


Rectus Sheath Hematoma Embolization: When, Why, and for Whom?
VASCULAR DISEASE MANAGEMENT. 2022;19(6):E110-E112
Abstract
Rectus sheath hematoma is an uncommon and often misdiagnosed disease. Although it is usually a self-limiting condition, it can present as a life-threatening emergency. Three treatment modalities are often used: conservative treatment, transarterial embolization, and surgical ligation of bleeding vessels. Unfortunately, there is no current consensus to guide the decision-making process for treating these complex patients.
Introduction
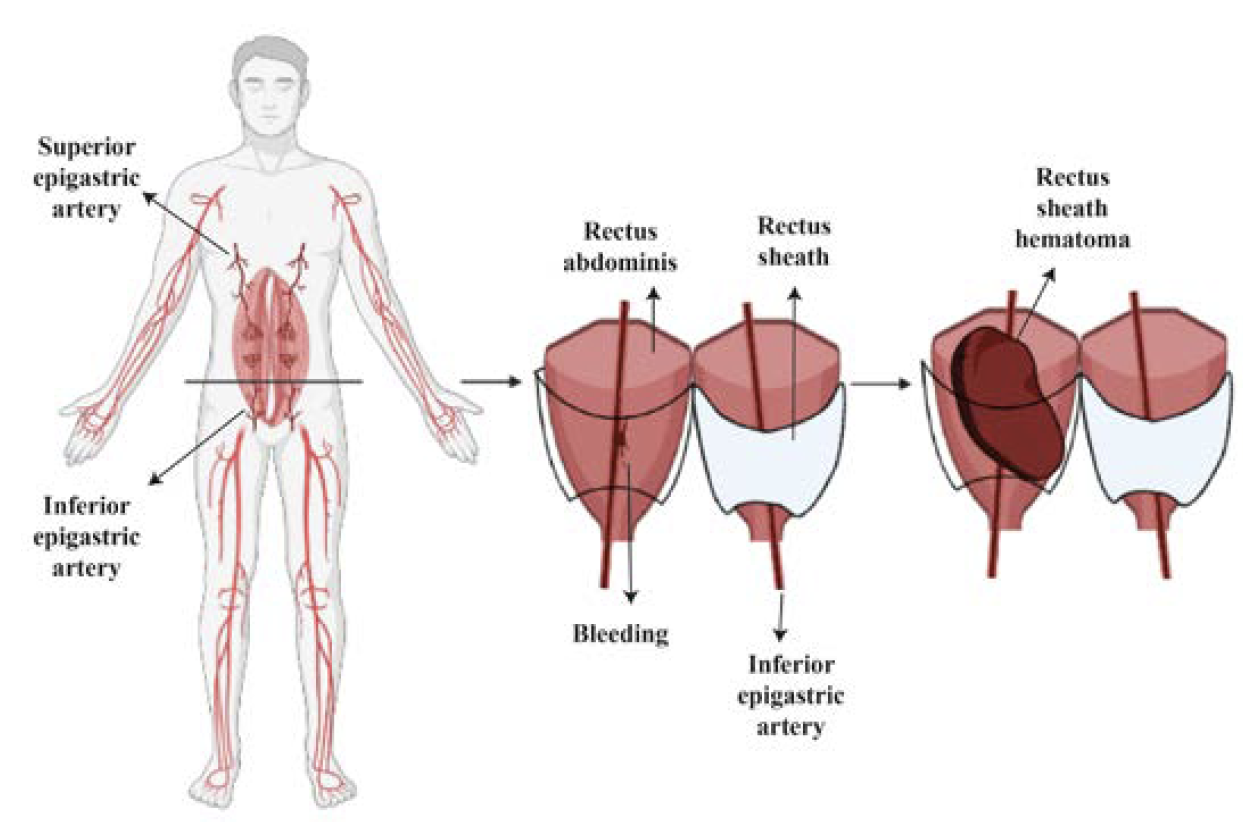
Rectus sheath hematoma (RSH) results from the bleeding of the epigastric artery or one of its branches into the rectus sheath1 (Figure 1). RSH accounts for less than 2% of patients presenting with acute abdominal pain syndromes.2 Unfortunately, it is frequently misdiagnosed, leading to increased morbidity and a reported mortality rate of up to 25%.3
RSH can be caused by direct abdominal trauma and, less commonly, can occur spontaneously.4 The mean age at presentation varies between 45 to 70. Potential risk factors identified to date include age, direct abdominal trauma, strong contraction of the rectus, iatrogenic vascular injuries after abdominal wall procedures, anticoagulation, pregnancy, gender (women are more commonly affected), and chronic use of corticosteroids.5
Abdominal pain is the most common symptom at presentation, along with a palpable abdominal wall mass.3 However, the patient’s presentation may vary significantly, depending on the size of the hematoma and the functional status of the patient. Treatment modalities include invasive procedures and conservative management. Thus, while stable patients with self-limiting RSH can benefit from conservative treatment, patients with active blood extravasation on computed tomography (CT), expanding RSH, or who are hemodynamically unstable often require intervention.6 However, the decision-making process is not always so simple and often represents a clinical challenge. Unfortunately, there is no current consensus to guide treatment selection for these complex patients.
When, Why, and for Whom?
Conservative treatment is the most common therapy for RSH because it is usually self-limited.3 Therefore, the first step to take is to assess the patient’s hemodynamic status. Hemodynamically stable patients will probably benefit from conservative treatment, and an ultrasound is often enough to make the diagnosis.7 Anticoagulants should be discontinued, and appropriate administration of vitamin K, fresh frozen plasma, and platelet transfusion can successfully arrest progression of RSH.8 In line with this, Berná et al have demonstrated a high success rate after conservative treatment, even in patients with large hematomas and hemodynamic changes.9
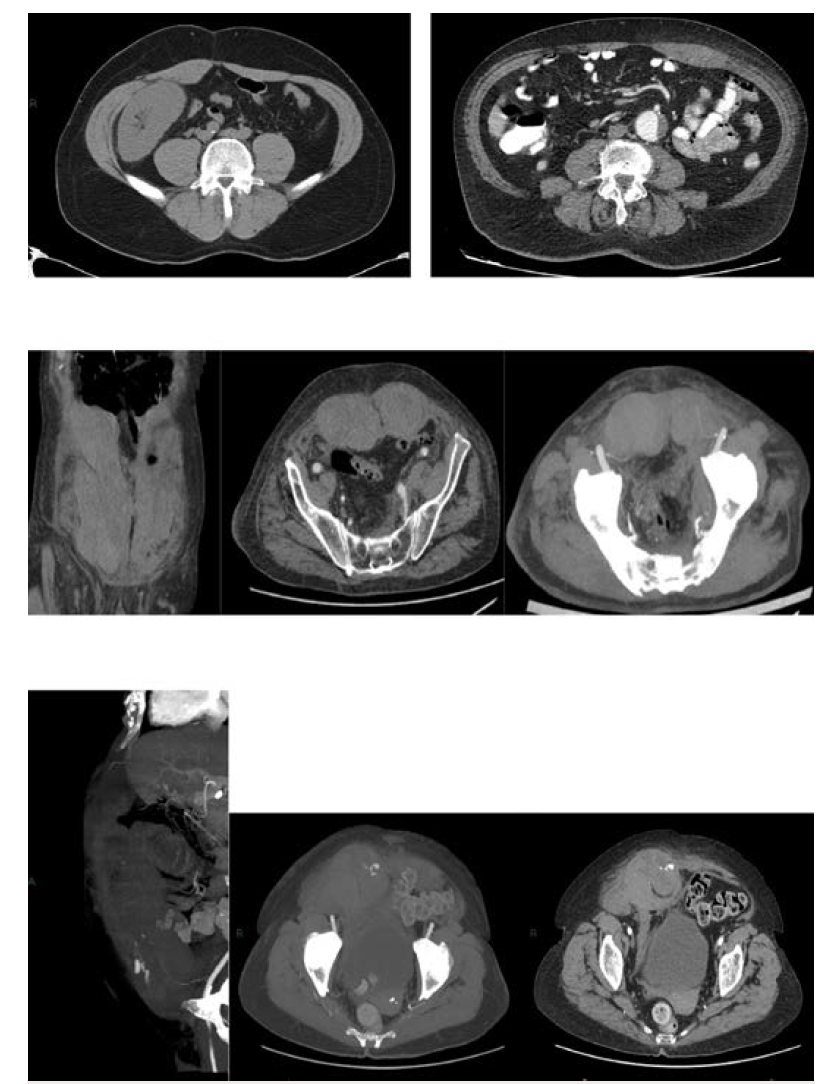
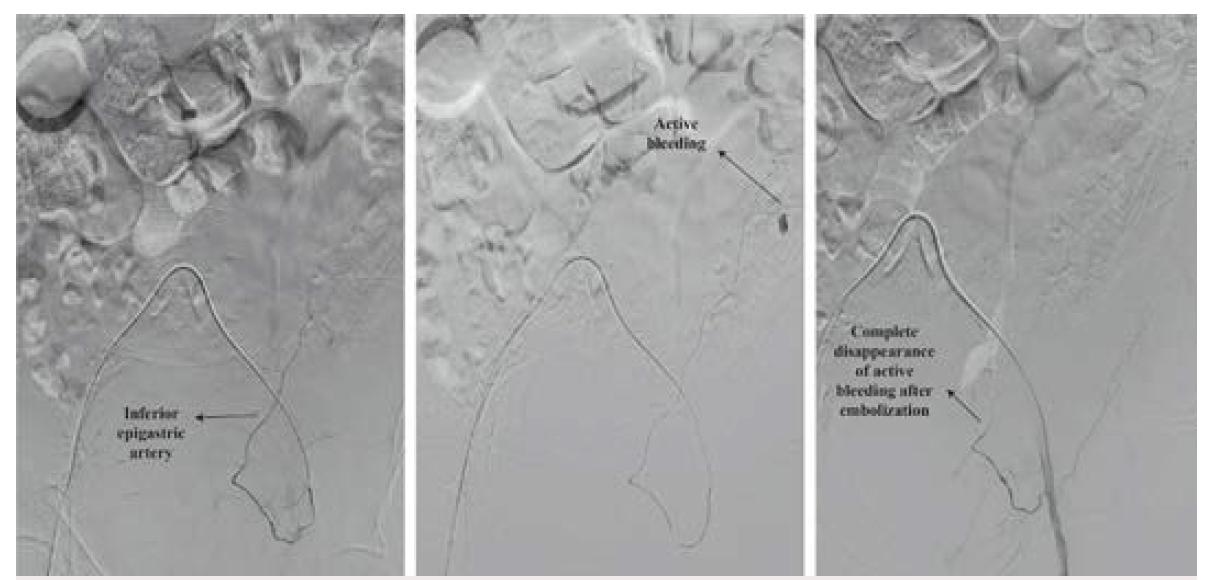
On the other hand, intravenous fluid resuscitation should be started in hemodynamically unstable patients. Red blood cell (RBC) transfusion depends on the hemodynamic status and presence of comorbid conditions.6 In an acutely hemorrhaging patient, transfusions should not be delayed awaiting laboratory tests. In addition, those patients who become hemodynamically stable with fluid resuscitation are managed as stable patients (transfuse if hemoglobin is <7g/dL).10 CT angiography must be performed as soon as possible. CT can help classify RSH according to the Berná classification as well as show evidence of active blood extravasation. The Berná grading system classifies RSH into 3 types: Type I, intramuscular and unilateral hematoma without hemodynamic compromise; Type II, unilateral or bilateral hematoma with blood between muscle and transversalis fascia, with a possible decrease in hematocrit; and Type III, hematoma associated with hemodynamic instability and with blood extending to the peritoneum and prevesical space6 (Figure 2). Active extravasation on CT angiography and a hematoma volume of >1000 mL to 1300 mL have been previously identified as predictors of conservative treatment failure.6,11 Therefore, the presence of active hemorrhage on CT angiography and/or hematoma (Type III) should promptly trigger endovascular arterial embolization or surgery. Historically, surgical ligation of the bleeding epigastric vessels was the treatment for uncontrolled RSH. However, it is well known that this technique is severely limited by the difficulties in localizing and ligating the bleeding vessel within the hematoma. Open surgery or guided drainage of RSH should be avoided when possible because it can diminish the potential tamponade effect of the rectus sheath.12 In line with this, surgery must be reserved for draining infected RSH and for controlling the bleeding in those health centers without hemodynamic and interventionist units. Selective arterial embolization, on the other hand, has been accepted as an effective and safe method for treating acute bleeding in patients with RSH.13 (Figure 3). Diamantopoulos et al reported 95.2% and 95% technical and clinical success, respectively, without rebleeding after epigastric artery embolization.14 Similarly, in a study by Contrella et al, the procedure only had to be repeated in 3 of the 32 patients who underwent endovascular embolization. In addition, no patient underwent surgery for RSH.6
Among patients with clear indications for conservative and invasive treatment, there is a complex group of patients in whom the choice of treatment must be based on several factors. For example, it has been proven that in cases of persistent hemodynamic instability despite intravenous resuscitation and/or the need of more than 4 RBC units, an invasive treatment should not be delayed.6,11,15 Similarly, care should be maximized in patients with changes ≥10 and ≥4g/dL in hematocrit and hemoglobin, respectively, as they have been recognized as predictors of failure after conservative treatment.11 The Berná grading system is also useful for stratifying patients with RSH. While patients with Type III RSH should undergo an invasive treatment, those with Type I RSH will benefit from conservative treatment. Closer follow-up is reasonable in patients with Type II RSH, and in case of a minimal deterioration in the hemodynamic status, invasive treatment should not wait.1 Older individuals are more likely than younger individuals to be affected by RSH due to a higher use of anticoagulant and antiaggregant drugs as well as a lower elasticity of epigastric vessels.16 Women are also more commonly affected, most likely due to less support from the rectal muscle mass compared with men.5 Other conditions, such as chronic corticosteroid use, have also been associated with RSH, probably due to interaction with coagulation factors.17
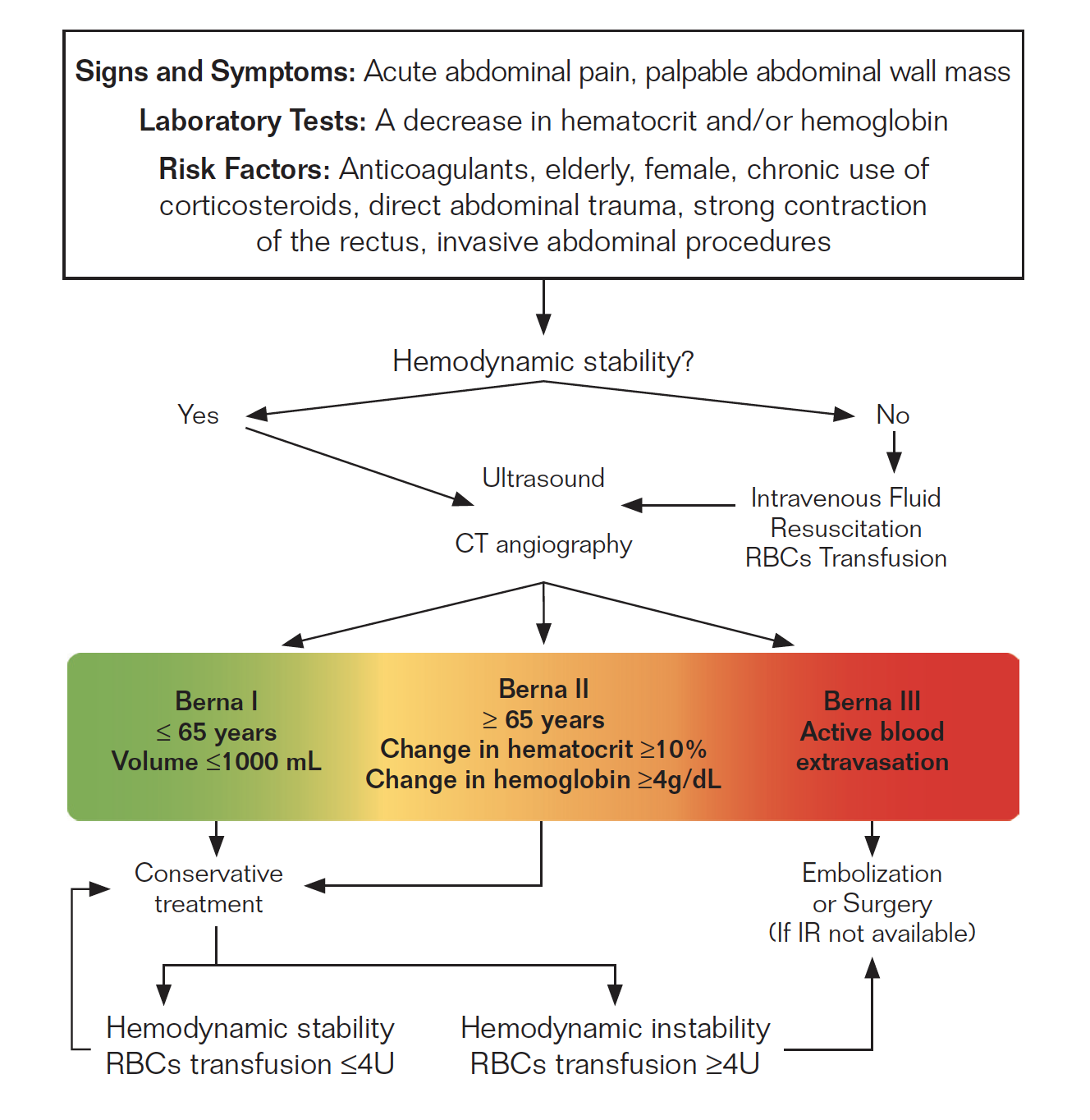
To date, there is a lack of consensus and algorithms to guide the decision-making process in the emergent setting of patients with RSH. For this reason, we have previously proposed an algorithm for RSH treatment based on an artificial neural network.11 It aims to identify, with a high degree of accuracy, those patients at risk of progressive RSH in whom early intervention could prevent clinical deterioration. We stratified patients into 3 groups: low, medium, and high risk. The group at low risk are represented by young and hemodynamically stable patients with limited RSH (Type I RSH and/or volume ≤ 1000 mL). This group can be safely managed with conservative treatment. The group at high risk are those patients with Type III RSH and/or hemodynamically unstable patients. This group will benefit from prompt intervention. Endovascular treatment should be prioritized over surgery whenever possible and available. Finally, the moderate risk group consists of older patients with changes in laboratory studies (hematocrit and hemoglobin) and/or Type II RSH. Intravenous fluid resuscitation and transfusions (if needed) should be instituted as early as possible in this group. Failure of this compensation attempt or the need for more than 4 RBC units should trigger immediate intervention (Figure 4).
Conclusion
RSH is a rare disease with high morbidity and mortality. Although uncommon, RSH should be considered a potential cause of abdominal pain, especially in older patients, anticoagulated, with a history of abdominal trauma or strong contraction of the rectus. Both conservative and invasive management are valid treatment modalities depending on the clinical presentation of the patient. In addition, endovascular interventions represent an attractive minimally invasive alternative with a high success rate and reduced morbidity.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript accepted May 23, 2022.
Address for correspondence: Patricio Méndez, MD, Department of Interventional Radiology, Hospital Alemán of Buenos Aires, Av. Pueyrredón 1640, CP 1118, Buenos Aires, Argentina Email: pmendez@hospitalaleman.com
Related Articles
Rectus Sheath Hematoma as a Complication of Ablation of Atrial Fibrillation
REFERENCES
1. Liao E-D, Puckett Y. A proposed algorithm on the modern management of rectus sheath hematoma: a literature review. Cureus. 2021;13(11):e20008. doi:10.7759/cureus.20008
2. Cherry WB, Mueller PS. Rectus sheath hematoma: review of 126 cases at a single institution. Medicine (Baltimore). 2006;85(2):105-110. doi:10.1097/01.md.0000216818.13067.5a
3. Hatjipetrou A, Anyfantakis D, Kastanakis M. Rectus sheath hematoma: a review of the literature. Int J Surg. 2015;13:267-271. doi:10.1016/j.ijsu.2014.12.015
4. Fitzgerald JEF, Fitzgerald LA, Anderson FE, Acheson AG. The changing nature of rectus sheath haematoma: case series and literature review. Int J Surg. 2009;7(2):150-154. doi:10.1016/j.ijsu.2009.01.007
5. Buffone A, Basile G, Costanzo M, et al. Management of patients with rectus sheath hematoma: personal experience. J Formos Med Assoc. 2015;114(7):647-651. doi:10.1016/j.jfma.2013.04.016
6. Contrella BN, Park AW, Wilkins LR, Sheeran D, Hassinger TE, Angle JF. Spontaneous rectus sheath hematoma: factors predictive of conservative management failure. J Vasc Interv Radiol. 2020;31(2):323-330. doi:10.1016/j.jvir.2019.06.009
7. Bello G, Blanco P. Giant rectus sheath hematoma. Ultrasound J. 2019;11(1):13. doi:10.1186/s13089-019-0129-4
8. Smithson A, Ruiz J, Perello R, Valverde M, Ramos J, Garzo L. Diagnostic and management of spontaneous rectus sheath hematoma. Eur J Intern Med. 2013;24(6):579-582. doi:10.1016/j.ejim.2013.02.016
9. Berná JD, Zuazu I, Madrigal M, García-Medina V, Fernández C, Guirado F. Conservative treatment of large rectus sheath hematoma in patients undergoing anticoagulant therapy. Abdom Imaging. 2000;25(3):230-234. doi:10.1007/s002610000007
10. Barkun AN, Almadi M, Kuipers EJ, et al. Management of nonvariceal upper gastrointestinal bleeding: guideline recommendations from the International Consensus Group. Ann Intern Med. 2019;171(11):805-822. doi:10.7326/M19-1795
11. Angeramo CA, Méndez P, Eyheremendy EP, Schlottmann F. Rectus sheath hematoma: conservative, endovascular or surgical treatment? A single-center artificial neural network analysis. Eur J Trauma Emerg Surg. 2022;48(3):2157-2164. doi:10.1007/s00068-021-01854-2
12. Donaldson J, Knowles CH, Clark SK, Renfrew I, Lobo MD. Rectus sheath haematoma associated with low molecular weight heparin: a case series. Ann R Coll Surg Engl. 2007;89(3):309-312. doi:10.1308/003588407X179152
13. Berná JD, Garcia-Medina V, Guirao J, Garcia-Medina J. Rectus sheath hematoma: diagnostic classification by CT. Abdom Imaging. 1996;21(1):62-64. doi:10.1007/s002619900011
14. Diamantopoulos A, Mulholland D, Katsanos K, et al. Transcatheter embolization of the inferior epigastric artery: technique and clinical outcomes. Vasc Endovascular Surg. 2021;55(3):221-227. doi:10.1177/1538574420980576
15. Popov M, Sotiriadis C, Gay F, et al. Spontaneous intramuscular hematomas of the abdomen and pelvis: a new multilevel algorithm to direct transarterial embolization and patient management. Cardiovasc Intervent Radiol. 2017;40(4):537-545. doi:10.1007/s00270-017-1590-8
16. Gündeş E, Çetin DA, Aday U, et al. Spontaneous rectus sheath hematoma in cardiac in patients: a single-center experience. Ulus Travma Acil Cerrahi Derg. 2017;23(6):483-488. doi:10.5505/tjtes.2017.67672
17. Azharuddin M, Gupta M, Maniar M. Subcutaneous heparin leads to rectus sheath hematoma: a rare complication. Cureus. 2018;10(6):e2769. doi:10.7759/cureus.2769
