



A Single-Center Pilot Study Investigating the Effects of a Native Cross-Linked Extracellular Matrix with Polyhexamethylene Biguanide to Manage Chronic Lower Extremity Wounds Exhibiting Bacterial Contamination
Abstract
BACKGROUND: Elevated bacterial bioburden and biofilm formation are common causes for delayed wound healing. Biofilm is an assemblage of surface-associated microbes enclosed in a self-produced matrix. Identifying and managing biofilm is a crucial component of successful wound care protocols. PURPOSE: To determine the effects of a native cross-linked extra cellular matrix with polyhexamethylene biguanide (PHMP; PHMP antimicrobial [PCMP]), in conjunction with next-generation DNA sequencing (NGS) and targeted debridement by fluorescence imaging, on managing bacterial bioburden to support wound healing. METHODS: Over 6 weeks, fluorescence images were captured to assess bacterial contamination as were standard images with measurements. Tissue swabs were obtained and analyzed using NGS to quantify bacterial bioburden. PCMP was applied at each treatment visit. RESULTS: Baseline wound duration was 23.0 ± 6.7 weeks, and baseline size was 7.9 ± 7.1 cm2. Two out of 5 wounds healed by week 4. The mean percentage area reduction of all wounds was 59.7% by week 4 and 78.1% by week 6. All wounds were fluorescence positive on week 1 and fluorescence negative by Week 4. CONCLUSION: PCMP, as an antimicrobial barrier, combined with use of a real-time method of bacterial detection, may be beneficial in managing the wound healing environment.
Wounds become chronic for a myriad of reasons and frequently stall in the inflammatory phase of healing.1,2 A multitude of systemic and local factors can contribute to wound stalling, including the accumulation of bacterial bioburden.3,4 Open wound surfaces are susceptible to micro-colonization by pathogenic, planktonic bacteria which worsen wound status as their concentration increases, commonly measured in colony forming units per gram of tissue (CFU/g).5-9 Bacterial loads of ≥104 CFU/g are capable of impairing wound healing, while wounds with bacterial loads of >105 CFU/g are generally classified as clinically infected.7,10 Making matters worse, the accumulation of bacteria can be furthered by the presence of devitalized tissue leading to creation of a nidus for bacterial growth.11
Accumulation of bacterial bioburden can result in the formation of biofilm.5 Biofilm is one of the most common causes of wound stalling in the inflammatory phase, and occurs in up to 90% of chronic wounds.12-15 In 6 to 12 hours after micro-colonization, extracellular polymeric substances (EPS) form and negate host immune response against colonized bacteria.16,17 Within 24 to 72 hours, the colonized bacteria can evolve into fully formed biofilm colonies, causing elevated matrix metalloproteinases (MMPs), further EPS growth, and bacterial proliferation.5,18,19 This creates a positive feedback loop of host immune response, inability to endogenously remove biofilm, biofilm expansion, and chronic inflammation.5,16-18 Ultimately, this culminates in the inability to escape the inflammatory phase and wound chronicity. Once chronic, wounds can result in both burdensome treatment costs and negative health outcomes. Currently, such biofilms cannot be analyzed and grown in the lab due to the complex growth requirements of these structures.20 However, using molecular-based techniques such as next-generation DNA sequencing (NGS), the bacterial and fungal components of these biofilms can be identified and quantified.21
An estimated 8.2 million Medicare beneficiaries suffer from chronic wounds, leading to $28 to $97 billion in annual expenditures.22 The cost of a single chronic wound ranges from approximately $3400 to $11,800 in average Medicare spending.22 However, many chronic wounds fail to heal and compound treatment costs. In total, biofilm is estimated to carry an annual cost of $94 billion, of which $12.1 billion stems from chronic wounds.23 Thus, wounds that develop biofilm carry the potential for significant economic burden. Specifically, biofilm and subsequent infections can increase treatment cost via prolonged wound care and development of severe outcomes, such as sepsis and amputation.24,25 Preclinical evidence has demonstrated an average of 41% less closure in diameter of biofilm-laden wounds over 28 days,26 while the healing time of biofilm-laden wounds was shown to be double that of those without (8 weeks vs. 4 weeks).27 Treatment of biofilm in a diabetic foot ulcer (DFU) is estimated to cost approximately $4800.28 Whereas treatment of sepsis or amputation ranges in cost from an estimated $16,300 to $38,300 and approximately $38,000 to $54,000, respectively.29,30 Therefore, effective treatment of biofilm is warranted to reduce healing time, prevent severe health outcomes, and lower treatment costs.
Successful biofilm treatment is complicated by the difficulty of bacterial detection and the presence of antibiotic resistance. Standard clinical practice dictates the use of debridement to disrupt biofilm and reduce the potential for bacterial nidus by removing devitalized tissue.31-33 However, the degree of post-debridement bacterial removal cannot be confirmed via the naked eye.16 It is possible to detect bacterial presence using a tissue swab or wound biopsy post-debridement, but results can take days and allow for biofilm reformation.18,31 Some evidence suggests that up to 29% of the tissues across the wound bed and periwound region were positive for bacteria post debridement.34 Other nonmechanical treatments for biofilm, such as antibiotics, can be inhibited by the EPS. The negative ion structure of the EPS acts as an anionic blockade against cationic antibiotics.35 The EPS also allows for bacterial proximity and the ease of horizontal transfer of resistance-conferring genes.36 Even if the EPS is disrupted by debridement, biofilm contains metabolically inactive “persister bacteria,” which may not be sensitive to antibiotic treatment.37 Overall, treatment of biofilm may be improved with modalities that can prevent its formation/reformation by eliminating and/or preventing the accumulation of bacterial bioburden. Conceivably, the combination of a real-time method of bacterial detection for targeted debridement with a non-cytotoxic, bacteria-sensitive treatment may achieve this goal.
Real-time detection and antimicrobial stewardship in the management of bacterial bioburden may be attainable with the use of non-contact fluorescence imaging and topical antimicrobials such as polyhexamethylene biguanide (PHMB). Fluorescence imaging provides immediate bacterial detection that is otherwise invisible to the naked eye, eliminating the waiting time necessary for a biopsy or swab test.38 Simultaneously, this reduction in waiting time may help to reduce treatment cost via early detection and selection of effective treatment courses.39 Fluorescence imaging devices can visualize red or cyan fluorescence from bacteria by virtue of bacterial porphyrin or pyoverdine production, respectively.38,40,41 This includes 87.5% of the most common wound pathogens such as Pseudomonas aeruginosa.42 This is paired with high detection accuracy, as positive predictive values for fluorescence imaging are reported at >95% for bacterial loads ≥104 CFU/g.38,43 Precise identification of bacterial bioburden may lead to greater bacterial removal via targeted debridement. However, on its own, even the most precise debridement is not sufficient for management of bacterial bioburden.
Topical PHMB possesses multiple mechanisms of action that are effective in the management of bacterial bioburden. Using direct physical contact, positively charged PHMB polymers interact with and penetrate negatively charged bacterial membranes.44,45 The compromise in membrane structural integrity leads to bacterial cell death while avoiding the spread of cytotoxicity to non-bacterial cells.35,46 PHMB is a broad-spectrum antimicrobial without any known bacterial resistance.47 PHMB has also been combined with native cross-linked extracellular matrix (PCMP; PuraPly AM, Organogensis Inc) as an antimicrobial barrier to manage bacterial bioburden. As an FDA 510(k)-cleared Class II medical device, PCMP is indicated for the management of chronic and acute ulcers of various etiologies. The cross-linked type 1 collagen contained in PCMP is coated with PHMB allowing for resistance to proteolytic degradation.48 Overall, the antimicrobial barrier effect of PCMP serves as a bridge between debridement to eliminate and/or prevent accumulation of bacterial bioburden and the possibility of biofilm formation/reformation. The authors hypothesize that management of bacterial bioburden with PCMP may help to support an ideal wound healing environment in this cohort of patients.
Taken together, the purpose of this study was to determine the effects of PCMP as an antimicrobial barrier, in conjunction with NGS and targeted debridement by fluorescence imaging, on managing bacterial bioburden to support wound healing.
Methods
Participants
All participants included in this prospective, single-center, open-label pilot study were ≥18 years of age, had a non-healing lower extremity wound present for ≥4 weeks, had a wound that failed ≥1 wound care treatments and was 5 cm2 to 25 cm2, had adequate circulation to their affected foot (ABI >0.8), and had a wound that showed positive fluorescence (red, cyan, or both). Participants included also completed an informed consent form, were willing and able to follow protocol requirements, and had no known sensitivity to porcine or collagen-derived products and PHMB. Participants were excluded from participation if cancer or clinical signs of infection were suspected in the wound site (eg, erythema, swelling, local warmth); other concurrent conditions were present that may compromise the participant’s safety; the participant was pregnant, breastfeeding, or planned on either during the trial; or the participant was concurrently enrolled in another clinical trial involving an investigational drug or device. Participants were also excluded if their wound was treated with tissue engineered materials or other scaffold products ≤30 days prior to treatment, had taken antibiotics within 7 days of enrollment, or had a wound that was a third-degree burn. The study was conducted in accordance with Health Insurance Portability and Accountability Act guidelines, adhered to tenets of the International Conference on Harmonization E6 Good Clinical Practice (ICH GCP) and the Declaration of Helsinki, and received ethics approval by an external institutional review board.
Study Design
The study was divided into a Screening Phase and a Treatment Phase that spanned over 6 weeks. An End of Study Visit (EOS) was scheduled on week 7, or earlier if the wound healed. Participants were seen at weekly intervals (7 ± 3 days) for the 6-week treatment period. Each visit was scheduled with reference to the allowed visit window (7 ± 3 days) from the treatment visit 1 date. Participants whose wound closed during the study or completed the treatment phase, but their wound did not heal, were considered as having completed the study. Participants who did not complete the treatment phase and had an unhealed wound were considered as not completing the study. The primary outcome assessed was the percentage decrease in wound bacterial bioburden at week 6 relative to baseline measurements. Secondary outcomes included the number of subjects that achieved complete wound closure (CWC) by weeks 4 and 6, and the percentage change in the wound area at weeks 4 and 6 relative to baseline measurements.
The screening phase of the study began with a screening visit (day 0) to determine participant eligibility for enrollment in the treatment phase. Informed consent was reviewed and signed by each participant followed by the collection of demographics, surgical history, and concomitant medications/therapies. Each participant then had a physical exam followed by an assessment of study wound history and infection status adapted from the International Wound Infection Institute (IWII). Only one wound was selected by the principal investigator (PI) as the study (target) wound. If multiple wounds were present, the largest that met eligibility criteria was selected. All wounds were photographed twice pre-debridement using non-contact fluorescence imaging (MolecuLight i:X; MolecuLight Inc). First, a standard photograph and measurement were taken followed by a photograph to confirm presence of fluorescence in the wound. The screening visit concluded with a review of inclusion and exclusion criteria. If deemed eligible, participants were enrolled in the treatment phase of the study.
The Treatment Phase lasted until the wound was healed or a maximum of 5 applications of PCMP plus standard of care (SOC) were completed. Potential adverse events, wound infection status, and concomitant medications/therapies were assessed during each treatment visit. Treatment visit 1 (day 0) was conducted on the same day as the Screening Visit and proceeded enrollment. The target wound was debrided, and a tissue swab was collected followed by capture of a standard and fluorescence photograph. All tissue swabs were analyzed by an independent testing lab (Pangea Laboratory). PCMP and SOC dressings were then applied according to product labeling. Treatment visits 2 through 6 included standard and fluorescence photographs taken pre- and post debridement and application of PCMP and SOC dressings. Another tissue swab was taken at treatment visit 6 if the wound remained unhealed.
All EOS visits were conducted in the same manner as treatment visits 2 through 6 with minor differences. For wounds that were healed, the EOS visit ended after capture of a standard photograph. Participants then reviewed and signed a completion of study exit form and were discharged from the study. For wounds that remained unhealed, the EOS visit ended after application of SOC dressings to the wound. Participants then reviewed and signed a completion of study exit form and were discharged from the study back to SOC treatment as prescribed by the PI.
Standard of Care
The SOC therapy in this study was cleansing with normal saline solution (NSS), debridement if clinically indicated, appropriate dressing to maintain moist wound environment (eg, plain calcium alginate and foam, rolled sterile gauze, self-adherent elastic wrap), offloading for DFU’s in weight-bearing areas, and compression for venous leg ulcers (VLUs). The choice of offloading was at the discretion of the PI but was either total contact casting, fixed ankle walker boot, or an equivalent device to the fixed ankle walker boot. During treatment visits, all dressings were removed, and the foot was washed with NSS; wound cleansers were prohibited. Ulcers were gently irrigated prior to each dressing change with the leg elevated for as much time as possible. During the treatment phase, cleansing and debridement were done prior to the application of PCMP.
Wound Imaging
The fluorescence imaging camera system uses a narrow band of safe violet (405 nm) light to maximize fluorescence signals from tissues and bacteria. The device employs proprietary optical filters to eliminate unwanted fluorescence wavelengths to detect the resulting fluorescence on an imaging sensor and display it on a screen in real time. The result is an image that depicts regions of tissue (typically green) and regions of bacteria (red or cyan) in a wound site. The colored regions of the wound aided in targeted debridement. The protocol for capturing images has been previously described.31 Briefly, all images were captured by a wound care clinician previously trained on device use and image interpretation.40,49 All images were captured according to the manufacturer’s directions.50 The captured fluorescence images were then used to determine presence and location of bacterial loads ≥104 CFU/g.38 A determination of fluorescence-positive (red or cyan, ‘FL+’) or negative (‘FL-‘) was then made for each wound. A determination of FL- did not influence whether PCMP was or was not subsequently applied.
NGS Microbiome Analysis
Samples were collected using the collection kit provided with the PrecisionBIOME NGS Microbial test (Pangea Laboratory). This kit contains sterile swabs and collection tubes pre-filled with a nucleic acid-stabilizing solution called DNA/RNA Shield (Zymo Research Corp.). This solution can preserve the microbial DNA present in the specimen at room temperature for up to 30 days. For sample collection, swabs were rotated in a zigzag position from wound edge to wound edge with enough pressure to produce fluid from the wound tissue. Immediately after sample collection, the swab was placed inside the collection tube and the rest of the swab stem was discarded at the breakpoint. Tubes were tightly capped and sent for 16S and ITS analysis through the PrecisionBIOME NGS Microbial test.
DNA Extraction, Library Preparation, and Sequencing
Shortly after collection, specimens were sent for analysis through the PrecisionBIOME NGS Microbial Test, an NGS test that provides accurate and fast identification and quantification of both bacterial and fungal species present in a clinical specimen along with antibiotic susceptibility information. Briefly, microbial DNA from the specimen was extracted using the ZymoBIOMICS DNA Miniprep Kit according to the manufacturer’s instructions (Zymo Research Corp). Extracted DNA was next prepared for NGS analysis following a workflow which included library preparation using the Quick-16S NGS library prep kit (Zymo Research Corp), sequencing of barcoded amplicons with the MiSeq sequencing platform (Illumina), and bioinformatics analysis using a proprietary PrecisionBIOME bioinformatics pipeline capable of producing species-level resolution of bacterial and fungal sequences. Positive and negative controls (transport medium alone and unused swabs) were also included in the NGS workflow. To control for contamination, cell and DNA mock communities were used as positive controls (ZymoBIOMICS microbial community standard, catalog Nos. D6300 and D6305; Zymo Research Corp.) from the DNA extraction process. ZymoBIOMICS Microbial Community Standard (Zymo Research Corp.) was used as a positive control to monitor the performance of all steps of the NGS workflow including the bioinformatic analysis. Potential sequencing errors and chimeric sequences were also removed with the DADA2 pipeline. Absolute abundance of total bacteria and fungi was determined using the Femto Bacterial and Fungal DNA Quantification kits (Zymo Research Corp) according to manufacturer’s protocols.
Analysis of Microbiota
Microbiota profiling was determined using the PrecisionBIOME bioinformatics analysis pipeline. UCLUST was used to perform taxonomic classifications using a PrecisionBIOME custom proprietary database. Phylotypes were computed as percent proportions based on the total number of sequences in each sample. Relative abundances of bacteria compared to fungi were determined assuming an equivalency of one 16S rDNA copy to one fungal ITS copy. While it is unlikely that the number of 16S or ITS copies change in any given taxa, this is an assumption, which may be considered a limitation of the analysis presented here. Absolute microbial quantification was achieved using a real-time polymerase chain reaction approach using primers targeting the V1-V3 and ITS regions for bacterial and fungal quantification, respectively. Species level resolution of this sequencing approach was previously confirmed by shotgun sequencing.51
Statistical Analysis
Descriptive statistics were expressed as mean ± SD. Mean, SD, or percentage change/reduction were calculated for primary and secondary outcomes.
Results
A total of 5 participants (2 men and 3 women) were assessed over the 6-week protocol. Participant age was 66.4 ± 14.5 years. Wound types included were VLU (n = 3), DFU (n = 1), and iatrogenic (n = 1). Wound duration prior to enrollment was 23.0 ± 6.7 weeks. Wound locations were on the left lower extremity (LLE; n=3) and the left heel (n = 2). Fitzpatrick Scale Type included I (n = 2), II (n = 2), and V (n = 2). All wounds were FL+ at week 1 and were FL- by week 4. At week 2, 2 wounds were FL- while 3 wounds were FL- within the wound and FL+ in the periwound. At week 3, 4 wounds were FL- and 1 wound was FL- within the wound and FL+ in the periwound. The mean bacterial cell count for all wounds at baseline measurement was 3.4 x 107 ± 6.5 x 107 CFU. Two wounds that healed prior to Week 6 only had tissue swabs during baseline measurement. Therefore, 3 unhealed wounds had bacterial cell counts for baseline measurement and week 6. Mean bacterial cell count for the unhealed wounds at baseline measurement was 5.1 x 107 ± 8.6 x 107 CFU and was 5.1 x 105 ± 3.5 x 105 CFU at week 6, equating to a percentage reduction of 99% (Figure 2). Mean bacterial cell count for healed wounds at baseline measurement was 8.3 x 106 ± 8.0 x 106 CFU.
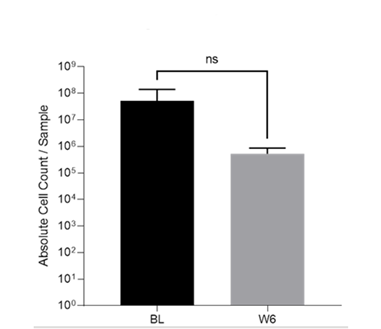
BL: baseline, W6: week 6.
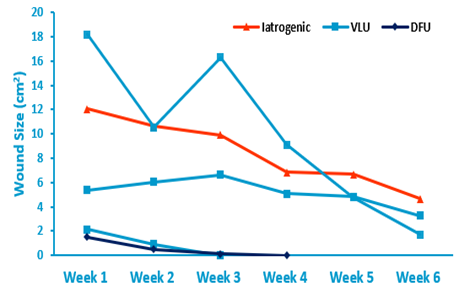
Mean wound area at baseline measurement for all wounds was 7.9 cm2 ± 7.1 cm2. By week 4, 2 wounds achieved CWC, and the remaining 3 wounds had a mean wound area of 7.0 cm2 ± 2.0 cm2. By week 6, the remaining 3 wounds had a mean wound area of 3.2 cm2 ± 1.5 cm2 leaving 3 wounds that did not achieve CWC. At week 4, average percentage reduction in wound area compared to baseline measurement was 59.7%. The average percentage reduction in wound area compared to baseline measurement was 78.1% at week 6. The average weekly percentage reduction in wound area was 42.4% for all wounds. The average weekly percentage reduction in wound area for wounds that achieved CWC was 79.9%. The average weekly percentage reduction in wound area was 17.5% for unhealed wounds. Nearly all wounds (n = 4) achieved a percentage reduction in wound area of >40% by week 6.
Patient 1
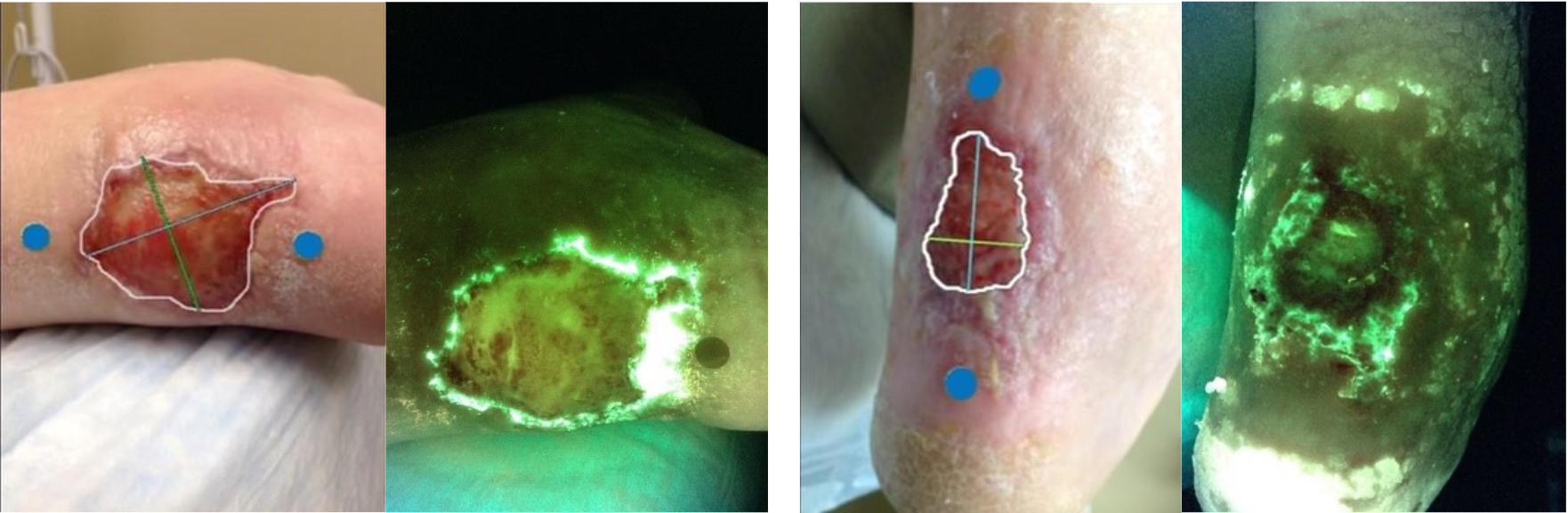
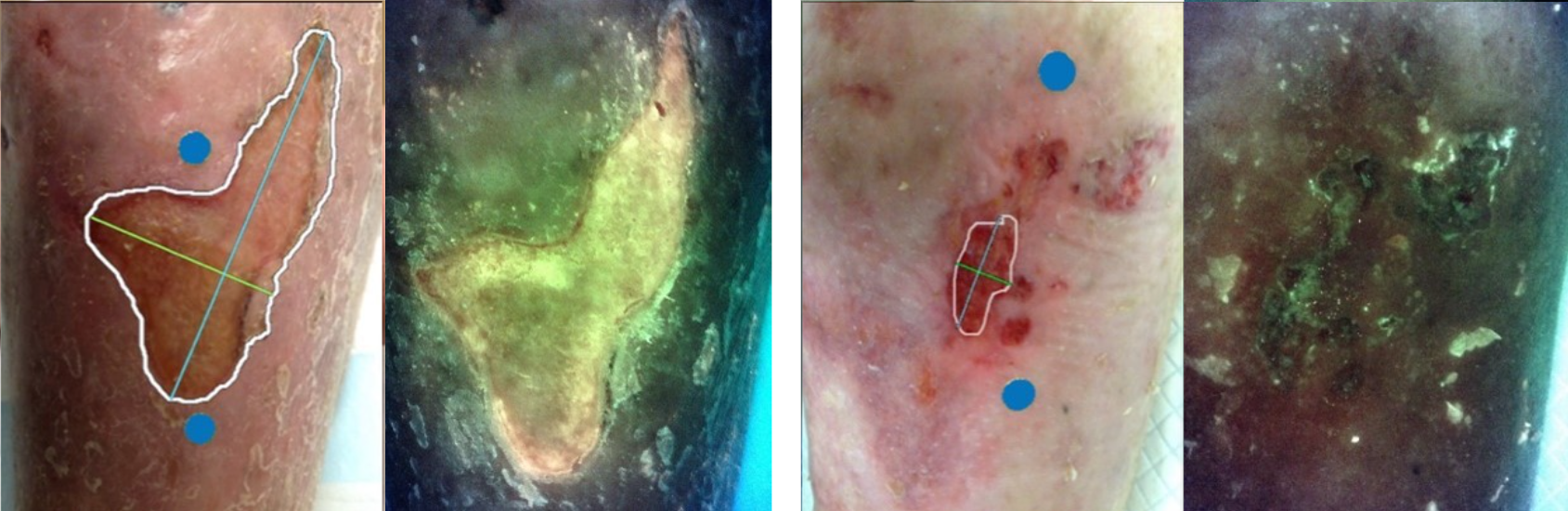
A 72-year-old male with a history of hypertension, degenerative joint disease, hypercholesterolemia, atrial fibrillation, and benign hypertrophy of the prostrate presented with an iatrogenic wound to his posterior left heel. The patient had a history of a broken tibia treated with casting that rubbed against the affected area and caused the wound. At initial presentation, the duration of the wound was 14 weeks, measured 12.06 cm2, and had a Fitzpatrick Score of II. In addition, the wound was FL+ in both the wound and periwound regions (Figures 1 and 3). By week 4, the wound measured 6.83 cm2, equating to a 43.4% area reduction. By week 6, the wound measured 4.68 cm², equating to a 61.2% area reduction over the course of the study. The wound became FL- at week 2 and remained FL- for the remaining duration of the trial (Figures 1 and 3).
Patient 3
A 62-year-old male with a history of angina, hypertension, hypercholesterolemia, peripheral vascular disease, degenerative joint disease, coronary artery disease, deep vein thrombosis, spinal stenosis, and dyspnea presented with a VLU to his LLE. At initial presentation, the duration of the wound was 31 weeks, measured 18.21 cm2, and had a Fitzpatrick Score of II. In addition, the wound was FL+ in both the wound and periwound regions (Figures 1 and 4). By week 4, the wound measured 9.12 cm2, equating to a 49.9% area reduction. By week 6, the wound measured 1.74 cm2, equating to a 90.4% area reduction over the course of the study. At Week 2, the wound became FL- in the wound but remained FL+ in the periwound region. At week 4, the wound became FL- in both the wound and periwound regions and remained FL- the remaining duration of the trial (Figures 1 and 4).
Discussion
Biofilm stands as one of the chief causes of wound chronicity, carrying the potential for significant economic burden and severe health outcomes.12-16,23-25 Treatment of biofilm is complicated by its rapid reformation and antibiotic resistance.16,35-37 Non-cytotoxic, bacteria-sensitive treatments paired with real-time detection of bacterial bioburden for targeted debridement may present the opportunity for early detection and effective management of bacterial bioburden. As a result, the formation/reformation of biofilm may be prevented allowing progression of wounds toward closure. This could result in improved patient outcomes and a reduction in both healing time and treatment cost. The results of this pilot study provide preliminary evidence for the use of fluorescence imaging for targeted debridement combined with PCMP as an antimicrobial barrier in support of bioburden management and wound closure. Fluorescence imaging allowed for targeted debridement and maximal removal of bacterial bioburden while PCMP served to support an ideal environment for wound healing by managing bacterial bioburden. Overall, wound management with PCMP and fluorescence imaging had a positive effect on 5 hard-to-heal wounds over 6 weeks.
Both pre-enrollment wound duration and FL+ at baseline measurement seemed to indicate that all wounds were suffering from bacterial bioburden-induced wound chronicity. While a multitude of factors can cause a wound to stall in the inflammatory phase, a transition of FL+ to FL-, coinciding with wound area reduction, supports this proposition. After SOC and PCMP treatment, wounds that had a duration of 23.0 ± 6.7 weeks either attained CWC (n = 2), experienced a ≥40% area reduction by week 6 (n = 2), or approached 40% area reduction by week 6 (n = 1; 39.11%). The simultaneous transition of FL+ to FL-may indicate a relationship between reduction of bacterial bioburden and progression of wound healing. This observation is supported by previous studies demonstrating that PCMP as an antimicrobial barrier can support wound healing while simultaneously reducing bacterial bioburden.46,52,53 In addition, the average area reduction for all wounds attained by week 4 (59.7%) gives strong likelihood to achieve CWC.54,55 However, it should be noted that 1 wound achieved less area reduction than the other wounds (5%) by week 4. Taken together, PCMP paired with SOC may be a viable method to support wound healing by reducing bacterial bioburden and helping to transition wounds out of chronicity.
Bacterial bioburden in the periwound region has been associated with delayed wound healing.31 Results from this study indicated that 80% of wounds had a FL+ periwound region at week 2 which was absent by week 4. This finding agrees with previous evidence suggesting that bacterial bioburden in the periwound region has been reported in ≥80% of wounds.31,39,56 Considering the prevalence and risk associated with its periwound presence, this finding highlights the importance of a real-time, high-accuracy method of bacterial bioburden detection. The use of fluorescence imaging allows for targeted debridement to enhance bacterial removal. This may not be attainable with SOC debridement that is visual based. In fact, some evidence suggests that up to 100% of wounds that received SOC debridement were FL+ afterwards.39,57,58 Thus, the ability to rapidly identify FL+ in the periwound region allowed for accurate debridement of our study wounds and may have contributed to the large mean area reductions.
It is interesting to note that unhealed wounds at week 6 were FL- yet bacterial loads of ≥104 CFU (5.1 x 105 ± 3.5 x 105 CFU) were detected. While it would seem counterintuitive that a wound would be FL-, despite a bacterial load ≥104 CFU, the NGS used to analyze the tissue swabs is extremely sensitive. This means that an NGS CFU incorporates bacteria of all genotypes and bacteria that are alive or dead.59 Therefore, it is possible that, while bacteria were still detected, other porphyrin/pyoverdine-producing bacteria contained within PCMP were reduced and a FL- was produced. In addition, variance in technique while collecting the tissue swab could have resulted in higher bacterial loads. For example, greater pressure applied while sampling or more twists of the swab could result in a larger bacterial concentration.60 Both potential explanations may be illustrated by 1 study wound that saw an increase in bacterial load from week 1 to week 6 despite achieving FL- (week 1: 9.8 x 103 CFU, FL+ vs. week 6: 7.4 x 105 CFU, FL-). Of most importance, this finding supports the ability of PCMP as an antimicrobial barrier to manage bacterial bioburden that can contribute to wound chronicity and supports the efficacy of fluorescence imaging in its detection during targeted debridement. Selective use of quantitative and semiquantitative methods to determine bacterial bioburden may prove useful as an adjunct to PCMP wound management in the future. Larger comparative studies appear to be warranted based on promising results demonstrated in this observational case series.
Limitations
Limitations were present in our study that should be noted. To begin, the small sample size of our pilot study makes it difficult to draw definitive conclusions about the effects of our methods of wound management. In addition, the short duration of our trial may have not allowed for observation of wounds that ultimately achieved CWC. Image review in our trial was not blinded, making it impossible to rule out measurement bias. Tissue swabs and NGS were only conducted at week 1 and 6. While all wounds achieved FL-, we were unable to corroborate our fluorescence imaging findings with NGS from weeks 2 to 5. As a diagnostic tool, fluorescence imaging has multiple limitations including inabilities to detect bacteria >1.5 mm from the wound surface and to identify bacterial genotypes. It should also be noted that FL+ is not a guarantee of the presence of infection. Therefore, fluorescence imaging should be viewed as an enhancement to SOC wound assessment and NGS as opposed to a replacement.
Conclusion
The present study demonstrated that use of a real-time method of bacterial detection and PCMP, as an antimicrobial barrier, may be beneficial in managing the wound healing environment. Real-time detection of bacteria by fluorescence imaging allows for targeted debridement and higher probability of bacterial removal. In turn, this may enhance the ability of PCMP to manage bacterial bioburden, prevent reformation of biofilm, and support an ideal environment for wound healing. As was demonstrated in our results, a combination of these modalities led to either CWC or high probability of future CWC in just 6 weeks. Therefore, use of this method of wound management may provide clinicians with an opportunity to shorten treatment time and cost to the patient while improving treatment outcomes. Implementing NGS as a diagnostic testing tool could provide a more comprehensive picture of all pathogens involved in the biofilm formation, and thus guide the selection of appropriate therapy and improve treatment outcome. Future studies should look to incorporate larger sample sizes and greater durations of observation to affirm the positive findings of our study.
References
1. Enoch S, Price P. Cellular, molecular and biochemical differences in the pathophysiology of healing between acute wounds, chronic wounds and wounds in the aged. World Wide Wounds. 2004;13:1–17.
2. Lanau-Roig A, Fabrellas N, Sáez-Rubio G, Wilson K. Time of Chronic wound healing, as part of a prevalence and incidence study. Enfermería Global. 2017;16(2):445-453.
3. Guo S, Dipietro LA. Factors affecting wound healing. J Dent Res. 2010;89(3):219-229. doi:10.1177/0022034509359125
4. Edwards R, Harding KG. Bacteria and wound healing. Curr Opin Infect Dis. 2004;17(2):91-96. doi:10.1097/00001432-200404000-00004
5. Darvishi S, Tavakoli S, Kharaziha M, Girault HH, Kaminski CF, Mela I. Advances in the Sensing and Treatment of Wound Biofilms. Angew Chem Int Ed Engl. 2022;61(13):e202112218. doi:10.1002/anie.202112218
6. Gardner SE, Hillis SL, Frantz RA. Clinical signs of infection in diabetic foot ulcers with high microbial load. Biol Res Nurs. 2009;11(2):119-128. doi:10.1177/1099800408326169
7. Percival SL, Thomas JG, Williams DW. Biofilms and bacterial imbalances in chronic wounds: anti-Koch. Int Wound J. 2010;7(3):169-175. doi:10.1111/j.1742-481X.2010.00668.x
8. Withycombe, C., Purdy, K.J. and Maddocks, S.E. (2017), Micro-management: curbing chronic wound infection. Mol oral Microbiol, 32: 263-274. https://doi.org/10.1111/omi.12174
9. Xu L, McLennan SV, Lo L, et al. Bacterial load predicts healing rate in neuropathic diabetic foot ulcers. Diabetes Care. 2007;30(2):378-380. doi:10.2337/dc06-1383
10. Bowler PG. The 10(5) bacterial growth guideline: reassessing its clinical relevance in wound healing. Ostomy Wound Manage. 2003;49(1):44-53.
11. Halim AS, Khoo TL, Saad AZ. Wound bed preparation from a clinical perspective. Indian J Plast Surg. 2012;45(2):193-202. doi:10.4103/0970-0358.101277
12. Malone M, Bjarnsholt T, McBain AJ, et al. The prevalence of biofilms in chronic wounds: a systematic review and meta-analysis of published data. J Wound Care. 2017;26(1):20-25. doi:10.12968/jowc.2017.26.1.20
13. Attinger C, Wolcott R. Clinically Addressing Biofilm in Chronic Wounds. Adv Wound Care (New Rochelle). 2012;1(3):127-132. doi:10.1089/wound.2011.0333
14. Metcalf DG, Bowler PG. Biofilm delays wound healing: A review of the evidence. Burns Trauma. 2013;1(1):5-12. Published 2013 Jun 18. doi:10.4103/2321-3868.113329
15. Rajpaul K. Biofilm in wound care. Br J Community Nurs. 2015;Suppl Wound Care:S6-S11. doi:10.12968/bjcn.2015.20.Sup3.S6
16. Phillips PL WR, Fletcher J, Schultz GS. Biofilms made easy. Wounds International. 2010;1(3):1-6.
17. Bjarnsholt T, Kirketerp-Møller K, Jensen PØ, et al. Why chronic wounds will not heal: a novel hypothesis. Wound Repair Regen. 2008;16(1):2-10. doi:10.1111/j.1524-475X.2007.00283.x
18. Percival SL, McCarty SM, Lipsky B. Biofilms and Wounds: An Overview of the Evidence. Adv Wound Care (New Rochelle). 2015;4(7):373-381. doi:10.1089/wound.2014.0557
19. Wolcott RD, Rumbaugh KP, James G, et al. Biofilm maturity studies indicate sharp debridement opens a time- dependent therapeutic window. J Wound Care. 2010;19(8):320-328. doi:10.12968/jowc.2010.19.8.77709
20. Thaarup IC, Bjarnsholt T. Current In Vitro Biofilm-Infected Chronic Wound Models for Developing New Treatment Possibilities. Adv Wound Care (New Rochelle). 2021;10(2):91-102. doi:10.1089/wound.2020.1176
21. Choi Y, Oda E, Waldman O, Sajda T, Beck C, Oh I. Next-generation sequencing for pathogen identification in infected foot ulcers. Foot Ankle Orthop. 2021;6(3):24730114211026933. Published 2021 Jul 12. doi:10.1177/24730114211026933
22. Nussbaum SR, Carter MJ, Fife CE, et al. An Economic Evaluation of the Impact, Cost, and Medicare Policy Implications of Chronic Nonhealing Wounds. Value Health. 2018;21(1):27-32. doi:10.1016/j.jval.2017.07.007
23. Wolcott RD, Rhoads DD, Bennett ME, et al. Chronic wounds and the medical biofilm paradigm. J Wound Care. 2010;19(2):45-53. doi:10.12968/jowc.2010.19.2.46966.
24. Mao C, Zhu W, Xiang Y, et al. Enhanced near-infrared photocatalytic eradication of MRSA biofilms and osseointegration using oxide perovskite-based P-N heterojunction. Adv Sci (Weinh). 2021;8(15):e2002211. doi:10.1002/advs.202002211
25. Clinton A, Carter T. Chronic Wound Biofilms: Pathogenesis and Potential Therapies. Lab Med. 2015;46(4):277-284. doi:10.1309/LMBNSWKUI4JPN7SO
26. Zhao G, Hochwalt PC, Usui ML, et al. Delayed wound healing in diabetic (db/db) mice with Pseudomonas aeruginosa biofilm challenge: a model for the study of chronic wounds. Wound Repair Regen. 2010;18(5):467-477. doi:10.1111/j.1524-475X.2010.00608.x
27. Zhao G, Usui ML, Underwood RA, et al. Time course study of delayed wound healing in a biofilm-challenged diabetic mouse model. Wound Repair Regen. 2012;20(3):342-352. doi:10.1111/j.1524-475X.2012.00793.x
28. Wolcott R. Economic aspects of biofilm-based wound care in diabetic foot ulcers. J Wound Care. 2015;24(5):189-194. doi:10.12968/jowc.2015.24.5.189
29. Paoli CJ, Reynolds MA, Sinha M, Gitlin M, Crouser E. Epidemiology and costs of sepsis in the United States-An analysis based on timing of diagnosis and severity level. Crit Care Med. 2018;46(12):1889-1897. doi:10.1097/CCM.0000000000003342
30. Hicks CW, Selvarajah S, Mathioudakis N, et al. Trends and determinants of costs associated with the inpatient care of diabetic foot ulcers. J Vasc Surg. 2014;60(5):1247-1254.e2. doi:10.1016/j.jvs.2014.05.009
31. Cole W, Coe S. Use of a bacterial fluorescence imaging system to target wound debridement and accelerate healing: a pilot study. J Wound Care. 2020;29(Sup7):S44-S52. doi:10.12968/jowc.2020.29.Sup7.S44
32. Bianchi T, Wolcott RD, Peghetti A, et al. Recommendations for the management of biofilm: a consensus document. J Wound Care. 2016;25(6):305-317. doi:10.12968/jowc.2016.25.6.305
33. Schultz G, Bjarnsholt T, James GA, et al. Consensus guidelines for the identification and treatment of biofilms in chronic nonhealing wounds. Wound Repair Regen. 2017;25(5):744-757. doi:10.1111/wrr.12590
34. Moelleken M, Jockenhöfer F, Benson S, Dissemond J. Prospective clinical study on the efficacy of bacterial removal with mechanical debridement in and around chronic leg ulcers assessed with fluorescence imaging. Int Wound J. 2020;17(4):1011-1018. doi:10.1111/iwj.13345
35. Carpenter S, Davis S, Fitzgerald R, et al. Expert recommendations for optimizing outcomes in the management of biofilm to promote healing of chronic wounds. Wounds. 2016;28:S1–S20.
36. Bowler P, Murphy C, Wolcott R. Biofilm exacerbates antibiotic resistance: Is this a current oversight in antimicrobial stewardship?. Antimicrob Resist Infect Control. 2020;9(1):162. Published 2020 Oct 20. doi:10.1186/s13756-020-00830-6
37. Lewis, K. Platforms for antibiotic discovery. Nat Rev Drug Discov 12, 371–387 (2013). https://doi.org/10.1038/nrd3975
38. Rennie MY, Lindvere-Teene L, Tapang K, Linden R. Point-of-care fluorescence imaging predicts the presence of pathogenic bacteria in wounds: a clinical study. J Wound Care. 2017;26(8):452-460. doi:10.12968/jowc.2017.26.8.452
39. Raizman R. Fluorescence imaging guided dressing change frequency during negative pressure wound therapy: a case series. J Wound Care. 2019;28(Sup9):S28-S37. doi:10.12968/jowc.2019.28.Sup9.S28
40. Rennie MY, Dunham D, Lindvere-Teene L, Raizman R, Hill R, Linden R. Understanding Real-Time Fluorescence Signals from Bacteria and Wound Tissues Observed with the MolecuLight i:XTM. Diagnostics (Basel). 2019;9(1):22. Published 2019 Feb 26. doi:10.3390/diagnostics9010022
41. Serena TE, Harrell K, Serena L, Yaakov RA. Real-time bacterial fluorescence imaging accurately identifies wounds with moderate-to-heavy bacterial burden. J Wound Care. 2019;28(6):346-357. doi:10.12968/jowc.2019.28.6.346
42. Jones LM, Dunham D, Rennie MY, et al. In vitro detection of porphyrin-producing wound bacteria with real-time fluorescence imaging. Future Microbiol. 2020;15:319-332. doi:10.2217/fmb-2019-0279
43. Hurley CM, McClusky P, Sugrue RM, Clover JA, Kelly JE. Efficacy of a bacterial fluorescence imaging device in an outpatient wound care clinic: a pilot study. J Wound Care. 2019;28(7):438-443. doi:10.12968/jowc.2019.28.7.438
44. Gilbert P, Moore LE. Cationic antiseptics: diversity of action under a common epithet. J Appl Microbiol. 2005;99(4):703-715. doi:10.1111/j.1365-2672.2005.02664.x
45. Müller G, Kramer A, Schmitt J et al.. Reduced cytotoxicity of polyhexamethylene biguanide hydrochloride (PHMB) by egg phosphatidylcholine while maintaining antimicrobial efficacy. Chem Biol Interact 2011; 190(2-3):171–178. https://doi.org/10.1016/j.cbi.2011.02.024
46. Davis SC, Gil J, Solis M, et al. Antimicrobial effectiveness of wound matrices containing native extracellular matrix with polyhexamethylene biguanide. Int Wound J. 2022;19(1):86-99. doi:10.1111/iwj.13600
47. Hübner NO, Kramer A. Review on the efficacy, safety and clinical applications of polihexanide, a modern wound antiseptic. Skin Pharmacol Physiol. 2010;23 Suppl:17-27. doi:10.1159/000318264
48. Gilliver S. PHMB: a well-tolerated antiseptic with no reported toxic effects. J Wound Care. 2009; Suppl:9-14.
49. MolecuLight. How to use the MolecuLight i: X (e-Learning Modules). Published 2018. Accessed April 16, 2023. https://moleculight.com/training-resources/
50. MolecuLight. i:XTM User Manual MolecuLight Inc. Published 2018. Accessed April 16, 2023. https://moleculight.com/wp-content/uploads/2018/05/PN_1294_MolecuLight_iX_User_Manual_Rev_1.0_English.pdf
51. Tang S, Prem A, Tjokrosurjo J, et al. The canine skin and ear microbiome: A comprehensive survey of pathogens implicated in canine skin and ear infections using a novel next-generation-sequencing-based assay. Vet Microbiol. 2020;247:108764. doi:10.1016/j.vetmic.2020.108764
52. Oropallo AR. Use of Native Type I Collagen Matrix Plus Polyhexamethylene Biguanide for Chronic Wound Treatment. Plast Reconstr Surg Glob Open. 2019;7(1):e2047. Published 2019 Jan 15. doi:10.1097/GOX.0000000000002047
53. Bain MA, Koullias GJ, Morse K, Wendling S, Sabolinski ML. Type I collagen matrix plus polyhexamethylene biguanide antimicrobial for the treatment of cutaneous wounds. J Comp Eff Res. 2020;9(10):691-703. doi:10.2217/cer-2020-0058
54. Sheehan P, Jones P, Caselli A, Giurini JM, Veves A. Percent change in wound area of diabetic foot ulcers over a 4-week period is a robust predictor of complete healing in a 12-week prospective trial. Diabetes Care. 2003;26(6):1879-1882. doi:10.2337/diacare.26.6.1879
55. Gelfand JM, Hoffstad O, Margolis DJ. Surrogate endpoints for the treatment of venous leg ulcers. J Invest Dermatol. 2002;119(6):1420-1425. doi:10.1046/j.1523-1747.2002.19629.x
56. Farhan N, Jeffery S. Utility of MolecuLight i:X for Managing Bacterial Burden in Pediatric Burns. J Burn Care Res. 2020;41(2):328-338. doi:10.1093/jbcr/irz167
57. Kim PJ, Attinger CE, Bigham T, et al. Clinic-based Debridement of Chronic Ulcers Has Minimal Impact on Bacteria. Wounds. 2018;30(5):114-119.
58. Schwartz JA, Goss SG, Facchin F, Avdagic E, Lantis JC. Surgical debridement alone does not adequately reduce planktonic bioburden in chronic lower extremity wounds. J Wound Care. 2014;23(9):. doi:10.12968/jowc.2014.23.Sup9.S4
59. Boers SA, Jansen R, Hays JP. Understanding and overcoming the pitfalls and biases of next-generation sequencing (NGS) methods for use in the routine clinical microbiological diagnostic laboratory. Eur J Clin Microbiol Infect Dis. 2019;38(6):1059-1070. doi:10.1007/s10096-019-03520-3
60. Griffith C. Surface Sampling and the Detection of Contamination. Handbook of Hygiene Control in the Food Industry. 2016;673-696. doi:10.1016/B978-0-08-100155-4.00044-3
