Medical Device–related Pressure Injury Due to Urinary Catheterization: A Case Report
Abstract
BACKGROUND: Urethral erosion secondary to a medical device–related pressure injury (MDRPI) is preventable, understudied, not well understood, and often overlooked. PURPOSE: This case report describes a patient who sustained an MDRPI secondary to indwelling urinary catheter placement for urinary retention. CASE STUDY: A 93-year-old man with prostate cancer and pneumonia received an indwelling urinary catheter for retention during a 2-week hospitalization. Upon his transfer to a rehabilitation facility, the patient’s daughter informed staff that she had observed a 1-cm urethral erosion on the urinary meatus. Within a week, the penile erosion worsened to encircle the urinary meatus to 1.5 cm, and clinical signs of infection were present. Eventually, the patient was transferred to a hospice facility where he died. CONCLUSION: This case study demonstrates the need for increased training of health care professionals in identifying risk factors for MDRPI and managing such injuries to limit their devastating impact on the patient and family members.
Penile erosion secondary to a medical device-related pressure injury (MDRPI) is preventable, understudied, not well understood, and often overlooked. Traumatic injuries to the penis due to indwelling urinary catheter use include urethral meatus pressure injuries, penile erosion, and cleaving of the penis. These traumatic urethral injuries tend to occur in people for whom long-term indwelling catheterization is prescribed, such as elderly men and men with spinal cord injuries.1,2
Penile pressure injuries, presenting as penile erosion and/or cleaving of the penis, can occur with indwelling urinary catheter use. Current guidelines continue to include urinary retention as an appropriate indicator for an indwelling urinary catheter in specific circumstances.3 Despite appropriate indications for use, urethral pressure injuries may result from urinary catheters.4,5 Cipa-Tatum et al stated that penile erosion was understudied and poorly understood.4 The authors suggested that penile trauma was due to long-term catheterization and improper securement that resulted in pressure and traction.4
Pittman et al defined a device-related, hospital-acquired pressure injury as “a localized injury to the skin and/or underlying tissue including mucous membranes, as a result of pressure, with a history of an external medical device at the location of the ulcer, and mirrors the shape of the device.”6(p154) A study by Barakat-Johnson et al found that device-related pressure injuries represented almost 30% of the surveyed pressure injury population.7 The Barakat-Johnson et al survey did not find urethral pressure injuries in the survey; their findings speak to the importance of medical devices as a source of adverse patient safety events.7 Pittman and Gillespie report the most common categories of devices that can cause a pressure injury include respiratory devices, tubes and drains, compression wraps, splints, and braces.8 In a cross-sectional study of 93 critical-care patients, da Silva Galetto et al found 20 patients (21.5%) developed urethral injuries due to a urinary catheter.9 Arnold-Long et al reported urinary/fecal tubes caused 17% of MDRPIs in their study of 304 inpatients.10 MDRPIs are associated with edema, low Braden and Glasgow Coma Scales, increased length of stay, poor perfusion, and poor nutrition.9,11-13 Bell indicated that medical devices as the cause of pressure injuries were often overlooked.1 This is consistent with the case study to follow.
Because urinary catheters are inserted through the urinary meatus into the urethra, they can cause mucosal pressure injury. Mucous membranes are very susceptible to pressure from medical devices that can lead to ischemia and injury.12,13 Accurate staging is an important factor in wound care and wound care research, but mucous membrane pressure injuries cannot be assessed using the same staging system used for those occurring on the skin surface due to the differences in the tissue anatomy that prevent differentiation between partial- and full-thickness tissue loss.13,14 Nonblanchable redness is not visible on mucous membranes.12,13 Though not stageable, mucosal pressure injuries are classified as pressure injuries and further described by location and causative device.12,13 Following the Edsberg et al recommendation,13 the description of a mucosal injury from a urinary catheter would be documented as a mucosal pressure injury to the urinary meatus caused by a medical device (urinary catheter tube). The purpose of naming the actual device facilitates follow-up analysis of the root cause and development of a preventive action plan.13
Shenhar et al suggest that meatal pressure injuries (MPIs) are a unique combination of skin and mucous membrane injury.15 The authors proposed a staging system that accommodates this combination. In their prevalence study including 168 male patients with indwelling catheters at a tertiary medical center, Shenhar et al found that 36% had some degree of MPI.15 MPIs can occur rather quickly.15,16 Applying the proposed staging system to their study participants, the authors found 4 cases of full-thickness skin and urethral mucosa loss of 2 cm or greater occurring between days 5 and 21 of urinary catheterization.15 Further research and guidance are needed to ensure MPI staging considers all layers of the skin and mucous membrane.
Patient vulnerability and body sites affected tend to make MDRPIs occur more rapidly than non-MDRPIs.17 Non-MDRPIs are related to the pressure caused by body weight, whereas MDRPIs are caused by devices that are held against the skin with tape or straps and are typically smaller and harder than skin and mucous membranes. Small devices can cause a pressure load against the skin of greater than 200 mm Hg.17 Many factors impact the likelihood of a medical device causing a pressure injury. These factors include:
- The shape, design, stiffness, and size of the device
- Limited guidance and awareness related to use and securement of devices
- A vulnerable patient population with comorbidities and fragile skin or edema17
As an MDRPI, trauma to the urinary meatus is considered a preventable hospital-acquired condition, making it an adverse patient safety event. A patient safety event is defined by The Joint Commission as “…an event, incident, or condition that could have resulted or did result in harm to a patient.”18(SE-5) The Joint Commission defines an adverse event as “..a patient safety event that resulted in harm to a patient.”18(pSE-5) Events and care before the injury should be examined to identify possible courses of preventive action to prevent future repetition of similar injuries.18
Here, the authors present the case of a 93-year-old man who developed an MDRPI secondary to an indwelling urinary catheter. The goal of this presentation is to describe this case, identify possible causes, and provide preventive solutions for traumatic urethral injuries. Informed consent was obtained from the patient’s family for the use of all health information relevant to this case. No pictures or identifiable information were included.
Case Report
A 93-year-old man was admitted to a local hospital due to a fall and a diagnosis of pneumonia. Typical for his age, the patient’s medical history was extensive. He had prostate cancer that did not respond to cryotherapy and continued to have an elevated prostate-specific antigen level. The patient had severe urinary retention that forced him to stand to void, and he could only void small amounts of urine with each effort. These frequent efforts to void compounded the shortness of breath from the pneumonia.
The patient’s urologist was consulted within 24 to 48 hours following admission and ordered placement of an indwelling urinary catheter. The authors could not confirm whether a bladder scanner was used before the insertion of the indwelling urinary catheter. After insertion, the catheter was secured to the inner right thigh with an adhesive-backed swivel retainer securement device. He continued to be placed in an incontinence brief due to incontinence of stool related to long-standing colitis and antibiotic therapy. Computed tomography (CT) of the pelvis and lower abdomen was ordered to investigate the urinary retention and bladder outflow restriction. The CT indicated a mass at the bladder neck. Further testing indicated metastasis of prostate cancer to the liver and spine. The decision was made to not treat the cancer. Over the next 10 days, the patient’s pneumonia weas brought under control, and discharge to a rehabilitation facility was scheduled.
Immediately following the patient’s transfer to the rehabilitation facility, his daughter (a registered nurse) assisted the attending nurse with incontinent care and noted a 1-cm erosion on the right side of the urinary meatus. The daughter also noted that the catheter securement device was still on the right thigh and had been there for the entire 2-week stay at the hospital. The daughter informed the nurse, but the transfer proceeded with no action taken.
Upon the patient’s arrival at the new facility, the daughter informed the staff of the urethral erosion. Within 24 hours, the daughter asked that the securement device be changed to the left side to decrease the pressure on the right urethral meatus. The only wound care measures consisted of the certified nursing assistants placing barrier cream on the wound. The securement device was changed to an elastic catheter leg band, but it remained on the right thigh. With each visit, the patient’s daughter found the securement device on the right side far more often than the left. Often, the urinary catheter was not even in the securement device.
The patient’s daughter notified the director of the facility that her father required wound care. Within a week of admission to the rehabilitation facility, the penile erosion encircled the urinary meatus, with the appearance of a fish mouth-shaped wound and diameter of 1.5 cm with scant amounts of bloody and purulent drainage. At this time, the daughter cleaned the wound herself and changed the urinary catheter securement device to the left side. The certified nursing assistant (CNA) entered the room and told the daughter that the urinary catheter bag could not be placed on the side of the bed that could be seen from the door. When asked why, the CNA said it was the “rule” of the facility.
Shortly afterward, the patient was transferred to a long-term care facility where he subsequently died while receiving hospice care. Certainly, the penile erosion did not cause his death; he was 93 years old with serious comorbidities. However, the sequence of events was disturbing to the family because they perceived they were not heard; there was a failure to pay attention and a lack of patient-centered care.
Discussion
There is minimal research on the prevention of penile erosion.16,19 Much of the information and guidance is based on expert opinion. Avoidance of long-term urinary catheters is the obvious solution but not always possible, as in this patient’s case.12,19 Penile pressure injuries do not respond to the topical wound care methods typically used for cutaneous tissue.1 The treatment for severe penile erosion or cleaving is surgical reconstruction or urinary diversion.1
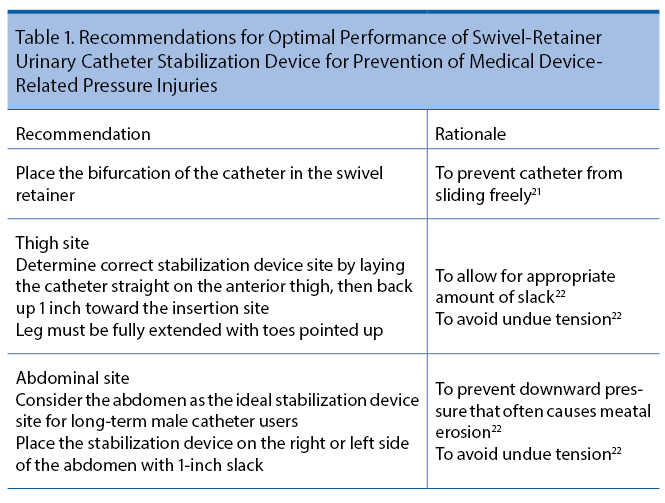
Thorough assessment is essential in the prevention of urethral trauma.4,7,8 The urethral meatus on all sides of the catheter tube should be assessed at least every 12 hours by a registered nurse (RN).12,14,20 Small urethral trauma can progress to deep penile injuries in a short time.9 In the case of this patient, the deeper injury occurred within 1 week of the discovery of the penile pressure injury. While assessing the skin of the penis, the RN should also assess the securement device to ensure the catheter is being correctly stabilized.1,12 The manufacturer of the swivel retainer urinary catheter provides recommendations and rationales for correct use of their product (Table 1). Manufacturers of other catheter securement devices have similar recommendations. One manufacturer of a leg band catheter securement device recommends securing the catheter to the inner thigh and leaving an ample loop above the band to prevent traction on the catheter.23 The instructions further state the leg band can be rotated and secured on alternating lower extremities to prevent irritation to the urinary meatus and promote patient comfort.23 The manufacturer instructions for a nonswivel adhesive-backed anchoring catheter device state the device should be placed on the upper thigh with the leg fully extended, leaving 1 inch of slack between the device and the urinary meatus.24
Although not mentioned in the literature, the use of adult incontinence briefs may have further contributed to the rapid development of the meatal injury and erosion. To the patient’s daughter, the adult incontinence brief appeared to be placed on the patient with no regard to the position of the catheter, often causing traction on the tubing. Further, the constant presence of the incontinence brief may have limited assessment of the position of the catheter and the condition of the urinary meatus. The use of incontinence briefs tends to hold in heat and humidity, which would alter the microclimate (temperature, humidity, and airflow) and enhance tissue disruption.17 In their 2018 article regarding use of adult incontinence briefs in hospitalized adults and the elderly, Bitencourt et al found instances of the concurrent use of indwelling urinary catheters and incontinence briefs. However, they found no studies related to the use of the two incontinence technologies.25
Appropriate securement of an indwelling catheter is recommended to decrease urethral injuries.1,26,27 The catheter tubing can be secured to the lower abdomen or thigh.4,21,22 These recommendations are generally based on expert opinion and the logical assumption that inappropriate use of the securement device could put traction or pressure on the urethral tissue.12,24 In a small study published in 2013, Rassin et al found performing urinary catheter care with soap and water, assessing the meatus, and alternating the catheter tubing from the right to left thigh every 8 hours decreased development of meatal pressure injury compared with the group of patients receiving catheter care only once daily.16 The control group had a pressure injury rate of 67.3%, and the group receiving the intervention had a pressure injury rate of 38.6% (P = .002).16 The manufacturers of one adhesive-backed urinary catheter stabilization device recommend changing the device at least every 7 days.21 The 2019 International Guidelines recommended at the level of expert opinion that medical securement devices be monitored and adjusted more than 2 times per day as indicated in patients at high risk for pressure injury.12 This recommendation substantiates the request of this patient’s daughter that the location of his urinary catheter securement device be moved periodically from the right thigh.
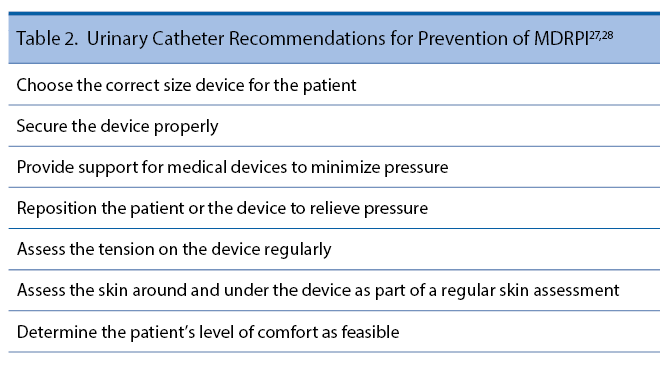
All nursing staff need to be educated on the risk for penile injury from urinary catheterization. Emphasis should be placed on frequent assessment of the tubing where it comes in contact with the skin and mucous membrane, proper use of the stabilization device to prevent traction and pressure on the meatus, and scrupulous care of the meatal membranes. The study by Rassin et al confirms that counseling the nursing staff to be aware of the position of the catheter at all times can mitigate unnecessary meatal pressure injury.16 The aforementioned International Guidelines from 2019 made other specific recommendations to decrease the incidence of MDRPIs (Table 2).28
Gefen et al go a step further to recommend that health care facilities have a care bundle approach to prevent MDRPIs.17 The care bundle they recommend is based on their study of a bundle approach to reduce tracheostomy-related pressure injuries, which successfully decreased MDRPIs from 8.1% to 2.3%.17 The trach bundle included a daily total skin assessment as well as a device assessment every 8 hours.17 The care bundle was integrated into the facility’s electronic health record to ensure it would be part of the nurses’ plan of care.17 Such a bundle could be developed for any medical device and any facility. Gefen et al recommended that facilities have a document on file for each medical device used in the facility that includes detailed information on how to use and secure the device.17 Clinicians need clear guidance from manufacturers and hospital educators on use and securement of devices as well as information regarding the importance of repositioning devices to offload pressure.17 The authors of the present case study are unaware of the existence of a care plan related to this patient’s skin care or medical device. Having a care bundle in place and backed by clinician awareness could have prevented the development of this patient’s pressure injury.
This case presents a challenging situation in which the patient clearly needed a urinary catheter, but actions to prevent an MDRPI were not taken. The patient’s clinical picture demonstrates the challenge of determining goals of care in palliative or end-of-life situations. The goal of care in palliative situations is to improve the quality of life for both the patient and the family.29 In this case study, the wound worsened, and both the patient and family were affected. Moreover, prevention of injury and patient-centered care should always be a primary goal of care.
Conclusion
There is substantial research available on pressure-related injuries, ranging from prevention to management. An MDRPI is a pressure injury. Urethral erosion due to the pressure from a urinary catheter is an MDRPI that should not happen. This MDRPI caused undue discomfort for the patient and stress for the family because they perceived they were not heard; there was a failure by staff to pay attention and a lack of patient-centered care. Ultimately, this type of pressure injury is preventable but often overlooked as described in the case study. This case study highlights the fact that there is a gap in the knowledge, understanding, and management of urethral erosion secondary to an MDRPI. In conclusion, this case study demonstrates that there is a need for increased research, awareness, and education on MDRPIs related to pressure from an indwelling urinary catheter.
Author Affiliations
Brenda K. Woodmansee, DNP1; and Jennifer A. Anderson, DNP, CNL-BC1
1College of Nursing, University of South Alabama, Mobile, AL
References
1. Bell MA. Severe indwelling urinary catheter-associated urethral erosion in four elderly men. Ostomy Wound Manage. 2010:56(12):36-39.
2. Bhat AL, Bhat N, Khandelwal N, Bhat A, Singh T. Catheter-induced urethral injury and tubularized urethral plate urethroplasty in such iatrogenic hypospadias. Afr J Urol 2020;26(17):1-5. doi: https://doi.org/10.1186/s12301-020-00030-z
3. AHRQ. Toolkit for Reducing Catheter-associated Urinary Tract Infections in Hospital Units:Implementation Guide. AHRQ. Pub No. 15-0073-2-EF. September 2015. Accessed January 22, 2022. https://www.ahrq.gov/sites/default/files/publications/files/implementation-guide_0.pdf
4. Cipa-Tatum J, Kelly-Signs M, Afsari K. Urethral erosion: a case for prevention. J Wound Ostomy Continence Nurs. 2011;38(5):581-583. doi:10.1097/WON.0b013e31822b3280
5. Young A, Mitacek, R. Penile erosion in a paraplegic man with indwelling urinary catheter and scrotal edema. Urol Case Rep. 2017:12:62-63. doi:10.1016/j.eucr.2017.03.001
6. Pittman J, Beeson T, Kitterman J, Lancaster S, Shelly A. Medical device-related hospital-acquired pressure ulcers; development of an evidence-based position statement. J Wound Ostomy Continence Nurs. 2015;42(2):151-154. doi:10.1097/WON.0000000000000113
7. Barakat-Johnson M, Barnett C, Wand T, White K. Medical device-related pressure injuries: An exploratory descriptive study in an acute tertiary hospital in Australia. J Tissue Viability. 2017;26(4):246-253. doi:10.1016/j.jtv.2017.09.008
8. Pittman J, Gillespie C. Medical device-related pressure injuries. Crit Care Nurs Clin North Am. 2020;32(4):533-542. doi:10.1016/j.cnc.2020.08.004
9. da Silva Galetto SG, do Nascimento ERP, Hermida PMV, Busanello J, de Malfussi LBH, Lazzari DD. Medical device-related pressure injuries in critical patients: prevalence and associated factors. Article in English and Portuguese. Rev Esc Enferm USP. 2021;55:e20200397. doi:10.1590/1980-220X-REEUSP-2020-0397
10. Arnold-Long M, Ayer M, Borchert, K. Medical device-related pressure injuries in long-term acute care hospital setting. J Wound Ostomy Continence Nurse. 2017;44(4):325-330. doi:10.1097/WON.0000000000000347
11. The Joint Commission. Quick Safety 43: Managing medical device-related pressure injuries. July 23, 2018. Accessed January 22, 2022. https://tinyurl.com/yck59w3k
12. European Pressure Ulcer Advisory Panel, National Pressure Injury Advisory Panel, Pan Pacific Pressure Injury Alliance. In: Haesler E, ed. Prevention and Treatment of Pressure Ulcers/Injuries: Clinical Practice Guideline. The International Guideline. EPUAP/NPIAP/PPPIA; 2019.
13. Edsberg LE, Black JM, Goldberg M, McNichol, L, Moore, L, Sieggreen M. Revised national pressure ulcer advisory panel pressure injury staging system: revised pressure injury staging system. J Wound Ostomy Continence Nurs. 2016:43(6):585-597. doi:10.1097/WON.0000000000000281
14. Delmore BA, Ayello EA. CE: pressure injuries caused by medical devices and other objects: a clinical update. Am J Nurs. 2017;117(12):36-45. doi:10.1097/01.NAJ.0000527460.93222.31
15. Shenhar C, Mansvetov M, Baniel J, Golan S, Aharony S. Catheter-associated meatal pressure injury in hospitalized males. Neurolurol Urodyn. 2020;39:1456-1463. doi:10.1002/nau.24372
16. Rassin M, Markovski I, Fishlov A, Naveh R-U. An evaluation of preventing pressure ulcers in the urinary meatus. Dimens Crit Care Nurs. 2013;32(2):95-98. doi:10.1097/DCC.0b013e31826bc65f
17. Gefen A, Alves P, Ciprandi G, et al. Device-related pressure ulcers: SECURE prevention. J Wound Care. 2020;29(suppl 2a):S1-S52. doi:10.12968/jowc.2020.29.Sup2a.S1
18. The Joint Commission. Sentinel events. Comprehensive Accreditation Manual for Hospitals: Update 1. January 2021. Accessed February 20, 2022. https://www.jointcommission.org/-/media/tjc/documents/resources/patient-safety-topics/sentinel-event/camh_24_se_all_current.pdf
19. LeBlanc K, Christensen D. Addressing the challenge of providing nursing care for elderly men suffering from urethral erosion. J Wound Ostomy Continence Nurs. 2005;32(2):131-134. doi:10.1097/00152192-200503000-00011
20. Black JM, Cuddigan JE, Walko MA, Didier LA, Lander MJ, Kelpe MR. Medical device related pressure ulcers in hospitalized patients. Int Wound J 2010; 7(5):358-365. doi:10.1111/j.1742-481X.2010.00699.x
21. BARD Medical. StatLock® foley stabilization device: tips to optimize performance. Accessed January 22, 2022. https://www.healthproductsforyou.com/ProdImages/CommonFile/Tips-to-Optimize-StatLock-Performance.pdf
22. BARD. StatLock® foley stabilization device: frequently asked questions. Urotoday.com. Accessed February 20, 2022. https://www.urotoday.com/images/catheters/tools/faqs.pdf
23. Dale Medical Products. Dale® Hold-n-Place® Foley catheter leg band. 2020. Accessed April 21, 2022. https://www.dalemed.com/assets/316-hold-n-place-leg-band-instructions-english.pdf
24. MC Johnson Co. Cath Secure® rationale and fact sheet. Accessed April 21, 2022. https://mcjohnson.com/wp-content/uploads/2021/11/Cath-Secure-Rationale-and-Fact-Sheet.pdf.
25. Bitencourt GR, Alves LAF, Santana RF. Practice of use of diapers in hospitalized adults and elderly: cross-sectional study. Rev Bras Enferm. 2018;71(2):343-349. doi:10.1590/0034-7167-2016-0341
26. Fisher J. The importance of effective catheter securement. Br J Nurs. 2010:19(18):S14-S18. doi:10.12968/bjon.2010.19.Sup8.79064
27. Wound, Ostomy, and Continence Nurses Society (WOCN). Care and management of patients with urinary catheters: a clinical resource guide. 2015. Accessed February 17, 2022. https://cdn.ymaws.com/member.wocn.org/resource/resmgr/document_library/Care_&_Mgmt_Pts_w_Urinary_Ca.pdf
28. European Pressure Ulcer Advisory Panel, National Pressure Injury Advisory Panel, Pan Pacific Pressure Injury Alliance. In: Haesler E, ed. Prevention and treatment of pressure ulcers/injuries: quick reference guide. EPUAP/NPIAP/PPPIA; 2019. Accessed January 22, 2022. https://internationalguideline.com/static/pdfs/Quick_Reference_Guide-10Mar2019.pdf
29. Vickery J, Compton, L, Allard J, Beeson T, Howard J, Pittman, J. Pressure injury prevention and wound management for the patient who is actively dying: evidence-based recommendations to guide care. J Wound Ostomy Continence Nurs. 2020;47(6):569-575. doi:10.1097/WON.0000000000000702