


Role of Endovascular Interventions in the Management of COVID-19 Patients Presenting With Massive Hemorrhage: A Single-Center Experience
Abstract
The COVID-19 pandemic has affected millions of people and led to significant mortality and morbidity. Patients with severe COVID-19 infection may have endothelial inflammation, leading to pseudoaneurysm formation with a risk of massive bleeding. We discuss the role of interventional radiology in its management. Methods. This retrospective study was conducted between May 2021 and November 2021. The inclusion criteria were all COVID-19-positive patients who presented with massive hemorrhage and were referred to interventional radiology. Demographics, clinical manifestations, imaging findings, endovascular management, and outcomes were analyzed for all included patients. Results. All 8 patients underwent endovascular embolization of pseudoaneurysms that were detected after contrast-enhanced computed tomography study of the chest, head, and neck. Successful embolization was achieved in all 8 patients. Two patients underwent lobectomy following embolization. No major complications were noted. There were no further episodes of bleeding. Conclusions. COVID-19 patients can present with acute massive hemorrhage 2 to 6 months after documentation of the initial infection. Secondary fungal infection following COVID-19 is a known complication. These patients require multimodality treatment. Endovascular management is safe and effective in most patients. Surgical backup is required for patients who do not respond to endovascular management.
VASCULAR DISEASE MANAGEMENT 2022;19(8):E122-E128
Key words: COVID-19, endovascular embolization, hemorrhage, internal carotid artery pseudoaneurysm, internal maxillary artery pseudoaneurysm, mucormycosis, pulmonary artery pseudoaneurysm
Introduction
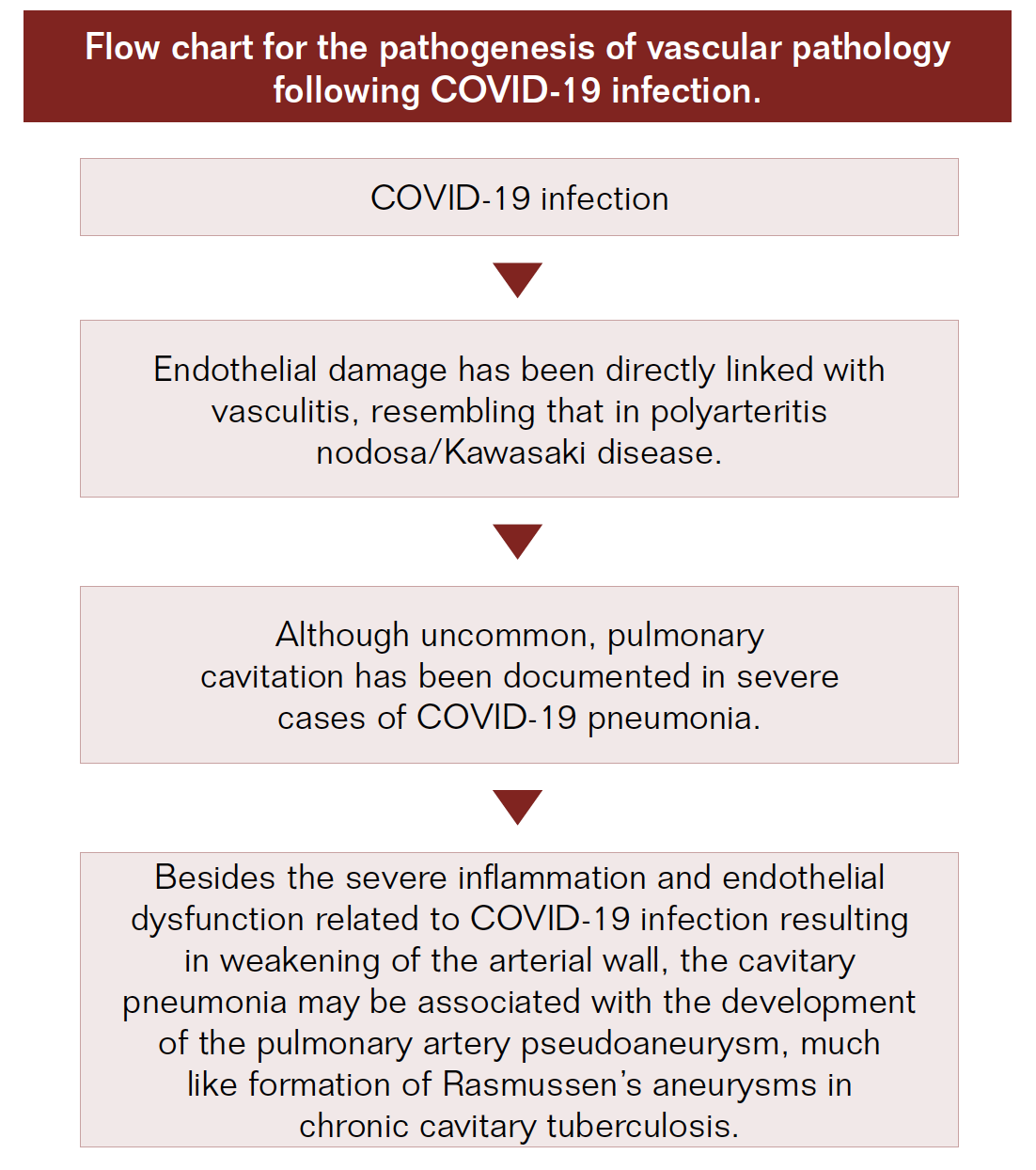
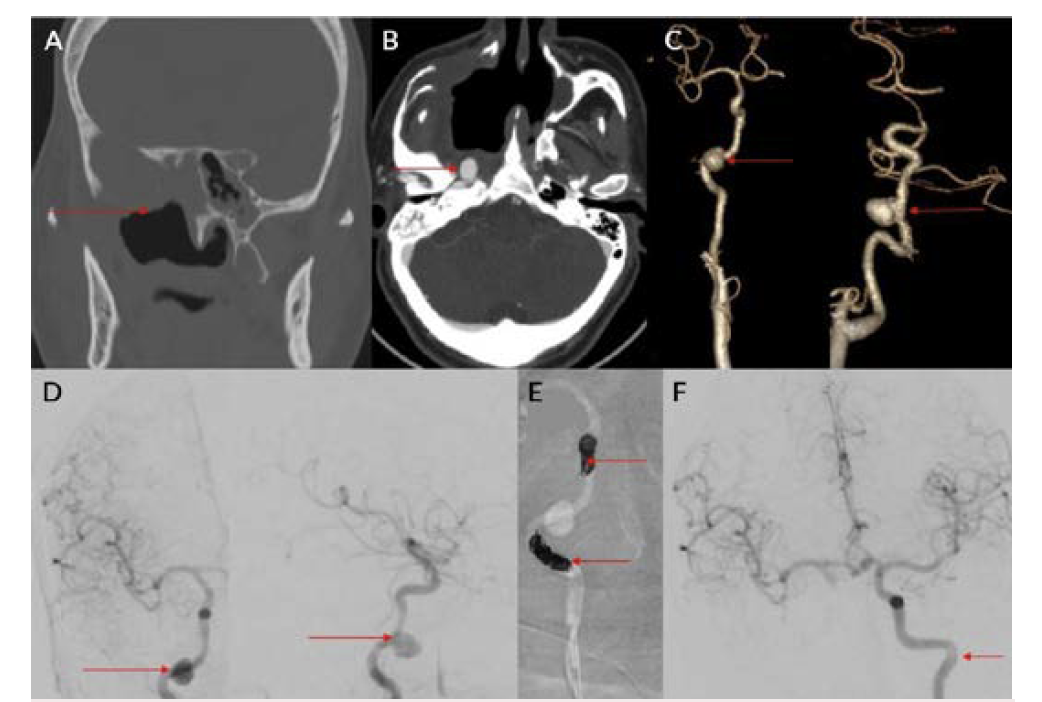
Pseudoaneurysms of major vessels are rare yet important entities because of their risk of rupture and unpredictable life-threatening bleeding. The COVID-19 pandemic commenced in January 2020 has affected millions of people all over the world with significant multiorgan involvement, causing high rates of morbidity and mortality. Patients with severe COVID-19 infection may have endothelial inflammation leading to pseudoaneurysm formation with a risk of increased bleeding (Figure 1). This retrospective study followed 8 patients with COVID-19 infection with associated vascular involvement leading to pseudoaneurysm formation and bleeding that was managed with endovascular intervention, highlighting the role of interventional radiology in the management of these patients.
Results
This retrospective study, conducted between May 2021 and November 2021 with prior approval by the institutional review board, included COVID-19-positive patients proven by real-time reverse transcription–polymerase chain reaction (RTPCR) test who presented with massive hemorrhage and were referred to interventional radiology. Patient demographics, clinical manifestations, imaging findings, endovascular management, and outcomes were analyzed.
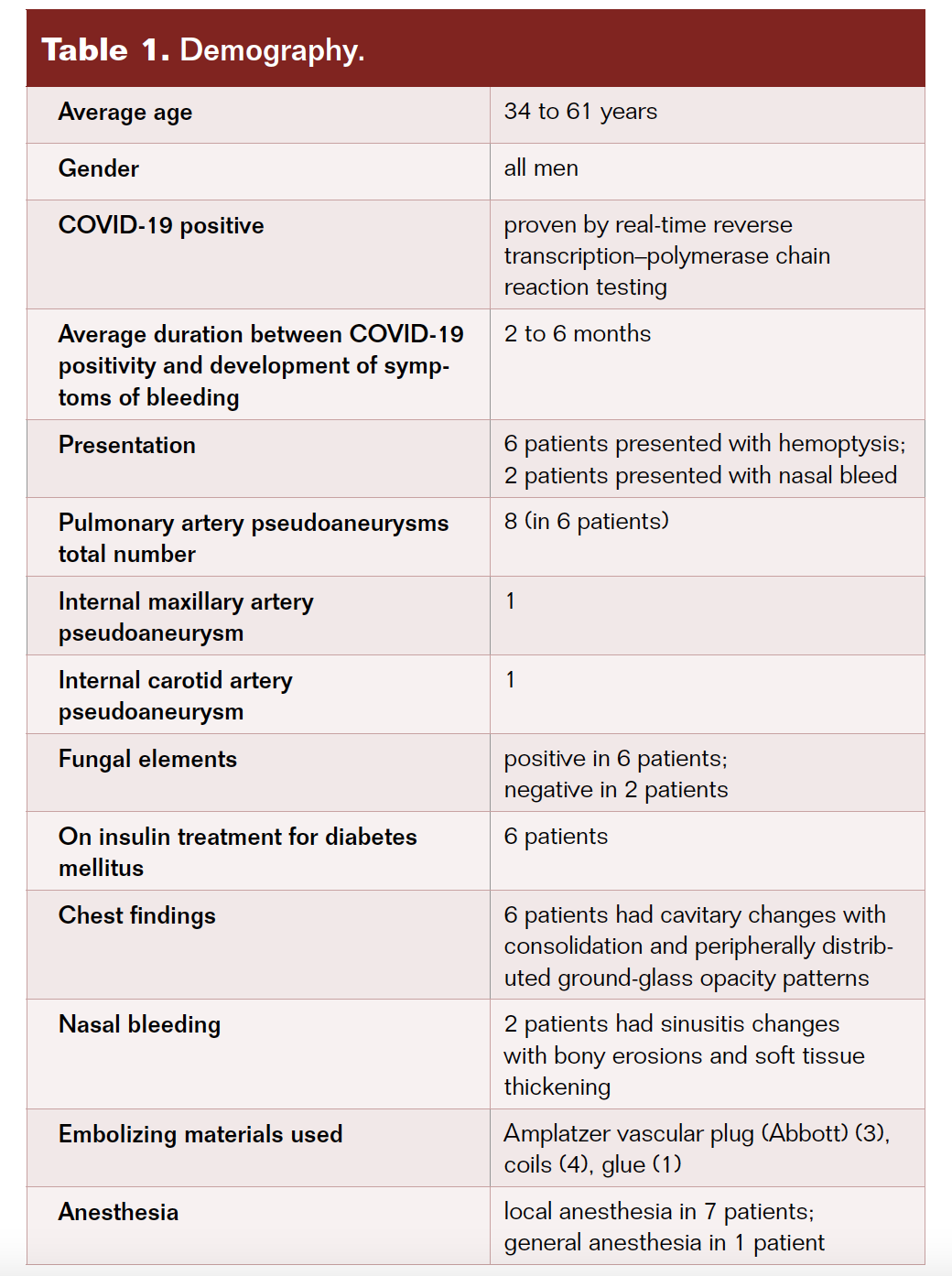
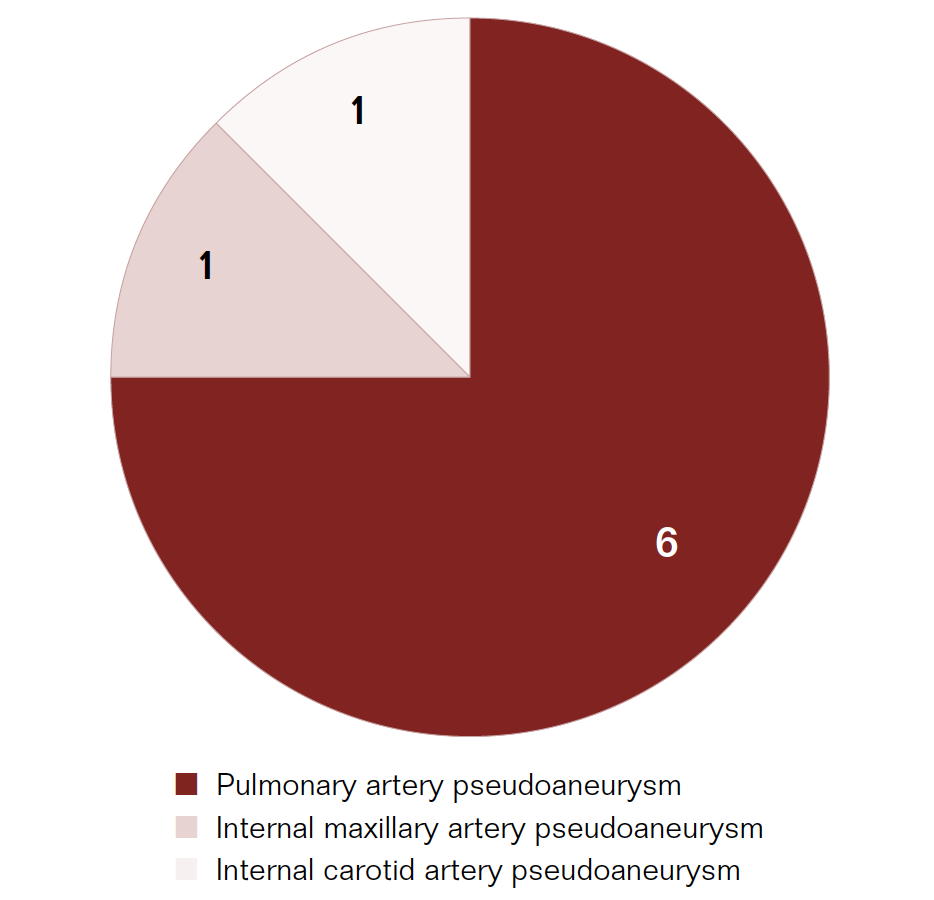
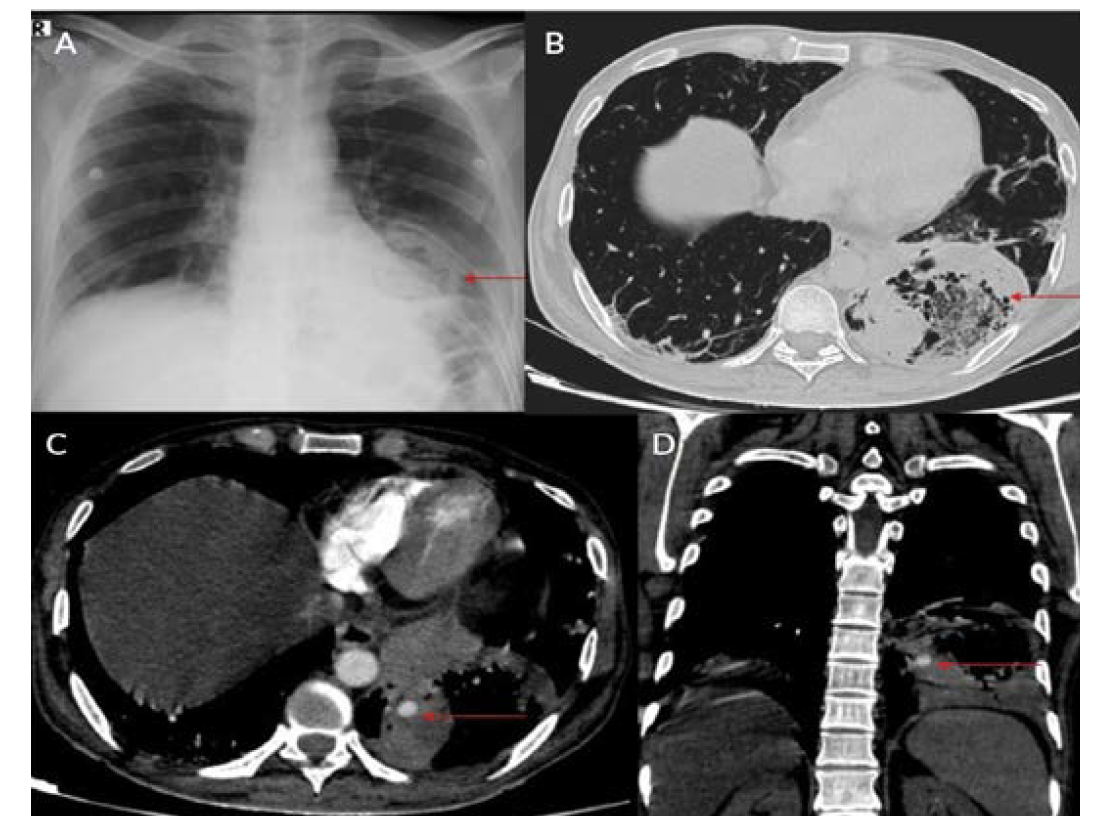
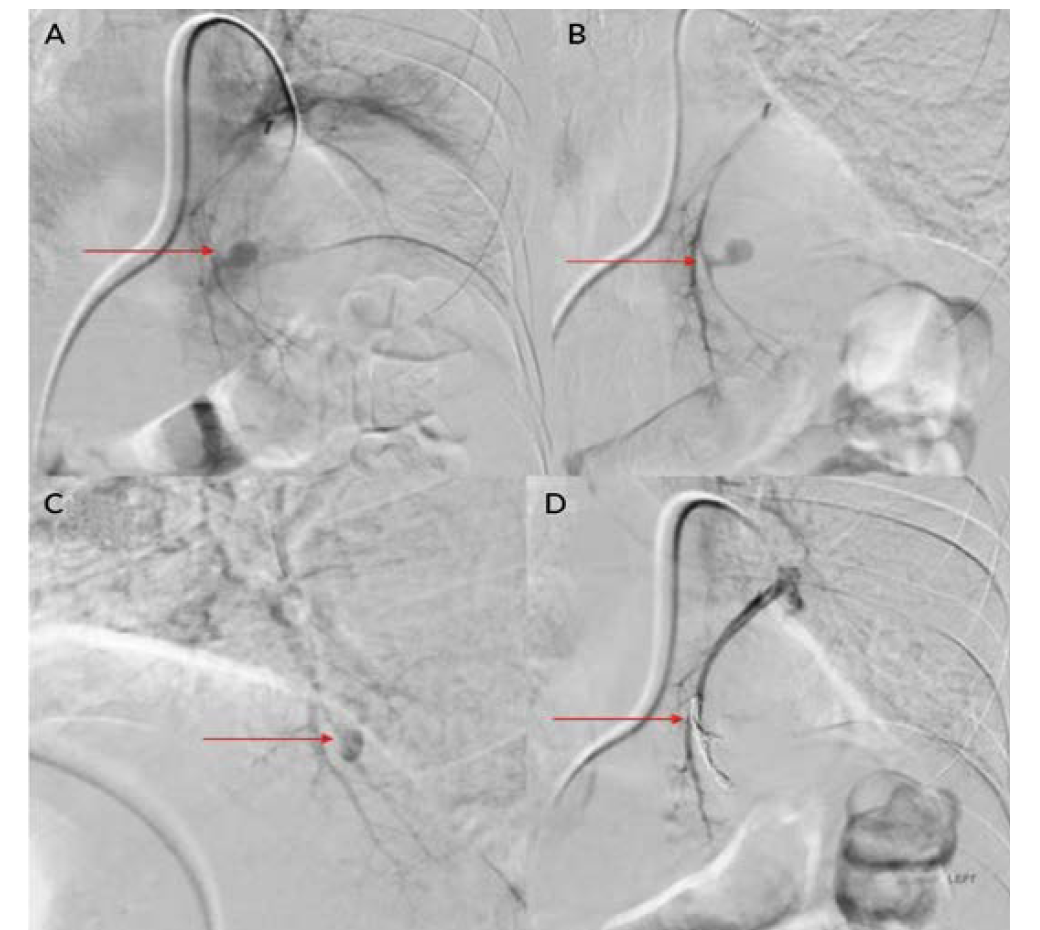
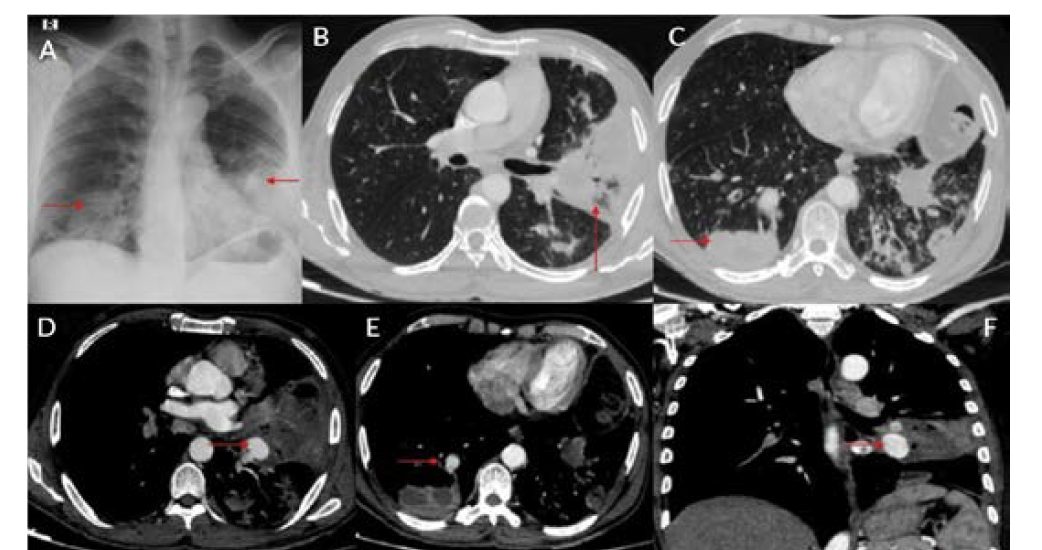
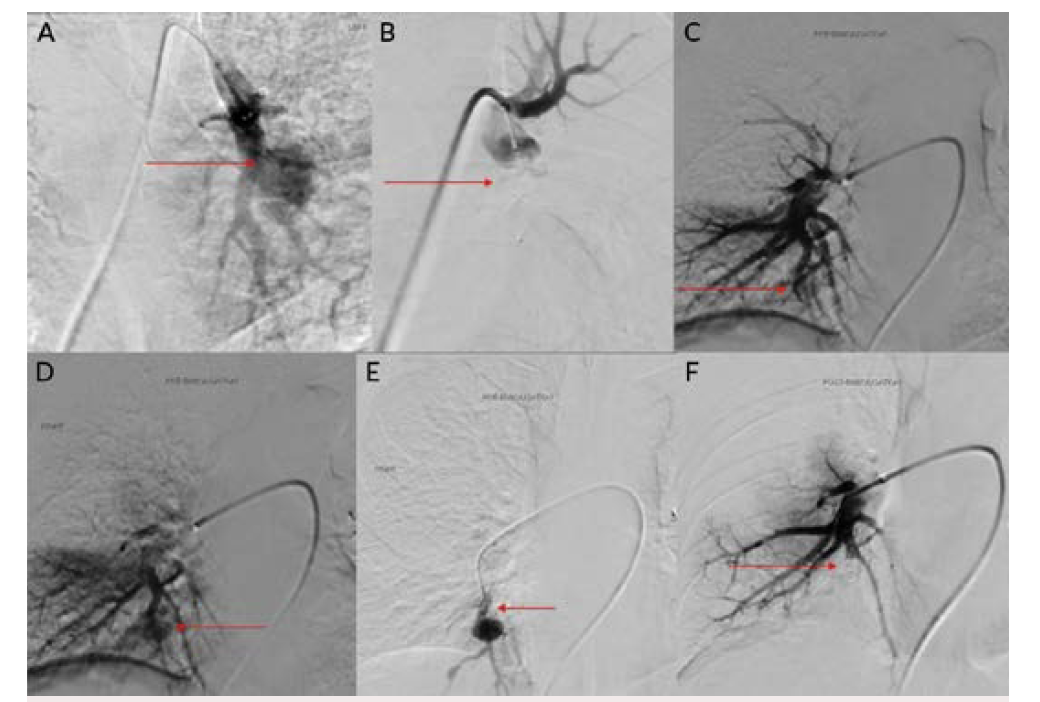
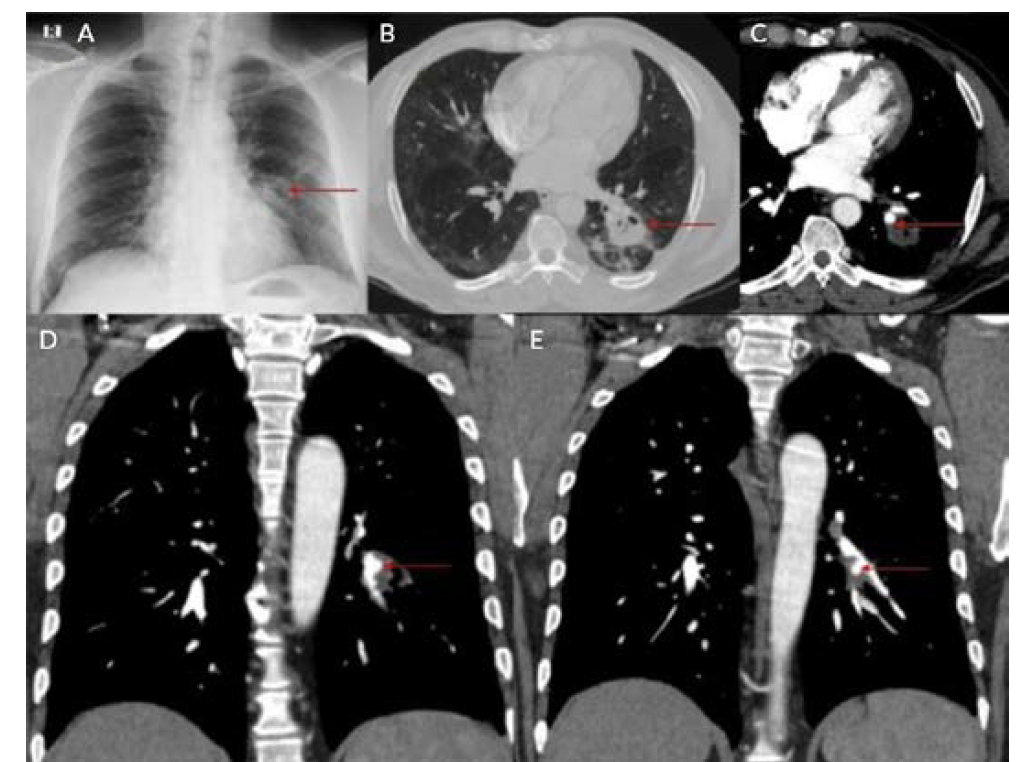
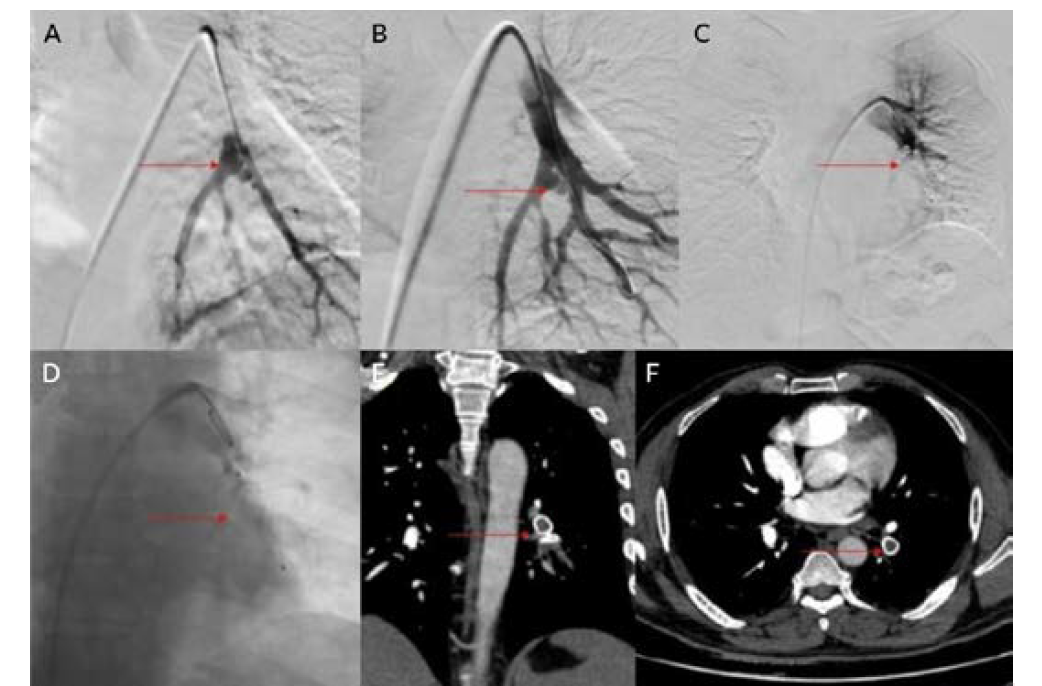
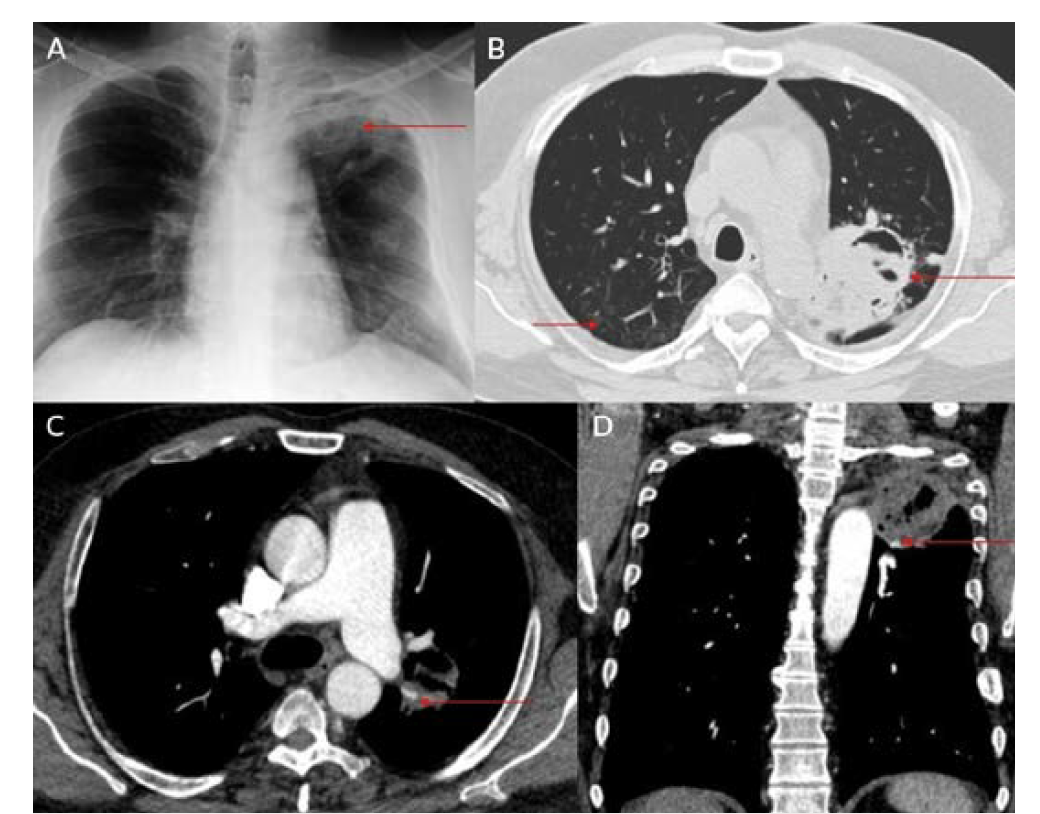
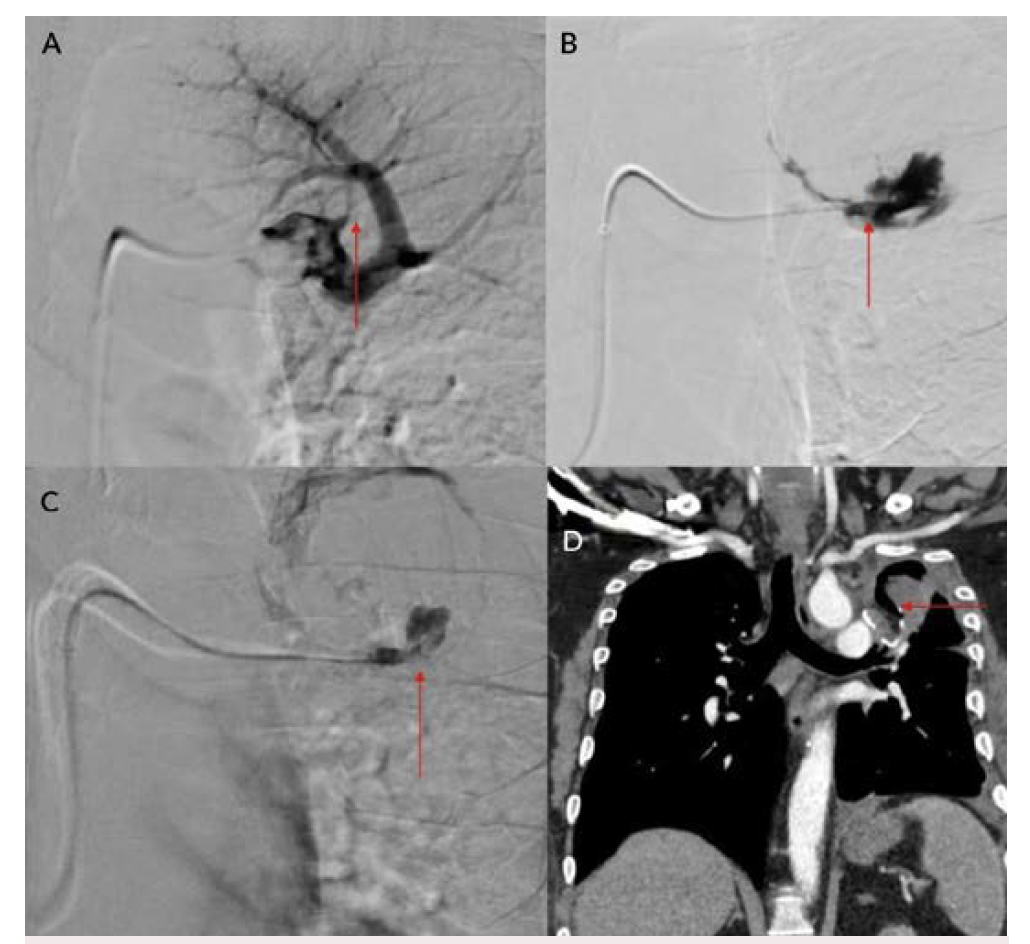
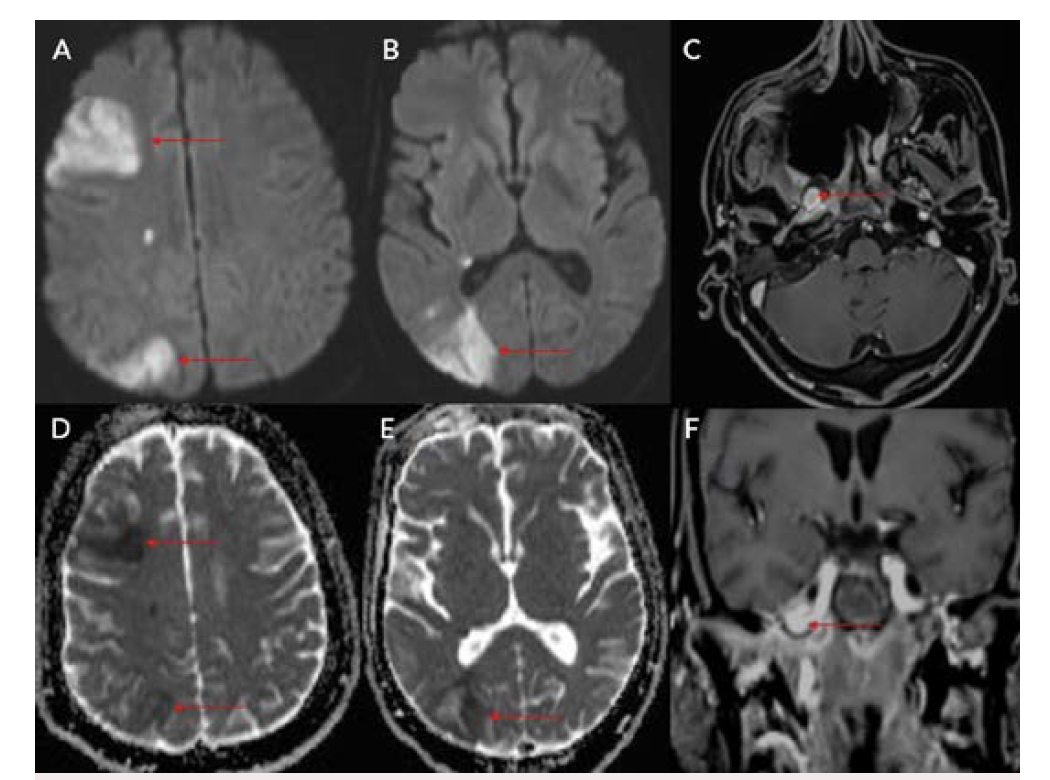
Eight patients were included during this study period; all were men between ages 34 and 61 (Table 1). Positivity to COVID-19 RTPCR test was detected over a period of 2 to 6 months prior to the acute hemorrhage. Six patients presented with massive hemoptysis; 2 presented with severe epistaxis. A contrast-enhanced computed tomography angiography was done in all patients. All 6 patients who presented with massive hemoptysis were detected to have pulmonary arterial pseudoaneurysms with associated cavitary lesions in the lungs (Figure 2). Among the 2 patients who presented with nasal bleed, 1 had a biopsy and culture-proven invasive fungal sinusitis with an internal maxillary artery pseudoaneurysm, probably of mycotic etiology. The second patient also diagnosed with invasive fungal sinusitis had multiple sinonasal debridements outside before presenting with massive epistaxis wherein a diagnosis of internal carotid artery pseudoaneurysm was made, probably secondary to iatrogenic or mycotic etiology. The presence of concomitant COVID-19 infection in these patients predisposed them to impairment of cell-mediated immunity, immune dysregulation, and a decrease in CD4 and CD8 counts, increasing their vulnerability to fungal infections. In 6 patients it was possible to obtain samples for fungal elements through biopsy. Endovascular embolization was performed under local anesthesia in 7 patients, and under general anesthesia in 1 patient. Different embolic agents were used: coils (Figures 3A and 3B), Amplatzer vascular plug (Abbott) (Figures 4A and 4B, Figures 5A and 5B), and glue (Figures 6A and 6B). However, 2 patients underwent lobectomy for extensive parenchymal disease apart from pseudoaneurysm. One patient with pulmonary artery pseudoaneurysm had contrast extravasation into the cavity during the procedure. All patients had cessation of hemorrhage. However, 2 patients required pulmonary lobectomy because of extensive parenchymal disease after embolization for the pseudoaneurysm.
Discussion
COVID-19 infection has affected people worldwide since 2020 after its initial outbreak in Wuhan, China. It has caused significant mortality and morbidity, causing millions of deaths to date. COVID-19 infection is known to affect multiple organs such as the lungs, heart, brain, and skin, with the lung being most common.1 Patients with COVID-19 usually present with complaints of fever, cough, malaise, and difficulty breathing.1 Diabetes mellitus is an independent risk factor for COVID-19 infection.1 Fungal infection was a known complication following COVID-19 infection, especially in those with poorly controlled blood sugar and who have been treated with immunosuppressive agents such as steroids.2,3 Pulmonary complications following COVID-19 infection were mainly related to fibro-cavitary changes.3-5 Hemorrhage following fungal infection was mainly due to vascular involvement and formation of pseudoaneurysm.6 Patients with severe COVID-19 infection may have endothelial inflammation and secondary fungal infection, leading to pseudoaneurysm formation with a risk of increased bleeding.5,6 Fungal sinusitis following COVID-19 infection is a well-known entity that can cause bleeding due to the involvement of the internal and external carotid vessels.2,3,5 Extracranial carotid artery aneurysms are found most frequently in the common carotid artery at or near the bifurcation, less frequently in the internal carotid artery (Figures 7A and 7B), and least often in the external carotid artery.7,8 Ongoing studies of the precise molecular underpinnings of mycotic pseudoaneurysms suggest that arterial wall breakdown is likely caused by matrix-degrading enzymes produced by either seeded bacteria or inflammatory cells of the host response.6 Diabetes and fungal infections are more frequently documented, which could result in mycotic aneurysm, spontaneous rupture, and massive hemorrhage.2,3,5
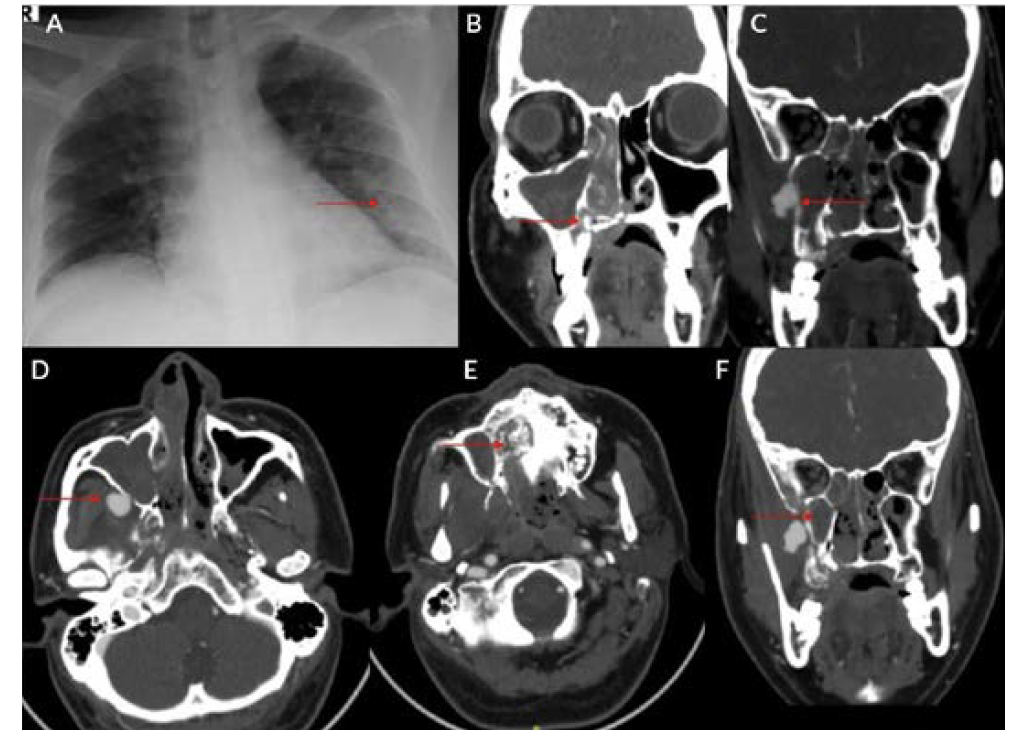
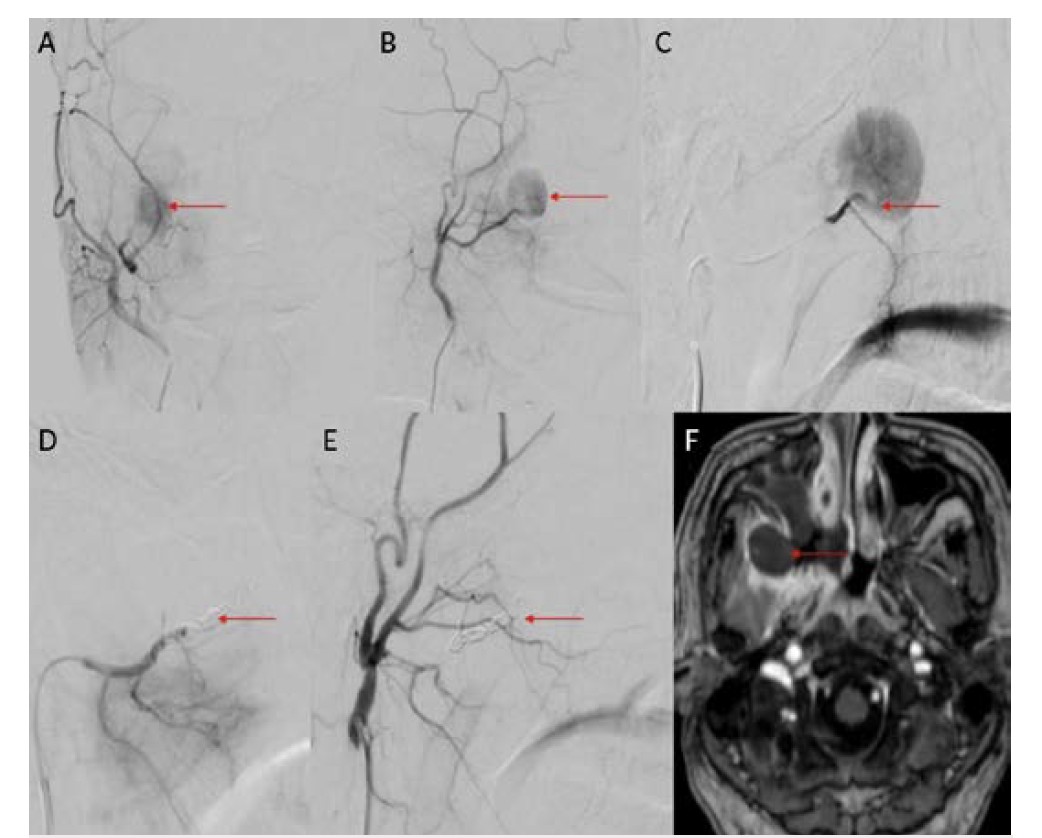
Pulmonary artery pseudoaneurysm is a rare but important entity because of its high risk of life-threatening hemorrhage.2,5,9,10 Peripheral branches of the lower lobe pulmonary artery are most commonly affected.2,5,10 A pseudoaneurysm is different from a true aneurysm because there is no wall except for the hematoma that is surrounding and containing it.6,9,11,12 The etiology of a pulmonary artery pseudoaneurysm is inflammatory erosion secondary to tuberculosis (Rasmussen aneurysm), necrotizing pneumonia, bacterial endocarditis, mucormycosis, or vasculitides (Marfan syndrome, Behçet’s disease, etc.). Other causes include necrotic cavitary lung carcinoma, congenital heart disease, and traumatic injury. Iatrogenic pseudoaneurysm secondary to pulmonary artery catheter placement has also been reported.4-6,9-11 Internal maxillary artery pseudoaneurysm is rare and is more commonly encountered following trauma and iatrogenic injury (Figures 8A and 8B).7,8,13 These patients present with massive or moderate bleeds, which can lead to death in about 50% of cases if left untreated.2,4 The most common artery leading to hemoptysis is the bronchial artery, which constitutes around 80% to 90%.4,5,13 Hemoptysis related to the pulmonary artery constitutes around 10%.10,14 Multidetector computed tomography (MDCT) pulmonary angiography is the modality of choice to diagnose pulmonary artery aneurysms.2,9,10,12 It provides detailed information about the presence, number, size, shape, and origin of pulmonary artery aneurysms.2,9,10 MDCT also allows detailed assessment of the orientation and size of the aneurysmal sac and size of the neck on multiplanar reconstruction.2,10 It also gives an overall idea about the pathology, and the involved lung segment eventually helps in planning the treatment accordingly.4,10,12,14 Digital subtraction angiography has the advantage of allowing endovascular intervention at the time of diagnosis.4,12,14 Ultrasound and magnetic resonance imaging are also used in cases of aneurysms involving neck vasculature.2,14,12
Management of these pseudoaneurysms usually involves a multidisciplinary approach. Multiple treatment approaches are available: conservative, surgical, and endovascular.4-6,11,14 The conservative approach mainly consists of medical management by treating the underlying disease with antifungal drugs, such as tranexamic acid. Surgical management usually consists of either ligation of the involved artery, bypass graft after ligation, and resection of the involved lung segment and vasculature.2,6,11,15 Medical and surgical management of massive hemoptysis is associated with a mortality rate ranging from 35% to 100%.3,5,9
Endovascular intervention is a minimally invasive technique that is used to treat these types of pseudoaneurysms.4-6,11 Pulmonary artery pseudoaneurysms can be treated with multiple techniques, such as coil embolization of the involved artery, plug placement within the involved artery, glue embolization of the aneurysm, and placement of a stent graft across the aneurysm.4,10,11 If the aneurysm is peripherally placed and is not accessible via a transarterial approach, ultrasound-guided injections such as thrombin or glue can be tried.14 The endovascular approach is minimally invasive compared with surgery.9,10 Mortality, morbidity, and complication rates following endovascular intervention are lower compared with surgery.5,11 Hospital stays following endovascular intervention are usually lower.9,10 Endovascular embolization has an initial success rate of 95%, and surgery is reserved for those patients where multiple sittings of embolization have failed.4,5,10
Conclusion
COVID-19 patients can present with acute massive hemorrhage 2 to 6 months after documentation of the initial infection. Secondary fungal infection with or without diabetes mellitus following COVID-19 is a known complication. A high index of suspicion is required to evaluate for pseudoaneurysm when patients present with massive bleeding from the upper respiratory tract. These patients require a multidisciplinary approach; endovascular management is safe and effective, and surgical backup is required for patients who do not respond to endovascular management.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript accepted August 11, 2022.
Address for correspondence: Shyamkumar N. Keshava, MBBS, DMRD, DNB, Department of Interventional Radiology, Christian Medical College, W4GP+7CW, Vellore, Tamil Nadu 632004, India. Email: shyamkumar.n.keshava@gmail.com
Related Articles
Catheterization, Myocardial Infarction, and the COVID-19 Pandemic: The Devil Is in the Details
COVID-19 and Aortic Thrombus: An Unusual and Dangerous Combination
High Risk of Deep Vein Thrombosis and Pulmonary Embolism in Patients With COVID-19
REFERENCES
1. Salman R, Masand P, Huisman TAGM, et al. A novel large-vessel arteritis in SARS-CoV-2-related multisystem inflammatory syndrome in children (MIS-C). Radiol Cardiothorac Imaging. 2021;3(1):e200535. doi:10.1148/ryct.2020200535
2. Chen Y, Gilman MD, Humphrey KL, et al. Pulmonary artery pseudoaneurysms: clinical features and CT findings. AJR Am J Roentgenol. 2017;208(1):84-91. doi:10.2214/AJR.16.16312
3. Swain S, Ray A, Sarda R, et al. COVID-19-associated subacute invasive pulmonary aspergillosis. Mycoses. 2022;65(1):57-64. doi:10.1111/myc.13369
4. Jajodia S, Goenka U, Jash D, Tiwary I, Goenka MK. Endovascular management of massive hemoptysis due to covid-19 related pulmonary artery pseudoaneurysm: a rare entity. Radiol Case Rep. 2021;16(11):3597-3601. doi:10.1016/j.radcr.2021.08.048
5. Pruthi H, Muthu V, Bhujade H, et al. Pulmonary artery pseudoaneurysm in COVID-19-associated pulmonary mucormycosis: case series and systematic review of the literature. Mycopathologia. 2022;187(1):31-37. doi: 10.1007/s11046-021-00610-9
6. Zhang N, Lechien JR, Martinez V, Carlier R-Y, El Hajjam M. Contribution of interventional radiologist in the management of pseudoaneurysm and neck hemorrhages in COVID-19 patients. Ear Nose Throat J. 2021;100(2_suppl):148S-151S. doi:10.1177/0145561320987030
7. Dunn GP, Uppaluri R, Hessler JL, Layland MK, Derdeyn CP, Sunwoo JB. Mycotic pseudoaneurysm of the internal maxillary artery: case report and review of the literature. Arch Otolaryngol Head Neck Surg. 2007;133(4):402-406. doi:10.1001/archotol.133.4.402
8. Bozkurt M, Kapi E, Karakol P, Yorgancilar E. Sudden rupture of the internal maxillary artery causing pseudoaneurysm (mandibular part) secondary to subcondylar mandible fracture. J Craniofac Surg. 2009;20(5):1430-1432. doi:10.1097/SCS.0b013e3181aee442
9. Khurram R, Karia P, Naidu V, Quddus A, Woo WL, Davies N. Pulmonary artery pseudoaneurysm secondary to COVID-19 treated with endovascular embolisation. Eur J Radiol Open. 2021;8:100346. doi:10.1016/j.ejro.2021.100346
10. Singh V, Garg P, Nath A, Phadke RV. Utility of endovascular embolisation in management of peripheral pulmonary artery aneurysms. Egypt J Radiol Nuclear Med. 2016;47(4):1415-1421.
11. Park A, Cwikiel W. Endovascular treatment of a pulmonary artery pseudoaneurysm with a stent graft: report of two cases. Acta Radiol. 2007;48(1):45-47. doi:10.1080/02841850601045104
12. Zugazaga A, Stachno MA, García A, et al. Pulmonary artery pseudoaneurysms: endovascular management after adequate imaging diagnosis. Eur Radiol. 2021;31(9):6480-6488. doi:10.1007/s00330-021-07819-8
13. Barbalho JCM, Santos ES, Menezes JMS Jr, Gonçalves FR, Chagas OL Jr. Treatment of pseudoaneurysm of internal maxillary artery: a case report. Craniomaxillofac Trauma Reconstr. 2010;3(2):87-89. doi:10.1055/s-0030-1254378
14. Shin S, Shin T-B, Choi H, et al. Peripheral pulmonary arterial pseudoaneurysms: therapeutic implications of endovascular treatment and angiographic classifications. Radiology. 2010;256(2):656-664. doi:10.1148/radiol.10091416
15. Peluso A, Venetucci P, Catelli A, Bracale UM. Management of deep femoral artery pseudoaneurysm in a COVID-19 patient. Ann Vasc Surg. 2021;73:141-142. doi:10.1016/j.avsg.2021.01.066

