


Review of Embolic Protection Devices in Percutaneous Peripheral Intervention
Abstract
The use of embolic protection devices (EPDs) in infrainguinal interventions continues to be debated, despite common use in carotid and coronary revascularization. This review discusses the current data available for debris burden of different atherectomy devices and efficacy of infrainguinal EPD. While clinically significant embolization does not occur frequently enough to justify routine application, EPD use during atherectomy has been demonstrated to have a high safety profile and improved clinical outcomes. Deployment of EPDs should be considered when using atherectomy in the setting of heavy plaque burden, lesions >140 mm in length, moderate to severe calcification, chronic total occlusion, or limited runoff vessels.
VASCULAR DISEASE MANAGEMENT 2021;18(6):E95-E98
Key words: atherectomy, distal embolization, embolic protection devices, infrainguinal Interventions
Introduction
Peripheral arterial disease (PAD) can lead to ischemia, compromise in ambulatory function, and risk of limb loss. Historically, open surgical treatments such as bypass were the only interventions available, in conjunction with smoking cessation, exercise, and medications. With advancing technologies and techniques, endovascular interventions such as angioplasty, stenting, and atherectomy are now commonly used to treat peripheral vascular disease. The determination to treat with an open or endovascular approach may be guided by TransAtlantic Inter-Society Consensus (TASC) II criteria; however, patient preference and operator expertise also help guide local treatment algorithms. While angioplasty and stenting can improve vessel diameter, atherectomy devices are designed to debulk atherosclerotic plaque burden, theoretically resulting in improved distal flow. Endovascular atherectomy devices include directional, rotational, laser, and orbital atherectomy options, each with different benefits and risk profiles.
Distal embolization (DE), characterized by dislodgment and downstream migration of atherosclerotic fragments and debris, is a fairly common occurrence in various vascular beds, including coronary, renal, and peripheral arteries. Clinical significance of DE depends on the amount and size of debris and the sensitivity of the organ perfused.1 DE occurs in 1%-20% of iliac, femoral, and popliteal percutaneous peripheral interventions (PPIs).2 Clinical presentation of DE varies from asymptomatic to limb-threatening ischemia requiring revascularization or amputation. With mechanical atherectomy, the DEFINITIVE LE study identified clinically significant embolus in 3.8% of cases.3 Embolic protection devices (EPDs) utilize innovative strategies to capture emboli before they travel to distal branches. Although EPD use is commonly accepted in carotid and coronary revascularization, application in lower-extremity interventions has been debated due to the uncertain significance of embolic events, added cost, and risk of EPD-related complications. This review discusses the current data available for the debris burden of different atherectomy devices and the safety and efficacy of EPD in PPI.
Embolic Protection Device Options
Available EPDs include distal occlusion devices, proximal occlusion devices, and distal embolic filters. Distal embolic filters, including SpiderFX (Medtronic), EmboShield NAV6 (Abbott Vascular), and Wirion EPS (Cardiovascular Systems, Inc [CSI]), are most commonly used in PPIs. A self-expanding filter bag on a microwire is delivered in a collapsed state within a delivery sheath, and is intended to be deployed 2.5-3.0 cm downstream of the target atherectomy site. Although most filter pore sizes are around 100 µm, filters can capture particles <100 µm while maintaining anterograde perfusion due to a reduced functional pore size from accumulation of captured debris.1 SpiderFX, EmboShield NAV6, and Wirion EPS distal embolic filters have been approved by the United States Food and Drug Administration (FDA) for above-the-knee lower-extremity arteries.
With distal occlusion devices, such as GuardWire (Medtronic) and TriActiv FX (Kensey Nash), a distal balloon occlusion impedes debris flow downstream while residual embolic material is aspirated prior to balloon removal. Meanwhile, proximal occlusion devices, such as Proxis (Abbott), utilize proximal balloon inflation to obstruct the vessel proximal to the plaque, causing flow cessation and allowing aspiration to remove debris. However, both distal and proximal occlusion devices are only FDA approved for saphenous vein graft use and use for peripheral interventions is considered off label.1
Safety and efficacy of EPDs. The DEEP EMBOLI registry is a single-center, prospective, open-label registry studying DE during intervention with Elite excimer laser ablative therapy (Spectranetics) and SpiderFX EPD. Out of 20 patients, 28 lesions were electively treated for infrainguinal occlusive disease. In addition to laser atherectomy, adjunctive percutaneous transluminal angioplasty (PTA) occurred in 27 lesions (96.4%), and stenting was done in 17 lesions (60.7%). Primary endpoint (<30% residual luminal narrowing or <20 mm Hg gradient) was met in all cases. All EPDs were deployed and retrieved without complications. Macrodebris, defined as “measurable particles,” occurred in 12/18 patients (66.7%) treated with laser atherectomy; of these, 4 EPDs (22.2%) captured clinically significant emboli, defined as >2 mm. Meanwhile, macrodebris occurred in 7/20 patients (35%) after receiving adjunctive intervention; of these, 4 patients (20%) had clinically significant emboli. One DE (5%) occurred after EPD retrieval prior to completing definitive treatment. The DEEP EMBOLI registry demonstrated that although DE with laser atherectomy is higher than standard treatment with PTA, the clinically significant DE rates were similar. EPD effectively capture macrodebris and is associated with successful immediate angiographic results.4
The PROTECT (Preventing Lower Extremity Distal Embolization Using Embolic Filter Protection) registry is a single-center, prospective, open-label registry that evaluated the safety and effectiveness of filter EPDs (SpiderFX or EmboShield) to reduce DE in PPI. Forty patients with 56 lower-extremity lesions were treated with angioplasty/stenting vs SilverHawk atherectomy (Medtronic) with EPD. Patients were then angiographically evaluated for signs of DE including presence of slow flow or loss of distal vessel run-off, and the filters were inspected after removal for presence of visible embolic material. Debris burden was classified into clinically significant debris (longest diameter >2 mm), macrodebris (visible, larger than dust-like size), and microdebris (small, dust-like size).5 The threshold of 2 mm is based on the theory that debris >2 mm could compromise a distal tibial artery, which averages 2.0-2.5 mm in diameter.4 All SilverHawk cases (n=11) demonstrated macroembolism captured by the EPD, of which 90.9% were clinically significant. Meanwhile, 37.9% of angioplasty/stenting cases (n=11) had macroembolism. All filters were deployed and retrieved successfully and 97.5% of patients met the primary angiographic endpoint of not having visible DE, slow flow, or loss of run-off. One case had no flow distally due to an overfilled filter, which was retrieved; the procedure was continued without EPD replacement and resulted in tibial embolization. Another case had a sidebranch embolization proximal to the EPD. Overall, the PROTECT registry demonstrated that filter EPDs are effective at catching macrodebris and are associated with successful immediate angiographic results; however, the clinical significance was undetermined.5
The DEFINITIVE Ca++ trial is a multicenter, prospective, single-arm study evaluating the safety and effectiveness of using directional atherectomy (SilverHawk, TurboHawk) and EPD (SpiderFX) to treat moderate to severely calcified infrainguinal lesions. The study comprised 168 moderately to severely calcified lesions in 133 patients with Rutherford class 2-4 disease who were treated with atherectomy. Adjunctive therapy, predominantly angioplasty, was performed in 91 lesions (53.8%) in 74 patients. Plaque debris was found in 129/133 atherectomy device nose cones (97.0%) and in 122/138 EPDs (88.4%). Of the EPDs with debris, 119/122 (97.5%) were successful at preventing DE. The 3 cases with DE were treated with catheter aspiration and had no clinical sequelae. Meanwhile, preservation of run-off was confirmed by core laboratory angiographic review in 98.3% of patients. Two patients (1.5%) had enough debris to require a second filter. The DEFINITIVE Ca++ trial determined that directional atherectomy with EPD is considered a safe and effective intervention for complex lesions in the superficial femoral and/or popliteal arteries with moderate to severe calcification.6
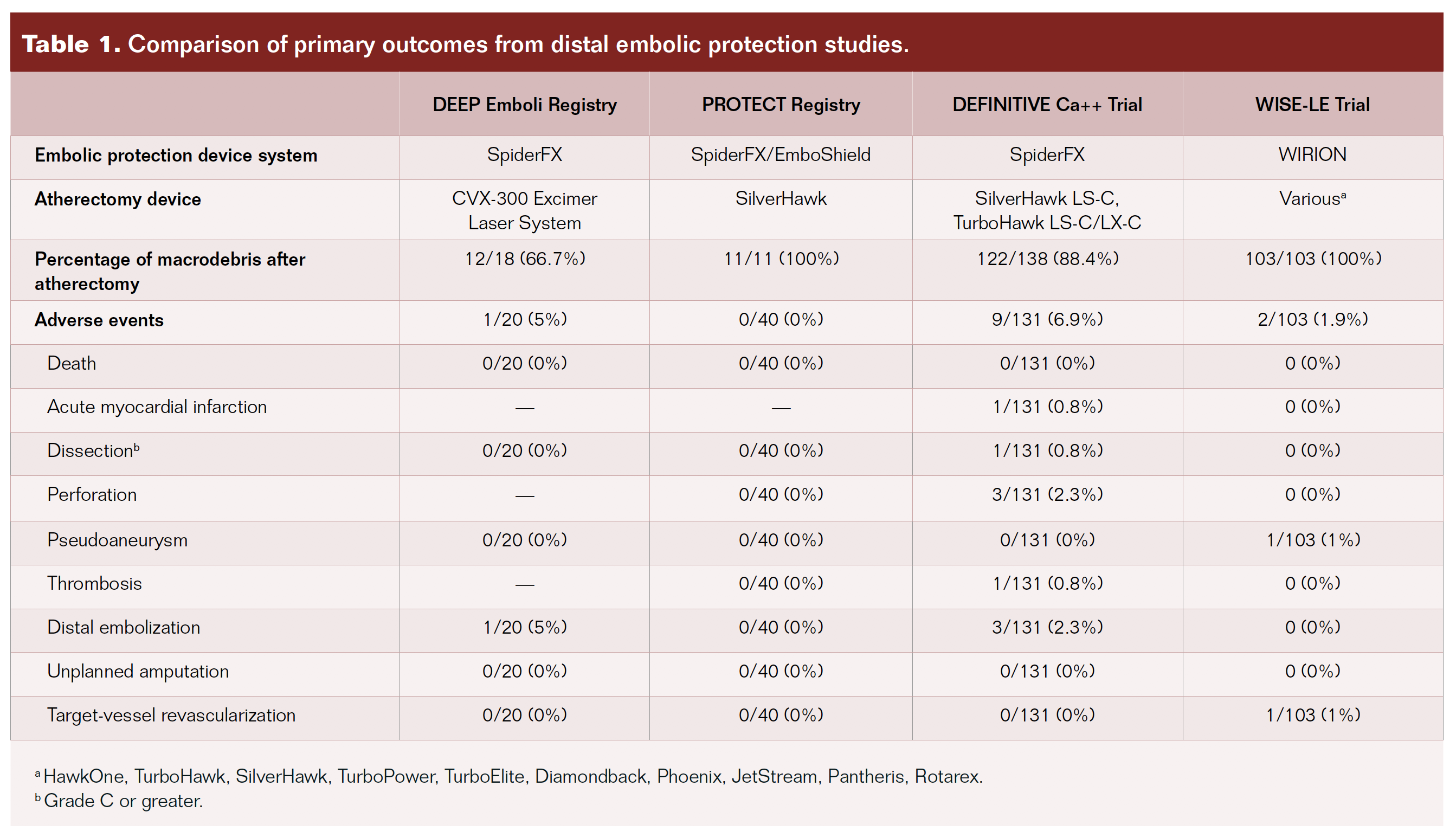
The more recent WISE-LE (Evaluation of Wirion EPS in Lower Extremities Arteries) study, a prospective, multicenter, non-randomized, single-arm investigation, evaluated the safety of the FDA-approved Wirion EPS filter. The study included 103 patients and 79.6% of lesions were in the superficial femoral artery. Lesions were longer, with similar degree of calcification when compared with the DEFINITIVE Ca++ and DEFINITIVE LE studies. Ten different atherectomy devices in conjunction with Wirion EPS and adjunctive therapy were used at the operator’s discretion. WISE-LE found that 100% of cases had embolization, irrespective of atherectomy device type, and that Wirion EPS was successful in capturing both micro- and macrodebris with very low adverse event rates. Debris analysis demonstrated debris of <1 mm, 1-2 mm, and >2 mm were captured in 98%, 22%, and 9% of filters, respectively. Two major adverse events (1.9%) occurred (1 occlusion requiring target-vessel revascularization and 1 pseudoaneurysm); both were deemed unrelated to the device or procedure. Demonstrating high success and device safety, the WISE-LE study suggests the benefit of using the WIRION EPS filter during lower-extremity atherectomy procedures.7
Lesion Selection
To evaluate the efficacy of embolic reduction strategies, Makam8 performed a single-center, retrospective, single-arm study evaluating EPD during infrainguinal atherectomy. Twenty-eight patients with 55 lesions were treated with angioplasty with Proteus (Angioslide), directional atherectomy with SilverHawk/TurboHawk, laser atherectomy, and orbital atherectomy. EPDs used were SpiderFX and Proteus, which has a unique design that allows simultaneous angioplasty and embolic debris removal. Embolic load retrieved from Proteus and SpiderFX was analyzed with the Proteus Particle Visualization Kit (Angioslide) to stain, visualize, and quantify debris. All EPDs were deployed and retrieved without complications. Procedural success with <30% residual stenosis was reached in 54/55 cases (98.2%). Three cases (5.45%) had reintervention at 4-9 months. Atherectomy performed on restenotic and reoccluded lesions resulted in twice the burden of debris in comparison with de novo lesions (42.53 ± 21.42 mm2 vs 21.42 ± 15.09 mm2; P<.01). Thrombolysis in conjunction with laser atherectomy had the greatest embolic load (59.84 ± 36.88 mm2), followed by laser atherectomy alone (36.99 ± 31.36 mm2), directional atherectomy (27.33 ± 17.20 mm2), and orbital atherectomy (17.04 ± 11.14 mm2; P<.05). Makam demonstrated that EPD use should be considered when treating lesions expected to result in greater embolic debris (ie, TASC II D classification, restenosis, reocclusion, or thrombolysis with laser atherectomy).
Mendes et al2 retrospectively evaluated 566 patients with 836 femoropopliteal PPIs to determine rates of DE and its clinical significance in patients with femoropopliteal PPI with or without EPD (SpiderFX). Primary endpoint was defined as angiographic detection of DE, with occlusion or filling defect in a previously patent artery, distal to the treated lesion. Other parameters include macroscopic debris load in filter EPD, major adverse events (mortality, morbidity, reintervention rates, or amputation), and vessel patency. All atherectomy cases had macroscopic debris. Of the cases with filter EPD, 59/87 (68%) had macroscopic debris, and out of these, 39/59 (66%) had moderate to severe burden of debris. In comparison with non-EPD cases, EPD cases had statistically significantly longer lesions (109 ± 94 mm vs 85 ± 76 mm), greater prevalence of occlusions (64% vs 30%) and greater proportion of TASC II C and D lesions (56% vs 30%). Outcomes for EPD vs non-EPD cases were evaluated, revealing no difference in primary patency and reintervention rates at 14 months between the groups. DE occurred in 35 cases (4%) of the 836 total interventions. Of the EPD cases, 2/87 (2%) had DE but neither had clinical consequences requiring reintervention. Meanwhile, DE occurred in 33/749 non-EPD cases (4.4%), and 21% of these cases required reintervention (1 case needed amputation; 1 case resulted in death). Of the cases with DE, 9% occurred with atherectomy. Overall, Mendes et al concluded that clinically significant DE during femoropopliteal PPI does not occur frequently enough to support the routine use of EPD in most PPI. However, considering embolic events were associated with recanalization of chronic total occlusions, EPD use should be considered in cases of chronic total occlusion treated with atherectomy.
To identify an algorithm for EPD use based on lesion morphology and vascular anatomy, Krishnan et al9 prospectively evaluated 508 claudicants at a single center. All cases were analyzed by angiography and histopathology, evaluating for angiographic calcium, DE, in-stent restenosis, chronic total occlusion, filter overflow, and plaque histopathology. Associations between lesion characteristics, patient demographics, and clinical presentation were evaluated with logistic regression. Krishnan et al found that there were no significant differences in DE based on type of atherectomy device. After simple logistic regression analysis, macroemboli were found to be strongly associated with lesion length >140 mm, calcification >40 mm, chronic total occlusions, single-vessel run-off, and in-stent restenosis.
Conclusion
During endovascular atherectomy of the lower extremities, distal embolization is a known phenomenon that may result in the occlusion of downstream vessels. EPD use has been demonstrated to be effective in capturing embolic debris during lower-extremity PPI with atherectomy, with a high safety profile and improved clinical outcomes.2,4-8 However, rates of clinically significant DE in patients undergoing PPI with atherectomy remain low, with limited cost-benefit analysis to guide decision making. Despite benefit in the appropriate clinical setting, supportive evidence justifying the routine use of EPD in all cases is lacking. Consideration of EPD use is recommended when using atherectomy for lesions >140 mm in length, calcification >40 mm, in-stent restenosis, chronic total occlusion, and in cases with limited run-off vessels.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript accepted May 25, 2021.
Address for correspondence: Millie Liao, DO, MS, Interventional and Diagnostic Radiology Resident Physician, Department of Vascular & Interventional Radiology, Loma Linda University, 11234 Anderson St, Loma Linda, CA 92354. Email: millieliao.ir@gmail.com
REFERENCES
1. Bangalore S, Bhatt D. Embolic protection devices. Circulation. 2014;129:e470-e476.
2. Mendes B, Oderich G, Fleming M, et al. Clinical significance of embolic events in patients undergoing endovascular femoropopliteal interventions with or without embolic protection devices. J Vasc Surg. 2014;59:359-367.
3. McKinsey J, Zeller T, Rocha-Singh K, et al. Lower extremity revascularization using directional atherectomy: 12-month prospective results of the DEFINITIVE LE study. JACC Cardiovasc Interv. 2014;7:923-933.
4. Shammas N, Coiner D, Shammas G, et al. Distal embolic event protection using excimer laser ablation in peripheral vascular interventions: results of the DEEP EMBOLI registry. J Endovasc Ther. 2009;16:197-202.
5. Shammas N, Dippel E, Coiner D, et al. Preventing lower extremity distal embolization using embolic filter protection: results of the PROTECT registry. J Endovasc Ther. 2008;15:270-276.
6. Roberts D, Niazi K, Miller W, et al. Effective endovascular treatment of calcified femoropopliteal disease with directional atherectomy and distal embolic protection: final results of the DEFINITIVE Ca++ trial. Catheter Cardiovasc Interv. 2014;84:236-244.
7. Shammas NW, Pucillo A, Jenkins JS, et al. WIRION embolic protection system in lower extremity arterial interventions: results of the pivotal WISE LE trial. JACC Cardiovasc Interv. 2018;11:1995-2003.
8. Makam P. Evaluating embolic reduction techniques concurrent to infrainguinal interventions: a single-center experience. J Invasive Cardiol. 2014;26:277-282.
9. Krishnan P, Tarricone A, Purushothaman R, et al. An algorithm for the use of embolic protection during atherectomy for femoral popliteal lesions. JACC Cardiovasc Interv. 2017;10:403-410.
