



Observational Study of Venous Leg Ulcer Treated With a Native Collagen-Alginate Dressing and the Impact on Wound-Related Quality of Life
Abstract
BACKGROUND: Venous leg ulcers (VLUs) are associated with various physical and social adverse effects for patients but also contribute to a significant socioeconomic burden. PURPOSE: To examine the clinical performance and safety of a collagen-alginate dressing in combination with standard wound care in non-healing VLUs. METHODS: In an observational, explorative, single-center study, VLUs of 60 patients were covered with a collagen-alginate dressing. Wounds were assessed during 5 visits over a 4-week period. At the final visit, health care professionals gave an overall assessment of the dressing. Outcome parameters were wound area reduction, wound pain, wound-related quality of life (QoL), and incidence of adverse events. RESULTS: The mean wound area decreased (17.8 ± 11.2 cm² versus 11.4 ± 9.0 cm²; P < .0001), and 4 patients achieved complete closure. Wound pain decreased after 2 weeks, and intake of analgesics reduced. Patients’ wound-related QoL improved and a correlation between the well-being sub-score and wound area reduction was found. All health care professionals rated the collagen-alginate dressing as ‘very good’ or ‘good.’ CONCLUSION: The collagen-alginate dressing is safe and effective in promoting healing and addressing the pain of VLUs. It also improves patients’ QoL, possibly by reducing wound area, pain, and exudate.
Introduction
Venous leg ulcers (VLUs) are the most common type of ulcers in the lower extremities, accounting for 70% to 80% of ulcers seen by health care professionals.1 This type of ulcer has a prevalence of up to 2% of the population, rising to 5% in individuals over the age of 65.1 Several risk factors contribute to the development of VLUs, including advanced age, obesity, low physical activity, arterial hypertension, deep vein reflux, deep venous thrombosis, and family history of VLUs.2 The exact physiological process leading to VLUs is not yet fully understood,3-5 but they are known to be caused by sustained venous hypertension due to chronic venous insufficiency.6-8 VLUs pose a significant socioeconomic burden due to their frequency, chronicity, and associated costs.9 The estimated annual costs for managing VLUs were approximately US$3.5 billion in the United States,10 US$802.55 million in Australia,11 and £102 million in the United Kingdom.12
VLUs are considered complex chronic wounds due to extensive loss of skin integrity, compromised tissue viability, association with systemic pathologies that hinder healing, and susceptibility to infection.4 While acute, simple wounds typically heal within 4 weeks,1 complex chronic wounds such as VLUs defy conventional treatment measures and fail to restore normal anatomical and functional integrity within 3 months.13 On average, VLUs require 6 to 12 months to heal, but with proper wound care and compression to counteract venous hypertension, healing rates of 76% at 4 months can be achieved.1 However, VLUs often recur, with recurrence rates of up to 50% at 3 months5 and 70% within 5 years of closure.1 Hence, many VLUs can be considered hard-to-heal wounds.14
The sustained healing of VLUs therefore presents a major challenge and considerably impacts patients’ health and quality of life (QoL).15 VLUs are associated with various physical and social adverse effects, including pain, limitations in work and leisure activities, impaired mobility, sleep disturbance, reduced psychological wellbeing, and social isolation.7 Studies have shown that VLUs particularly affect the emotional aspect of patients’ health-related QoL.16,17 Moreover, there are associations between wound status and QoL decline17 as well as between ulcer-related pain and reduced QoL.16 Approximately 80% of patients with VLU experience mild-to-moderate pain,18 which is the most prevalent symptom in these patients.19 Pain not only affects wound healing via an emotional-physiological link but also has a profound impact on physical, psychological, and social wellbeing, ultimately reducing QoL.19
The Society for Vascular Surgery and the American Venous Forum recommend primary dressings that manage wound exudate and maintain a moist wound bed in conjunction with multicomponent compression bandaging as standard care for managing VLUs,20 provided there are no arterial complications.15 The ankle-brachial pressure index (ABPI) is used to assess arterial disease and guide treatment decisions.15 Primary wound contact dressings are used beneath compression devices to promote healing, provide comfort, control exudate, and prevent adherence of compression garments to the wound bed.21 Various dressing types including alginate, foam, hydrocolloid, hydrofiber, or hydrogel are available.22 Promising results with respect to safety and wound healing in non-healing VLUs have been achieved with a combination of a collagen dressing and an alginate pad in conjunction with compression therapy.23
This observational, explorative study was conducted to examine the clinical performance and safety of a native collagen-alginate dressing in combination with standard wound care on wound area reduction, pain management, and wound-related QoL in non-healing VLUs.
Methods
The observational, explorative, single-center study was performed between August 2020 and July 2022 at the Northwell Health System Comprehensive Wound Care Healing Center and Hyperbarics, New York, U.S. The study was carried out in compliance with the US Federal Food, Drug, and Cosmetics Act and in accordance with the ethical principles of the Declaration of Helsinki. The study plan was verified by BRANY IRB (Lake Success, NY). The aim of the study was to investigate the effectiveness and safety of a native bovine collagen-alginate dressing for the treatment of non-healing VLUs in conjunction with standard care practices. Standard care practices included debridement of stalled wounds prior to further local wound care as well as treatment-accompanied compression therapy.
Patients suffering from VLUs and who conformed to the inclusion and exclusion criteria (Table 1) were recruited. Informed consent was obtained from all participants. Following study assessment and baseline documentation, patients’ wounds were covered with a collagen-alginate dressing (Cutimed® Epiona®, BSN medical GmbH, Essity Group, Hamburg, Germany) of appropriate size, a secondary dressing, and compression. Compression had been applied in 49 (98.0%) patients in the form of wraps, stockings, or bandages of various compression classes (I – III, 18 – 46 mmHg) for durations ranging from < 6 weeks to > 6 months before study onset depending on disease severity and patient preference. Compression was not reported for 1 patient. At the time of study initiation, bandages were used in 11 (19.0%), stockings in 6 (10.3%), wraps in 39 (67.2%), and other compression in 2 (3.4%) patients. Eight patients received 2 of the aforementioned types of compression. Class I compression was used in 11 (19.0%), class II in 6 (10.3%), and class III in 41 (70.7%) patients. Compression therapy was not modified during the study. The following secondary dressings were used: gauze, conforming bandages, abdominal pad, foam superabsorber, hydrofiber, and alginate. Within a 4-week study period, wounds were assessed during 5 visits: Visit (V) 1 at Day 0 / baseline, V2 at Day 7 ± 1 day, V3 at Day 14 ± 2 days, V4 at Day 21 ± 3 days, and V5 at Day 28 ± 3 days. Application of the dressing as well as dressing changes were performed at the discretion of the health care professional, typically every 3 to 5 days, following the instructions provided. Patients were given enough products for intermediate dressing changes. All patients were treated with the collagen-alginate dressing for 4 weeks / 5 visits, or until complete wound healing was achieved. After 28 ± 3 days, dressings were removed for final documentation of the wound, and the health care professional gave an overall assessment of the collagen-alginate dressing.
The primary outcome parameter was wound area reduction. Secondary outcome parameters included patient-reported wound pain and wound-related QoL as well as incidence of adverse events. Wound pain was evaluated during each visit using a visual analogue scale (VAS) ranging from 0 (no pain) to 10 (maximum pain). Wound-related QoL was investigated at baseline and V5 or the visit at which complete wound healing prior to study end was achieved, respectively. Patients filled in a validated wound-QoL questionnaire, the Wound-QoL-17, consisting of 17 items as described elsewhere.9 Items were grouped in 3 categories, namely “body score,” “wellbeing score” and “everyday life score,” resulting in a total score and 3 sub-scores. Lower values indicated higher QoL.
All enrolled subjects were allocated to the intention-to-treat (ITT) population. Analyses were then conducted using a per-protocol (PP) population approach. Descriptive and inferential statistics of baseline data and outcome parameters were performed using standard statistical measures (absolute and relative frequencies for categorial data, mean, and standard deviation). P < .001 was considered statistically significant for inferential statistical tests, including analysis of variance and t-test.
Results
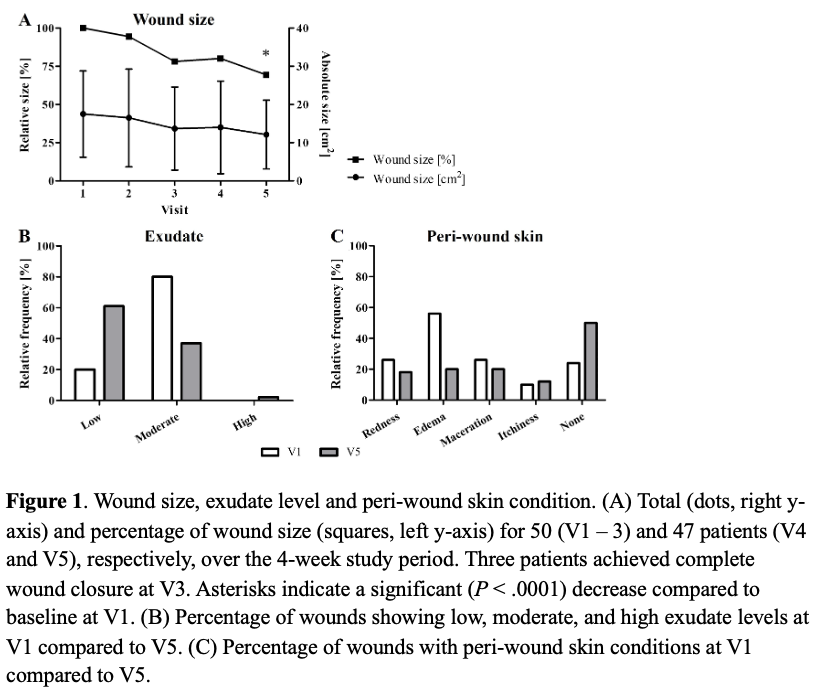
A total of 60 patients were initially recruited (ITT population) and 50 patients (58% male) completed the study according to the protocol (PP population). Ten patients were lost to follow-up, had unsuccessful screening, and were no longer within the inclusion criteria. Of the PP population, 47 patients completed V1 through V5, with 1 patient achieving complete wound healing at V5. Three participants achieved complete wound healing at V3.
Assessed ulcers were located on the leg in 49 patients and on the leg and foot in 1 patient. Wound duration ranged from 1.5 to 24 months (Figure 1). Patients were 68.7 ± 14.6 years old on average and had a mean ABPI of 1.1 ± 0.1. Baseline data of participants’ demographics are presented in Table 2. All patients (100%) reported comorbidities, with hypertension being the most common (70%). Patients also reported chronic venous hypertension (26%), venous insufficiency (20%), diabetes (20%), deep vein thrombosis (18%), morbid obesity (16%), and varicose veins (10%).
Wound size
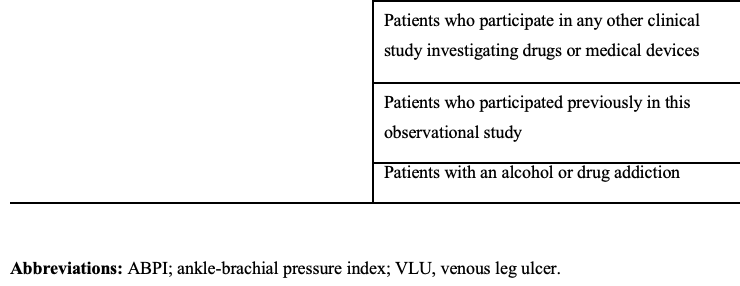
The average wound area at V1 measured 17.8 ± 11.2 cm² and significantly decreased to 11.4 ± 9.0 cm² at V5 (Figure 1A) (N = 48; P < .0001). Similarly, the relative wound area reduction of 32.2 ± 42.7% (min: -120.8 %, max: 100.0 %) between V1 and V5 was significant (N = 48; P < .0001). During the study period, 4 individuals successfully achieved wound closure, characterized by 100% epithelial or scar tissue formation. Among these patients, 3 reached this milestone at V3, while 1 patient accomplished it at V5. Wound healing did not depend on wound duration, as it was comparable for wounds of all 3 included duration categories (Table 2). In line with decreased wound size, percentage of wounds with moderate amount of exudate decreased from 80% to 37% during the study period (Figure 1B). More precisely, a decrease of exudate was observed in 24 patients (48%), an increase was seen in 2 patients (4%), and no change was documented in the remaining 24 patients (48%). Treatment with the collagen-alginate dressing protected and improved the peri-wound skin. Accordingly, redness, edema, and maceration decreased between V1 and V5, whereas the proportion of patients unaffected by periwound skin conditions increased (Figure 1C). Itchiness was only reported for 1 more patient at V5 compared to V1.
Wound pain
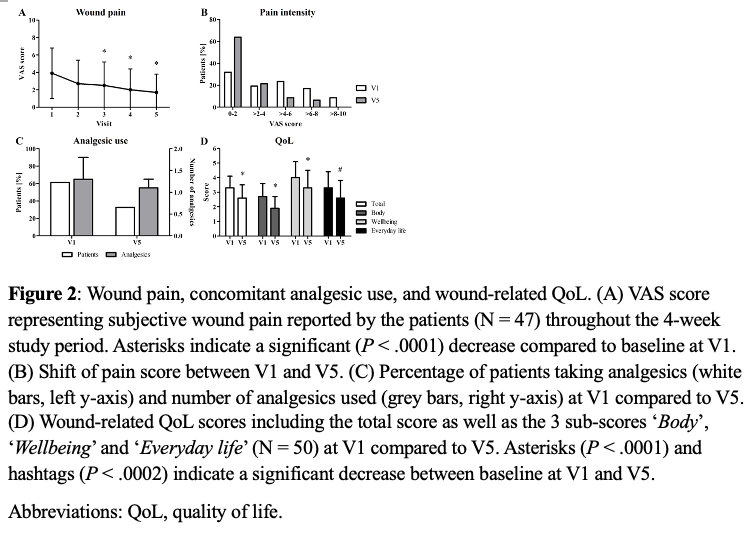
Wound pain was assessed using a VAS ranging from 0 (no pain) to 10 (maximum pain). Before treatment with the collagen-alginate dressing, patients evaluated their pain with a mean score of 3.9 ± 2.9 (N = 50) which significantly decreased to 2.5 ± 2.7 at V3 (N = 50; P = .0004), 2.0 ± 2.4 at V4 (N = 47; P < .0001), and 1.7 ± 2.1 at V5 (N = 47; P < .0001) (Figure 2A). Treatment with the collagen-alginate dressing also alleviated severe pain, as shown by a reduced number of scores > 4 at V5 compared to V1 and no score > 8 (Figure 2B). Consequently, the number of patients experiencing no pain (0 on the VAS) steadily increased from 7 patients (14.9%) at V1 to 23 patients (48.9%) at V5. In addition, at V1 a mean of 1.3 analgesics were taken by 61.2% of patients, whereas only 32.7% of patients required a mean of 1.1 analgesics at V5, indicating that the use of additional analgesics was discontinued in 46.6% of patients previously requiring painkillers (Figure 2C). Wound pain was not correlated with wound area. In accordance with decreased general wound pain, pain during dressing changes also decreased from a mean VAS score of 0.3 ± 1.5 at V1 to 0 at all other visits. Of note, local topical anesthetics were applied in 34 of the 50 patients as part of standard care before wound debridement during visits, if necessary.
Quality of life
Patients’ wound-related QoL was assessed at V1 and at the final visit using the Wound-QoL-17 questionnaire. While wound-related QoL did not improve for every patient, overall total and sub-scores showed a significant decrease at the final visit compared to V1 (N = 50; P < .0001 for total, body, and wellbeing score, P = .0002 for everyday life score) (Figure 2D). Wound-related QoL deteriorated for 9 patients (18%), as indicated by an increased score. Sub-scores were further analyzed to identify potential correlations to different wound parameters. A statistically significant correlation (P = .0002) was found for the relative wellbeing score reduction and the relative wound area reduction. No other correlations were identified.
Dressing evaluation
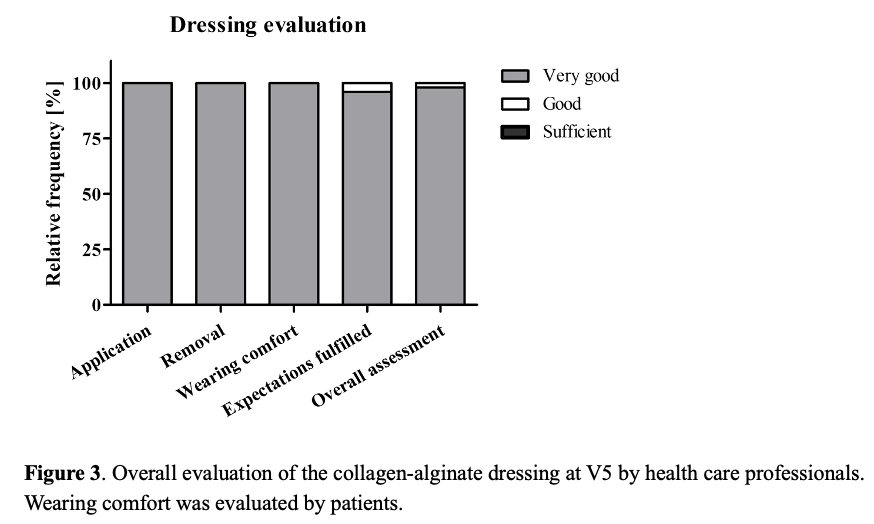
Participating health care professionals were asked to give an overall evaluation of the collagen-alginate dressing at V5. Application and removal of the dressing as well as its adaptation to the affected area were rated ”very good” for all 50 treatments (Figure 3). The fulfillment of health care professionals’ expectations was rated as “very good” in 96% and “good” in 4% of cases. The overall assessment of the collagen-alginate dressing was “very good” for 98% of the treatments and “good” for 2 % (Figure 3). The dressing’s performance compared to previous treatment products was rated “better” in 92% and “the same” in 8% of cases. Wearing comfort was rated “very good” by all 50 patients.
Overall, treatment of VLUs using the collagen-alginate dressing significantly decreased wound size, even in previously persisting wounds. The dressing led to the protection and improvement of periwound skin as indicated by an overall decrease in the number of patients reporting periwound skin conditions. Treatment with the alginate dressing significantly decreased general wound pain while significantly improving wound-related QoL.
Safety
During the complete study period, 8 adverse events were reported, 2 of which occurred in patients in the PP population. Adverse events included pain, wound infection, increased slough, and fungal dermatitis. All reported events were categorized as moderate. An association with the collagen-alginate dressing was considered unlikely in all 8 adverse events. No serious adverse events were documented.
Case reports
Two representative cases are described here in more detail as examples of the main findings of this study.
Case 1
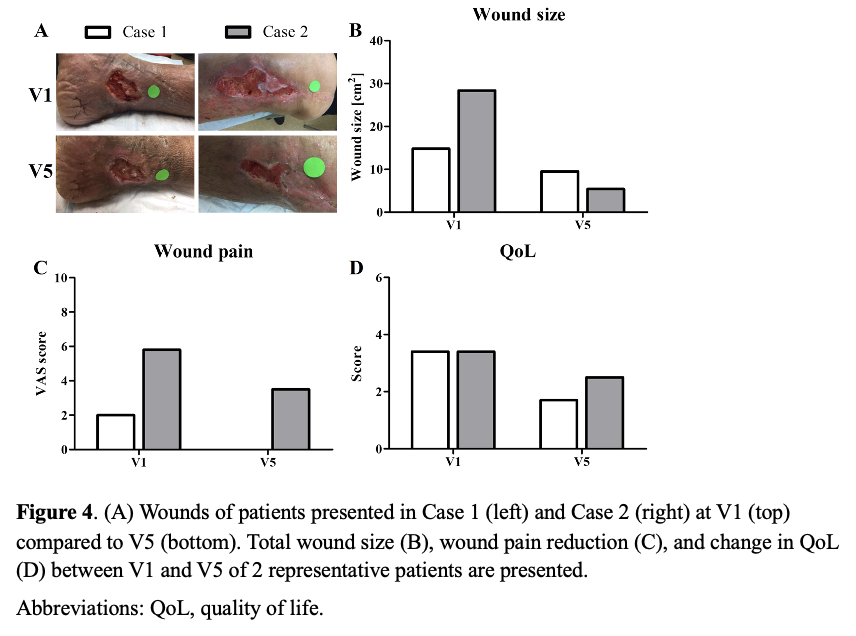
A 64-year-old male with a history of hypertension, chronic venous insufficiency, and lymphedema presented with a stalled, complex VLU he had suffered from for 24 months. The wound area measured 14.8 cm2 at V1 and decreased by 35.8% to 9.5 cm2 at V5 (Figure 4A; Figure 4B). The patient reported a reduction of wound pain by 100% within the study duration (Figure 4C). The total wound-related QoL score decreased by 50% from V1 to V5 (Figure 4D), representing an improved wound-related QoL.
Case 2
A 57-year-old female with obesity and a history of hypertension and chronic venous insufficiency had suffered from a VLU for 3 months. The wound had been treated with various medications as well as compression therapy, but healing had stalled. Initially, the wound measured 28.4 cm2. At V5, following 4 weeks of treatment using the collagen-alginate dressing, the wound area was reduced by 81% to 5.4 cm2 (Figure 4A; Figure 4B). Wound pain levels as documented by the patient decreased by 39.7% from V1 to V5 (Figure 4C). The total wound-related QoL score improved by 26.5% within the 4-week study period (Figure 4D).
Discussion
Chronic wounds such as VLUs considerably impact patients’ lives, and patients can exhibit increased rates of depression10 and a substantial loss of QoL.4,19,24 Numerous factors affect QoL in VLU patients, including physical, psychosocial, and treatment aspects. The main physical consideration is wound pain, while other physical factors impacting VLU patients include exudate, wound odor, limited mobility, and sleep disturbances. Psychosocial parameters include social isolation, depression, loss of power, and helplessness. Efficacy of treatment, improvement of the wound, and time required for healing make up the treatment-related aspects. Both psychosocial and treatment aspects are mainly affected by the chronic nature of VLUs.24 However, the most significant and consistent symptom of VLU is pain,4,19,24 which is the main contributor to poor QoL.24-27 Pain is often inadequately addressed,24,28 as the patients’ subjective discomfort is often considered secondary to the primary, objective clinical aspects of wound care and healing.25 Several previous studies have showed that pain can impair wound healing through psycho-neuro-immunological connections,29 suggesting a positive correlation between improved pain and VLU healing.28 Hence, wound status and characteristics, pain, and treatment efficacy all interact to ultimately affect QoL.
In addition to the social, personal, financial, and psychological impact on the individual patient,30 VLUs also inflict a high socioeconomic burden on health care systems due to the cost and prolonged duration of care.31 Indirect costs arise from the loss of productivity of both patients and family members who offer home care but also from premature disability and various other contributing factors.31 Therefore, promoting wound healing of VLUs not only reduces pain but also considerably increases patients’ QoL and lowers socioeconomic costs.32 Consequently, there is a high need for management strategies that improve healing without increasing overall costs.
Generally, compression therapy has long been considered the mainstay for management of VLUs.32 However, choosing the right dressing to use under compression is crucial in order to maintain an optimal, moist wound healing environment and protect the wound and periwound skin.21,32 Numerous dressing options—such as alginate, foam, hydrocolloid, hydrofiber, or hydrogel—are available.22 A substantial part of the extracellular matrix is made up of collagen, indicating the potential benefits of collagen-based wound dressings in the wound healing process.33 Collagen and collagen-derived fragments regulate numerous cellular functions to drive the process of tissue function, growth, and repair, making collagen a key component of wound healing. The function of collagen in wound healing has been reviewed elsewhere.34,35
This observational, explorative study was carried out to investigate the clinical efficacy and safety of a native collagen-alginate dressing in conjunction with standard wound care in non-healing VLUs. In addition to wound area reduction, this study particularly focused on the impact of the dressing on pain and wound-related QoL. To assess QoL, the Wound-QoL-17 questionnaire was used. It has been validated as a simple tool with good internal consistency for the longitudinal evaluation of QoL in patients with chronic wounds.9 Non-healing VLUs that had previously unsuccessfully been treated with debridement, further local wound care, and compression therapy were additionally treated with a native collagen-alginate dressing under compression for 4 weeks. Within the study period, mean wound area significantly decreased and 4 patients achieved complete wound closure. In addition, the overall total and sub-scores of wound-related QoL significantly improved and a significant correlation between the QoL wellbeing sub-score and reduced wound area was found after treatment with the native collagen-alginate dressing.
Collagen-based wound dressings have been shown to have positive effects on wound healing in vitro and in vivo. They significantly boost fibroblast production, attract fibroblasts to enhance the deposition of organized collagen fibers, and facilitate directed cell migration. Their hydrophilic properties support fibroblast permeation and the uptake of fibronectin while preserving leukocytes, macrophages, fibroblasts, and epithelial cells. They also help maintain the wound’s chemical and thermostatic microenvironment. Additionally, these dressings inhibit or deactivate excess matrix metalloproteinases, which are key contributors to wound chronicity.36 However, data concerning the effect of collagen-alginate dressings in conjunction with compression therapy on wound-related QoL are scarce. Collagen-based wound dressings employ various forms of carriers including gels, pastes, or cellulose. The collagen may be derived from bovine, porcine, or other animal sources, and be native or denatured. While there may be differences in the exact effects of the various collagen-based wound dressings, the general mode of action is similar.36 Hence, studies investigating other collagen-based products for wound management can be compared to the native collagen-alginate dressing investigated in the present study. For example, the effect of collagen from fish skin on healing, pain intensity, and QoL in patients with VLUs was investigated in a randomized, controlled trial.37 Patients received standard treatment including class 2 compression therapy (40 mmHg) and wound hygiene procedures in addition to either a collagen gel or placebo gel for 12 weeks. Healing progress, pain reduction, and improvement in QoL were observed in all patients. The same standard of care, including compression therapy and wound bed care, was received by both groups. However, better results in both the healing process, as indicated by wound area reduction, and improvement of health-related QoL were achieved with the addition of an intervention in the form of collagen gel. The authors therefore concluded that 12 weeks of treatment with collagen gel reduced the severity of physical complaints, pain, and local skin symptoms, which greatly influenced QoL in VLU patients.37 These results can be transferred to the findings of the present study. Before study onset, standard of care including compression therapy was already implemented without success, and compression therapy remained the same throughout the study period. Conclusively, keeping the healing-promoting characteristics of collagen and collagen-based wound dressings in mind, improvements of wound size reduction and wound-related QoL observed in the present study are most likely attributable to the native collagen-alginate dressing.
The present findings regarding the correlation between the QoL wellbeing sub-score and reduced wound area are supported by a study by Barnsbee et al which agrees with the association between wound area and QoL.11 The authors assessed healing times of VLUs managed according to guideline recommendations and compared them with VLUs treated by standard care. The study indicated that significantly faster healing times, as occurring in VLUs managed with optimal care, could positively affect QoL and social functioning. They also suggested that faster healing may reduce the overall costs of treating VLUs despite the potential additional costs associated with optimal care.11 Guarnera et al investigated the correlation between pain and QoL in patients with vascular leg ulcers.38 They found that this correlation worsened for ulcers of longer duration and those with a larger wound area.38 In contrast, wound healing in the present study did not depend on the wounds’ duration. In line with these studies, Mathias et al reported that 79% of patients whose VLUs had healed within 12 weeks after being treated with a bilayered human skin construct under standard therapeutic compression reported their health to be “much better,” with the greatest improvements observed for pain and other physical symptoms as assessed by a health-related QoL questionnaire.39
In the present study, the percentage of wounds with moderate amounts of exudate decreased by more than 40% within the study period. Interestingly, in another study, a significant association between wound status and QoL in patients suffering from VLUs was demonstrated.17 More precisely, significant correlations between the presence of exudate and QoL, the presence of non-viable tissue and QoL, and the presence of infection/inflammation and QoL were found.17 Consistent with these findings, reduced exudate and significantly improved QoL were found in the present study.
Mean general wound pain levels were significantly reduced after 2 weeks, while pain at dressing changes was completely absent after 1 week of treatment in the present study. Furthermore, the use of analgesics was reduced, and the number of pain-free patients increased by 34% to include nearly half of the participants by the final visit after 4 weeks of treatment. These results are comparable to the findings of a study investigating 3 different primary dressings used under compression: 2 hydrocolloid dressings and a superabsorbent polyurethane dressing.40 The authors of that study reported a significant decrease in pain levels as measured by VAS scores after 2 weeks compared with baseline across all 3 groups. Similarly, the number of pain-free patients increased by approximately 40% after 4 weeks of treatment.40 In contrast to the study by Guarnera et al, which found an association between pain, wound area, and QoL in patients with vascular leg ulcers,38 no correlation between pain and QoL was detected in the present study, as well as in a study by González de la Torre et al.17 It is noteworthy that the herein investigated collagen-alginate dressing was able to reduce even severe levels of pain, making it a useful tool in the management of VLU-related pain.
The observed wound area reduction of 32.2% is comparable to that of a previous study assessing the efficacy of the same collagen-alginate dressing in combination with standard care in the management of chronic wounds of various etiologies.41 The mean wound area reduction observed in the previous study measured 38.1% and was achieved after 3 weeks of treatment.41 In this context, it is important to note that the present study was conducted during the COVID-19 pandemic, which led to a significant decrease in care compared to previous years.42 This reduction was characterized by fewer face-to-face clinician visits, reduced referrals to specialists, and a smaller number of prescriptions for wound care products. As a result, healing rates of VLUs decreased, and the time required for VLUs to heal increased.42 Nevertheless, treatment with the collagen-alginate dressing in conjunction with debridement and compression therapy was able to kick-start wound healing in previously persistent VLUs. Furthermore, the dressing was positively rated by participating health care professionals with regard to its handling and performance and by patients with respect to its wearing comfort. Importantly, few adverse events were documented during the study, all of which were unlikely to be related to the collagen-alginate dressing.
Limitations
Even though this study provides evidence that the native collagen-alginate dressing promotes healing of hard-to-heal wounds under compression, thereby significantly improving QoL, the non-controlled nature of the study limits its significance. Further randomized, controlled clinical trials or multi-institutional studies should therefore be conducted to confirm these promising results. Future studies could consider the description of covers and type of compression.
Conclusions
In this prospective, descriptive, post-marketing surveillance study, 50 patients with VLUs that had persisted for 1.5 to 24 months were treated with standard wound care and a collagen-alginate dressing over a 4-week period. During this time, 4 wounds healed completely and no adverse events occurred. Wound size decreased by an average of 32.2%, which was accompanied by a reduction of wounds with moderate exudate. Wound pain decreased after only 2 weeks, and patients’ total wound-related QoL improved significantly after 4 weeks. There was a significant correlation between the QoL wellbeing sub-score and reduction in wound area.
The study indicates that treating patients with a collagen-alginate dressing together with standard treatment can improve VLU outcomes in terms of wound size reduction, pain, and QoL, even in stalled, hard-to-heal ulcers that had previously not responded to standard therapy. In conclusion, the collagen-alginate dressing is a safe and effective dressing to promote wound healing of hard-to-heal and complex VLUs and adequately address pain experienced by patients. Due to the positive correlation between reduced pain and VLU healing suggested in literature, these effects may contribute to each other. By reducing the wound area and presumably by lowering wound pain and exudate levels, the dressing also has a direct positive impact on patients’ QoL. Consequent shorter treatment periods and improved QoL as a result of the dressing may ultimately lead to reduced personal and socioeconomic costs. The exact association between these parameters is beyond the scope of the present study and will need to be elucidated in future investigations. Further randomized, controlled trials or multi-institutional studies may demonstrate further efficacy of the product.
Acknowledgments
Authors: Alisha Oropallo, MD1,2,3; Amit Rao, MD1; Sally Kaplan, RN1; Farisha Baksh, BS1; Christina Del Pin, MD1,2; and Julie Isgro, NP1
Affiliations: 1Northwell Health System, Department of Surgery, Comprehensive Wound Care Healing and Hyperbaric, Lake Success, NY; 2Donald & Barbara Zucker School of Medicine at Hofstra/Northwell, Hempstead, NY; 3Northwell Health System, Department of Surgery, North Shore University Hospital, Manhasset, NY
Correspondence: Alisha Oropallo, MD; Northwell Health Comprehensive Wound Healing Center & Hyperbaric, 1999 Marcus Avenue Suite M6, Lake Success, New York 11042; aoropallo@northwell.edu
Disclosure: This study was funded by BSN Medical GmbH, Essity Group (Hamburg, Germany).
References
1. Raffetto JD, Ligi D, Maniscalco R, Khalil RA, Mannello F. Why venous leg ulcers have difficulty healing: overview on pathophysiology, clinical consequences, and treatment. J Clin Med. 2021;10(1):29. doi:10.3390/jcm10010029
3. Schneider C, Stratman S, Kirsner RS. Lower extremity ulcers. Med Clin North Am. 2021;105(4):663-679. doi:10.1016/j.mcna.2021.04.006
4. Ferreira MC, Tuma P Jr, Fernandes Carvalho V, Kamamoto F. Complex wounds. Clinics (Sao Paulo). 2006;61(6):571-578. doi:10.1590/s1807-59322006000600014
5. Gethin G, Cowman S, Kolbach DN. Debridement for venous leg ulcers. Cochrane Database Syst Rev. 2015(9):CD008599. doi:10.1002/14651858.CD008599.pub2
6. National Institute for Health and Care Excellence. Chronic wounds - advanced wound dressings and antimicrobial dressings. NICE Guideline ESMPB2. 2023;1-43. https://www.nice.org.uk/guidance/esmpb2
7. Norman G, Dumville JC, Westby MJ, Stubbs N, Soares MO. Dressings and topical agents for treating venous leg ulcers. Cochrane Database Syst Rev. 2018;6(6):CD012583.
8. Scottish Intercollegiate Guidelines Network. Management of chronic venous leg ulcers - a national clinical guideline. Guidance 120. 2010;1-46. https://www.oxfordhealth.nhs.uk/wp-content/uploads/2015/08/SIGN-Guidelines-foer-the-Management-of-Venous-Leg-Ulcers.pdf
9. Augustin M, Conde Montero E, Zander N, et al. Validity and feasibility of the wound-QoL questionnaire on health-related quality of life in chronic wounds. Wound Repair Regen. 2017;25:852-857. doi:10.1111/wrr.12583
10. Rice JB, Desai U, Cummings AKG, Birnbaum HG, Skornicki M, Parsons N. Burden of venous leg ulcers in the United States. J Med Econ. 2014;17(5):347-356. doi:10.3111/13696998.2014.903258
11. Barnsbee L, Cheng Q, Tulleners R, Lee X, Brain D, Pacella R. Measuring costs and quality of life for venous leg ulcers. Int Wound J. 2019;16(1):112-121. doi:10.1111/iwj.13000
12. Walzer S, Dröschel D, Vollmer L, Atkin L, Ousey K. A cost-effectiveness analysis of a hydration response technology dressing in the treatment of venous leg ulcers in the UK. J Wound Care. 2018;27(3):166-172. doi:10.12968/jowc.2018.27.3.166
14. Leaper D, Münter C, Meaume S, et al. The use of biatain Ag in hard-to-heal venous leg ulcers: meta-analysis of randomised controlled trials. PLoS One. 2013;8(7):e67083. doi:10.1371/journal.pone.0067083
15. Guest JF, Fuller GW, Vowden P. Venous leg ulcer management in clinical practice in the UK: costs and outcomes. Int Wound J. 2018;15(1):29-37. doi:10.1111/iwj.12814
16. Folguera-Álvarez C, Garrido-Elustondo S, Rico-Blázquez M, Verdú-Soriano J. Factors associated with the quality of life of patients with venous leg ulcers in primary care: cross-sectional study. Int J Low Extrem Wounds. 2022;21(4):521-528. doi:10.1177/1534734620967562
18. Leren L, Johansen E, Eide H, Falk RS, Juvet LK, Ljoså TM. Pain in persons with chronic venous leg ulcers: a systematic review and meta-analysis. Int Wound J. 2020;17(2):466-484. doi:10.1111/iwj.13296
19. Kim J, Wilkie DJ, Weaver M, et al. Multidimensional pain characteristics in older adults with chronic venous leg ulcers. Adv Wound Care (New Rochelle). 2021;10(10):544-556. doi:10.1089/wound.2020.1355
20. O’Donnell TF, Jr., Passman MA, Marston WA, et al. Management of venous leg ulcers: clinical practice guidelines of the Society for Vascular Surgery® and the American Venous Forum. J Vasc Surg. 2014;60(2 Suppl):3s-59s. doi:10.1016/j.jvs.2014.04.049
21. O’Meara S, Martyn‐St James M, Adderley UJ. Alginate dressings for venous leg ulcers. Cochrane Database Syst Rev. 2015(8): CD010182. doi:10.1002/14651858.CD010182.pub3
23. Romanelli M, Mulder G, Paggi B, Macchia M, Panduri S, Dini V. The use of a collagen matrix in hard-to-heal venous leg ulcers. J Wound Care. 2015;24(11):543-547. doi:10.12968/jowc.2015.24.11.543
24. Vishwanath V. Quality of life: venous leg ulcers. Indian Dermatol Online J. 2014;5(3):397-399. doi:10.4103/2229-5178.137828
25. Maddox D. Effects of venous leg ulceration on patients’ quality of life. Nurs Stand. 2012;26(38):42-49. doi:10.7748/ns2012.05.26.38.42.c9111
26. Green J, Jester R. Health-related quality of life and chronic venous leg ulceration: part 1. Br J Community Nurs. 2009;14(12):S12-S17. doi:10.12968/bjcn.2009.14.Sup6.45538
27. Heinen MM, Persoon A, van de Kerkhof P, Otero M, van Achterberg T. Ulcer-related problems and health care needs in patients with venous leg ulceration: a descriptive, cross-sectional study. Int J Nurs Stud. 2007;44(8):1296-1303. doi:10.1016/j.ijnurstu.2006.05.001
28. Green J, Jester R. Health-related quality of life and chronic venous leg ulceration: part 2. Br J Community Nurs. 2010;15(3):S4-S10. doi:10.12968/bjcn.2010.15.Sup1.46906
29. World Health Organization. Wound and lymphoedema management. 2010. Accessed July 26, 2023. https://www.who.int/publications/i/item/9789241599139
30. Franks PJ, Barker J, Collier M, et al. Management of patients with venous leg ulcers: challenges and current best practice. J Wound Care. 2016;25(Suppl 6):S1-S67. doi:10.12968/jowc.2016.25.Sup6.S1
31. Nicolaides AN. The most severe stage of chronic venous disease: an update on the management of patients with venous leg ulcers. Adv Ther. 2020;37(Suppl 1):19-24. doi:10.1007/s12325-020-01219-y
32. Harding K. Challenging passivity in venous leg ulcer care - the ABC model of management. Int Wound J. 2016;13(6):1378-1384. doi:10.1111/iwj.12608
34. Mathew-Steiner SS, Roy S, Sen CK. Collagen in wound healing. Bioengineering (Basel). 2021;8(5):63. doi:10.3390/bioengineering8050063
35. Lee C, Lee Y. Collagen-based formulations for wound healing applications. Wound Healing Biomaterials. 2016;2:135-149. doi:10.1016/B978-1-78242-456-7.00007-6
36. Brett D. A review of collagen and collagen-based wound dressings. Wounds. 2008;20(12):347-356.
38. Guarnera G, Tinelli G, Abeni D, Di Pietro C, Sampogna F, Tabolli S. Pain and quality of life in patients with vascular leg ulcers: an Italian multicentre study. J Wound Care. 2007;16(8):347-351. doi:10.12968/jowc.2007.16.8.27856
40. Charles H. Venous leg ulcer pain and its characteristics. J Tissue Viability. 2002;12(4):154-158. doi:10.1016/s0965-206x(02)80024-9
41. Sabo M, Le L, Yaakov RA, Carter M, Serena TE. A post-marketing surveillance study of chronic wounds treated with a native collagen calcium alginate dressing. Ostomy Wound Manage. 2018;64(4):38-43.
42. Guest JF, Fuller GW. Cohort study assessing the impact of COVID-19 on venous leg ulcer management and associated clinical outcomes in clinical practice in the UK. BMJ Open. 2023;13(2):e068845. doi:10.1136/bmjopen-2022-068845
