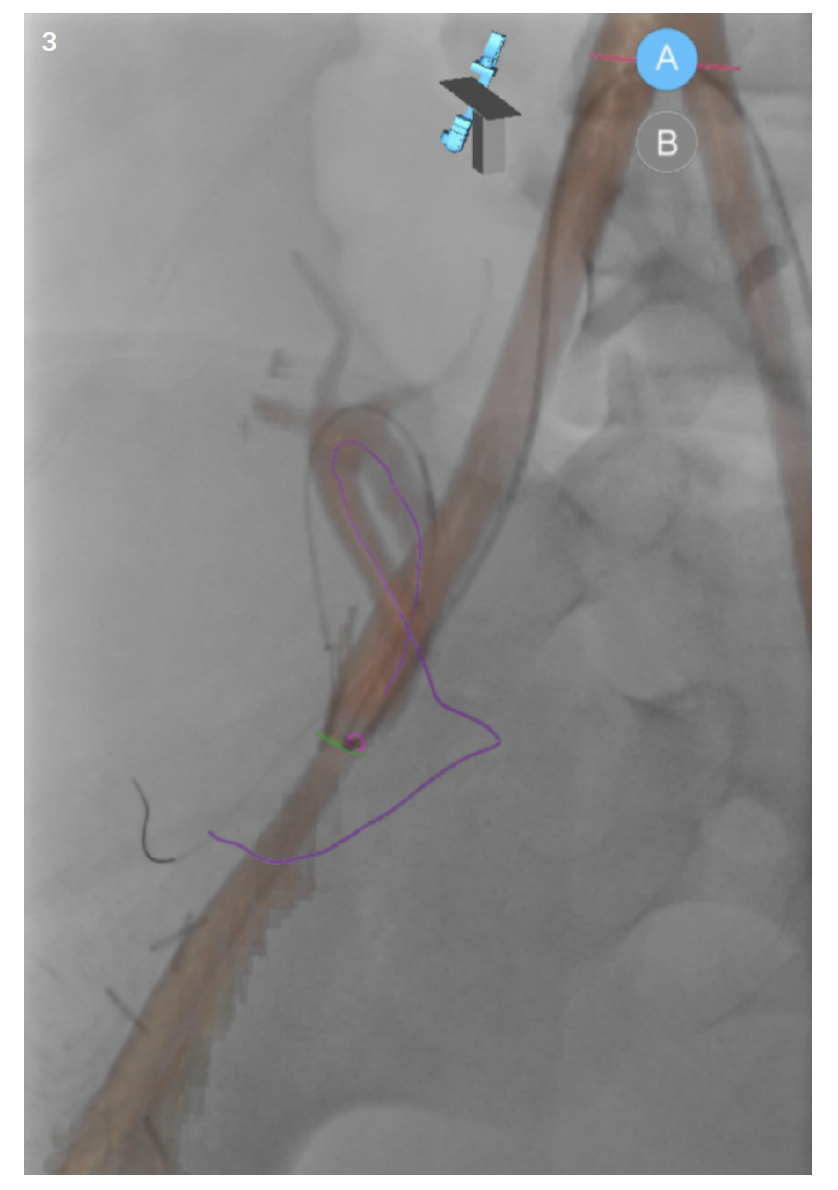
In pediatrics, MR and CT datasets are mainly used for fusion to assist with intraprocedural guidance and road mapping. As with most things in pediatrics, its use is currently limited. It is, however, an area of interest that is growing among the community. Sometimes patient vascular anatomy is complex; other times, patient size makes navigating even normal anatomy difficult. Though most interventionalists would be able to perform a complicated case without assistance, the datasets have potential to help decrease patient radiation and contrast dose in the hands of even the most skilled users. This may be able to be accomplished through use of the patient’s prior cross-sectional imaging to create 3D roadmaps on the day of treatment. While it may not be a “perfect” one-to-one recreation of the patient’s anatomy, the roadmap created and overlaid on live fluoroscopy is often more than sufficient (Figure 1). In complex cases, the roadmap created will at the very least give the interventionalist a better approximation of where a tortuous vessel’s origin might be in the 3D space (Figure 2). And if the interventionalist has a better idea of the vessel origin, they may be able to select it faster, thus limiting patient radiation and contrast dose. And while the same software can be used for even more advanced techniques such as organ segmenting, it is straightforward to use. It doesn’t matter how useful or “nifty” you think something is if it is unreliable and cumbersome to implement. Once the interventionalist understands Siemens’ simple and intuitive workflow, use of prior imaging in this manner is something that can easily be done with little effort and time. The other thing to keep in mind is with the simplified workflow; if whatever overlay was created using the patient’s prior imaging is not helpful or is a hinderance, it can easily be turned off. While it may seem counterintuitive, the ability to easily turn off an advanced feature if it is not serving its purpose is just as important as to not waste time in the suite doing unnecessary troubleshooting.

Can you elaborate on how you utilize navigational software to help with pediatric interventions?
Navigational software is most useful in pediatric musculoskeletal interventions. If there is a small lesion in a difficult-to-get-to place and CT is either unavailable or unreliable, it is a wonderful tool. A safe needle trajectory can be preplanned off the original MR or CT. Once planned, it then can be fused to live fluoroscopy and the system will generate a virtual guide for the needle. By starting with a skin entry point then moving to a progression view, the needle can be safely guided down along the planned path to the area of interest. I place a high value on having a plan B or C if your original plan is not working. Siemens needle guidance software accomplishes just that. If the plan made from the patient’s original imaging is not working, the case can be easily troubleshot with syngo DynaCT. A syngo DynaCT can be performed, and a new trajectory can be planned so the case can continue. Troubleshooting with syngo DynaCT is made even easier with the new ARTIS icono. The technology allows for speedy acquisition at a reasonably low dose so if the original plan isn’t working, abandoning it and starting over with syngo DynaCT so that the case can safely be performed is a more palatable option.
What would you want your peers to know about the ARTIS icono technology that is maybe under-discussed? Or is there something that surprised you?
From the perspective of a pediatric interventional radiologist, the ARTIS icono has a lot of technology that surprises me and I think is underutilized. While some of the tools and features may be well known by adult interventionalists, much of it is new to me. Things as simple as utilizing metal artifact reduction software to clean up syngo DynaCT angio runs to as complex as using multimodality fusion. The system is even able to interface with newer simulation platforms to help train residents and fellows. It’s all new and enticing.
In pediatrics, we are accustomed to getting by with the bare minimum. Technology like this can really change the game if you know when and how to use it. With that being said, I think the most important and surprising thing about the ARTIS icono is not the technology itself, but the support from Siemens Healthineers’ staff. The technology is more than capable. It is so capable, in fact, that it is hard to keep up. But Siemens Healthineers’ staff knows it inside and out. They will allow you to harness the true power of the technology and use it in situations you never thought of to unlock its full potential.
