


Dysphagia and Wounds: Making the Connection
Dysphagia is the medical term for swallowing difficulties. It is characterized by the abnormal transfer of a bolus of food or liquid from the mouth to the stomach involving any of the 3 stages of swallowing (oral, pharyngeal, or esophageal). In a large population-based study, 1 in 6 adults reported experiencing difficulty swallowing.1 In long-term care facilities, the prevalence of dysphagia is likely much higher, but limited data is available. The older age of nursing home residents and common comorbidities (including neurological diseases, strokes, and dementia, plus polypharmacy) are all factors of why dysphagia is encountered commonly in long-term care facilities.
Dysphagia can lead to significant health issues, such as dehydration, malnutrition, fatigue, aspiration, pneumonia, and a general decline in functional status.2 These factors often contribute to skin breakdown and prolonged wound healing. Proper evaluation and management of dysphagia can facilitate marked improvements in nutrition and hydration and, ultimately, skin integrity and wound healing.
SIGNS AND SYMPTOMS OF DYSPHAGIA
Patients with dysphagia display a variety of clinically observable signs, symptoms, and complaints related to eating or swallowing. Some of the problems encountered include2,3:
- Inability to keep a bolus of food in the mouth
- Difficulty in gathering the bolus in the back of the tongue
- Food remaining in the mouth after swallowing
- Taking too long to eat solid foods
- Eating only soft foods
- Hesitation or inability to initiate swallowing
- Coughing or choking when drinking or eating (or after eating)
- Hoarseness or a wet voice quality
- Frequent throat clearing
- Sensation of food stuck in the throat or at the bottom of the neck
- Nasal regurgitation
- Frequent repetitive swallowing
- Avoiding social dining
- Dry mouth or lack of saliva
- Drooling or excessive saliva
- Pocketing food in the cheek
- Pain with swallowing
Any single or a combination of these issues may lead to reduced food intake, subsequent unintended weight loss, and loss of lean body mass, which ultimately affects wound development and healing.
Dysphagia also takes a psychological toll on its sufferers, which can further compromise health. Many social activities and forms of entertainment involve eating and drinking, often in the presence of friends, family members, and coworkers. If a person experiences major changes in the swallowing process, this can lead to feelings of shame, anxiety, depression, fear of eating, and isolation, which significantly impact quality of life.3 Therefore, identifying a person who has difficulty swallowing is important in order to manage this condition before severe psychological and physical consequences develop.
THE LINK BETWEEN DYSPHAGIA AND WOUNDS
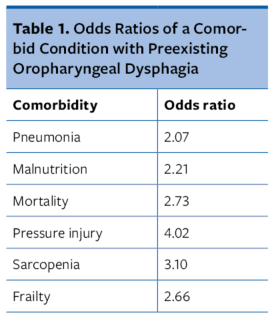
In 2022, a meta-analysis4 examined the pooled prevalence of oropharyngeal dysphagia (OD) and the risk of certain comorbidities and geriatric syndromes, several of which are related to nutrition. This analysis included 39 studies with 31,488 participants and determined the odds ratio (OR) for each comorbidity.
An OR is a statistic that quantifies the strength of the association between two events, A and B. An OR of 1 indicates the 2 events are independent (ie, the odds of one event are the same in either the presence or absence of the other event). If the OR is greater than 1, then A and B are associated (correlated) in the sense that, compared with the absence of B, the presence of B raises the odds of A.
It is important to understand the link between dysphagia and other medical conditions, particularly wounds, because they are often treated as unrelated diagnoses, while the research clearly finds they are interrelated. In fact, this study determined the participants with OD were 2.21 times more likely to be at risk for malnutrition, and 4.02 times more likely to be at risk for pressure injuries. Table 1 lists additional associations uncovered by this analysis.
DYSPHAGIA TREATMENT AND MANAGEMENT
In addition to good oral hygiene, the intervention strategies typically utilized for patients with dysphagia are classified as compensatory, rehabilitative, and diet modification.
Compensatory Strategies. Interventions for dysphagia management in the elderly are traditionally compensatory. They aim to alter the swallow pattern but do not provide any lasting functional change. In other words, these techniques help patients who cannot or have not yet received rehabilitation. The aims of most of these techniques are to reduce bolus size or redirect the path of the bolus to protect the airway, prevent aspiration, and improve bolus clearance. However, it is important to keep in mind that these are all temporary fixes, and it is necessary to use these techniques with every single swallow to achieve effectiveness.
Examples of postural compensatory mechanisms include sitting upright (90˚-seated angle), head rotations, and a simple chin tuck when swallowing. Other compensatory techniques, such as having the patient swallow 3 times, cough to clear the residue before taking the next bite, or reduce the rate and amount food and liquids consumed, are designed to change swallowing behavior. It is necessary to communicate and remind patients about the following recommendations as suggested interventions2,5:
- Eat slowly and allow ample time for a meal
- Take small amounts of food or liquid into the mouth using a teaspoon
- Concentrate on swallowing—eliminate distractions, such as television
- Avoid mixing solid food with liquids in the mouth at the same time
- Place food on the stronger side of the mouth if the patient has unilateral weakness
- Alternate between solids and liquids to wash down residue
- Use sauces, gravies, and condiments liberally to help lubricate foods and prevent fragmentation
- Have the caregiver provide verbal cues to help with cognitive and attention difficulties
- Include cold food items—a cool temperature facilitates swallowing
Rehabilitative Strategies. Rehabilitative techniques include exercises and maneuvers that are designed to create lasting change in an individual’s swallowing by improving underlying physiological function over time.5 Swallowing exercises include exercises of the lips, jaw, tongue, soft palate, pharynx, larynx, and/or respiratory muscles to improve function. Maneuvers are specific strategies that clinicians use to change the timing or strength of movements of swallowing. Some maneuvers require following multistep directions, making them inappropriate for some patients with cognitive impairments.
A speech language pathologist, also known as a speech therapist, can determine the appropriate treatment. These healthcare professionals are trained to conduct bedside swallowing evaluations that include history, oropharyngeal sensorimotor assessment, and evaluation of trial swallows of foods and liquids of varying consistencies to determine what exercises and/or maneuvers may benefit the patient.
Diet Modification. Diet modification of food texture and/or fluid consistency is a nutritional approach commonly utilized for dysphagia management. Swallowing thin liquids, such as water, juice, coffee, or tea, requires coordination and control because these fluids are aspirated easily into the lungs, which may lead to pneumonia. A patient who has difficulty consuming thin liquids sometimes is given liquids with greater viscosity, which are thickened by adding nonfat dry milk powder, cornstarch, or commercial thickeners.
If necessary, it is possible to alter food consistency mechanically (softened or pureed). In addition, patients must avoid certain foods that are difficult to swallow, such as extremely hard or chewy foods. When offering food to the patient with dysphagia, it is important to remember that food, no matter the consistency, needs to look, smell, and taste good in order for the patient to consume it. Attractive plate presentations, including the use of food molds to approximate the original look of the pureed foods, aromatic ingredients, and strong flavors to enhance the appeal of pureed foods, are of utmost importance.6
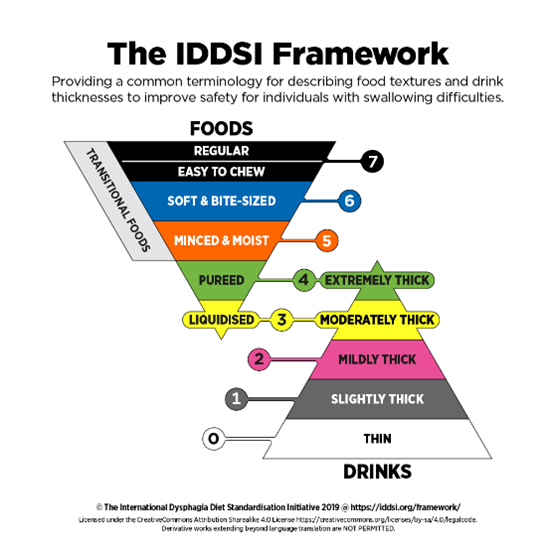
The International Dysphagia Diet Standardization Initiative (IDDSI) is a global initiative to improve the lives of people with dysphagia around the globe. Its framework provides common terminology for describing food textures and drink thicknesses in order to improve safety for individuals with swallowing difficulties. The IDDSI framework consists of a continuum of 8 levels (0-7). Drinks are measured from Levels 0 to 4, while foods are measured from Levels 3 to 7.
Figure 1 depicts the IDDSI framework. It is important for clinicians to become familiar with this framework because nutritional supplements often are marked with an IDDSI level. For example, Expedite Cup (Medtrition) is currently the only available therapeutic nutrition supplement to support wound healing designed with the dysphagia patient in mind. It is a gelatin consistency that is IDDSI Level 4 (spoon/pudding thick). The availability of wound-specific products for patients with dysphagia has become crucial as more is learned about the odds of developing a pressure injury with preexisting dysphagia and the role of nutrition in wound healing.
PRACTICE POINTS
Patients who are consuming inadequate amounts of foods or fluids because of swallowing problems are at risk for a variety of nutritional problems that will, in turn, impact their ability to heal a wound. It is imperative to identify dysphagia so that treatment can start as soon as possible. Identification, diagnosis, and treatment of this disorder requires an interdisciplinary team approach, including speech and nutrition professionals. With compensatory strategies, proper food consistencies, the new generation of wound-specific products for dysphagia, and some compassion, patients can learn to swallow easily and safely and consume all the calories, protein, and fluids they require for wound healing.
Nancy Collins, PhD, RDN, LD, NWCC, FAND, is a wound-care-certified registered dietitian nutritionist based in Las Vegas, NV. Dr. Collins is well known for her expertise in the complex relationship between malnutrition, body composition, and tissue regeneration. To contact Dr. Collins, visit her website at www.drnancycollins.com
References
1. Adkins C, Takakura W, Spiegel BMR, et al. Prevalence and characteristics of dysphagia based on a population-based survey. Clin Gastroenterol Hepatol. 2020;18(9):1970-1979.e2. doi:10.1016/j.cgh.2019.10.029
2. Niedert KC. Nutrition Care of the Older Adult: A Handbook of Nutrition throughout the Continuum of Care. Academy of Nutrition and Dietetics; 2016:149-153.
3. Dylczyk-Sommer A. Dysphagia. part 1: general issues. Anaesthesiol Intensive Ther. 2020;52(3):226-232. doi:10.5114/ait.2020.98074
4. Banda KJ, Chu H, Chen R, et al. Prevalence of oropharyngeal dysphagia and risk of pneumonia, malnutrition, and mortality in adults aged 60 years and older: a meta-analysis. Gerontology. 2022;68(8):841-853. doi:10.1159/000520326
5. American Speech-Language-Hearing Association. Adult dysphagia. Accessed April 11, 2023. https://www.asha.org/practice-portal/clinical-topics/adult-dysphagia/#collapse_6
6. Mahan KL, Escott-Stump E, Raymond, JL. Krause’s Food and the Nutrition Care Process. 13th ed. Elsevier; 2011:929-933.
