



Application of Clinician Support Tools to Improve Wound Healing Outcomes and Simplify Treatment Selection for Effective Exudate Management
© 2024 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Wounds or HMP Global, their employees, and affiliates.
Abstract
Background. Achievement of moisture balance can be a critical factor affecting time to closure of nonhealing wounds, and dry wounds can take much longer to heal than those with high exudate levels. Whether the goal of management is to donate moisture to the wound or control excessive fluid until the cause has been identified and addressed, choice of dressing and other wound management products can affect nursing resources, clinical outcomes, concordance, and quality of life for the patient. Case Reports. The cases discussed illustrate differences in management approaches for dry and wet wounds and show how clinician support tools (eg, tissue type, infection/inflammation, moisture imbalance, epithelial edge advancement [TIME] clinical decision support tool) can facilitate treatment decisions. Dressing selection in particular can be challenging given the range of wound types, increasing demands on wound care practitioner time and the requirements necessitated by individualized patient treatment goals. Development of wound management decision tools can help to simplify product selection, and use of patient discussion guides can help to identify patients and caregivers who have the confidence to help implement their wound management plan. Conclusion. Adopting wound management decision tools has the potential to ease the increasing burden of wound care to health care systems, patients, and society.
Abbreviations: CDST, clinical decision support tool; NPWT, negative pressure wound therapy; TIME, tissue, infection/inflammation, moisture imbalance, epithelial edge advancement.
Background
Addressing moisture imbalance can be a critical factor affecting successful closure of nonhealing wounds.1 Both excess and insufficient moisture levels can impede wound healing; however, dry wounds have been shown to take approximately twice as long to heal as highly exuding wounds.1,2 Prolonged healing time is not only burdensome for patients, but also increases the total cost of wound care.3
Low or insufficient exudate levels can occur in wounds toward the end of the healing process, in those with dry eschar or with tissue ischemia, in patients who are severely dehydrated, or even with inappropriate use of a dressing, device, or intervention.1 In all cases of insufficient exudate production, the aim of treatment is to donate moisture to the wound, reduce damage to the wound bed, and help prevent and/or manage pain.
For wounds with excess moisture, it is important to identify and manage the cause. Where infection is the underlying cause, topical (eg, silver or iodine-based dressings, or polyhexamethylene biguanide) or combined topical and systemic antimicrobial therapy (eg, antibiotics) will be necessary.1,4 In more complex cases, biofilm involvement should be investigated and treated with repeated debridement (mechanical, autolytic, or enzymatic) and maintenance desloughing along with topical antimicrobials.4,5 In cases in which arterial involvement has been ruled out, compression therapy is considered to be the standard for managing excessive exudate and edema caused by venous insufficiency.6
Ultimately, moisture levels can be managed using a range of products depending on the options available to the treating clinician and the nature of the wound; these include products such as alginate, hydrofiber, hydrogel, and hydroconductive dressings, as well as NPWT.1,7 However, foam dressings are often a preferred and easy option for exudate management and are used either as the primary or as a secondary dressing. It is critical to routinely reevaluate moisture balance and frequency of dressing changes to ensure the dressing and/or therapy selection remains appropriate, particularly in settings in which dressing use may be restricted or scrutinized (eg, US Medicare restrictions on foam dressing usage in some settings). Choice of product for managing moisture imbalance can potentially affect healing times, influence patient quality of life, and even affect cost-effectiveness.⁸ Rationalizing the range of available products to wound care practitioners can facilitate treatment decisions. Identifying and recommending preferred treatments for specific wound types or a dressing range with features that suit most wound management requirements (eg, minimizing dressing change frequency, masking strikethrough, minimizing pain at dressing change, managing odor) could aid clinical decision-making and help provide a consistent approach to wound management. Incorporation of product recommendations into a decision tree can also help bring consistency to management approaches.
One example of a decision tree that was developed and implemented at a community-based acute care facility in the Greater Toronto Area in Canada as part of a basic guide to wound assessment, management approaches, and dressing selection, is provided in Figure 1.
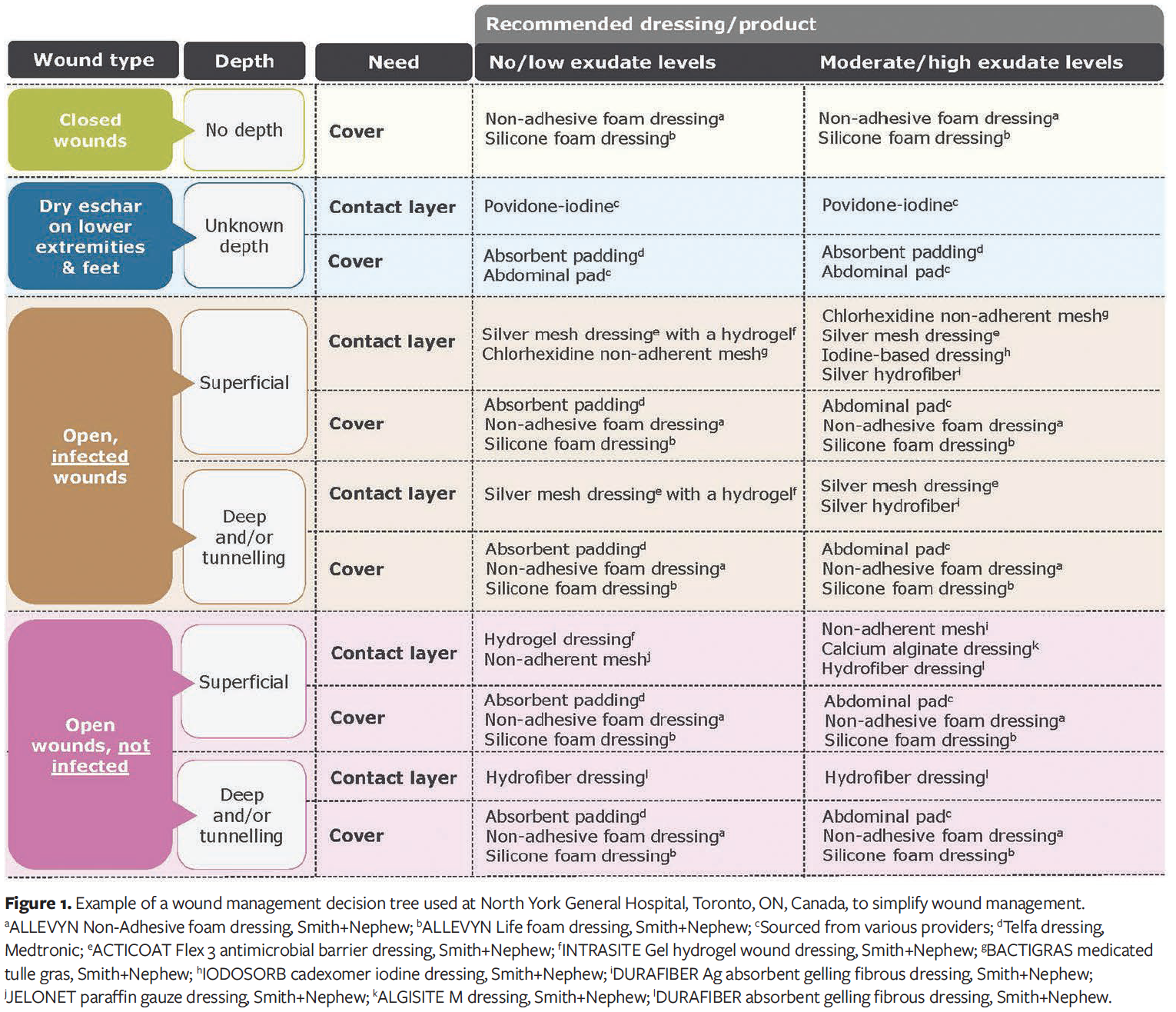
Alongside supporting wound management resources, a decision tree can be used to aid selection of the most appropriate treatment approach for each wound using the products available, while developing a comprehensive care plan tailored to the patient based on the TIME (Tissue type [non-viable/deficient], Infection/Inflammation, Moisture imbalance, Epidermis/Edges [non-advancing or undermined]) principles (Figure 2).
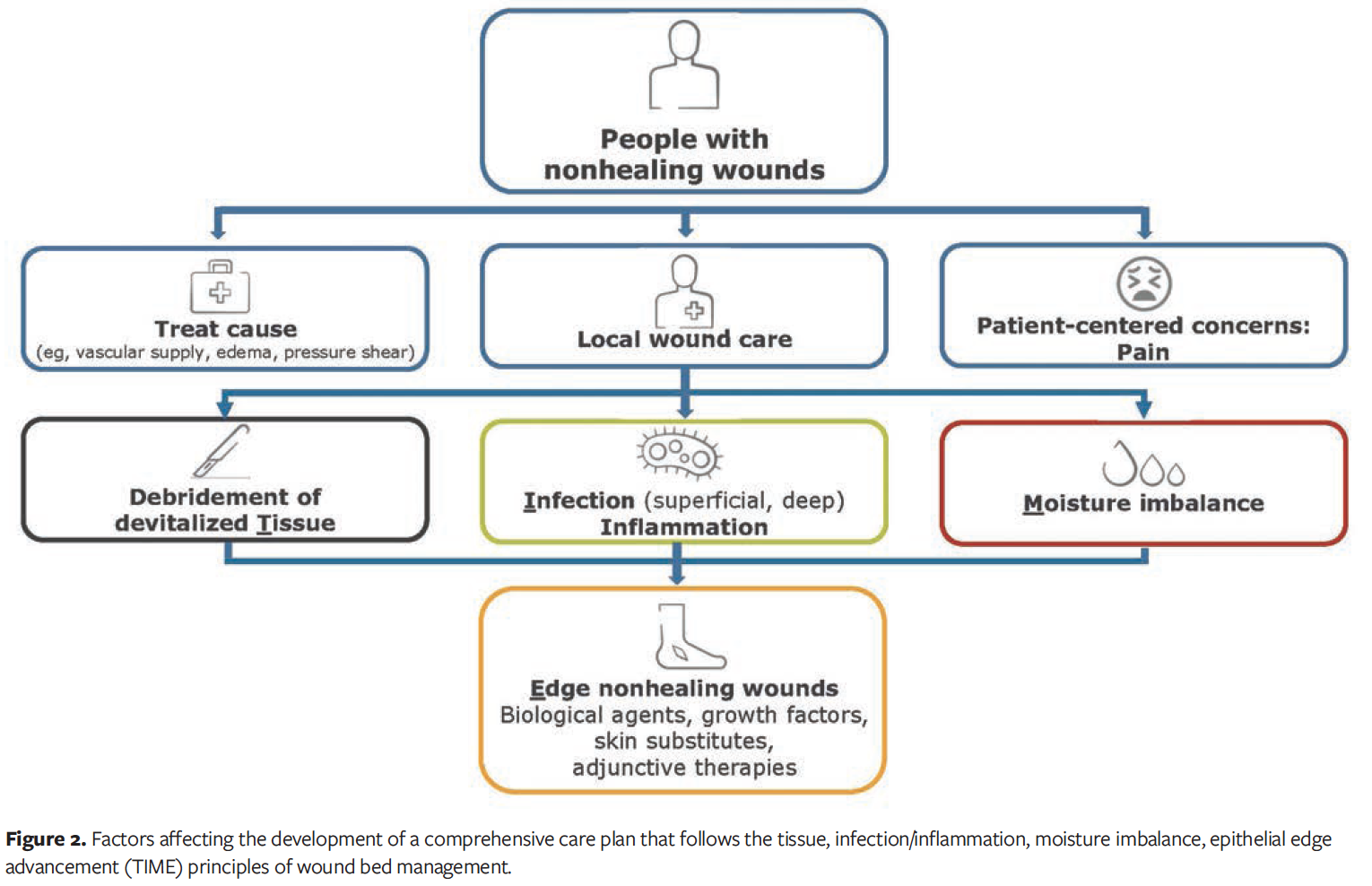
TIME is one of the most widely used tools to help manage wound exudate levels as part of effective wound bed preparation and assessment. The tool encourages wound care practitioners to evaluate the tissue types present in the wound bed, the presence of inflammation and infection, moisture balance, and wound edge status.9 In 2019, a 1-page TIME-related prompt for practice—the CDST—was developed that uses an A, B, C, D, E approach to facilitate wound assessment, selection of appropriate treatments, and determination of short-term goals: Assess patient well-being and wound, Bring in multidisciplinary team and informal caregivers to promote holistic patient care, Control or treat underlying causes and barriers to wound healing, Decide appropriate treatment and determine short-term goals, and Evaluate and reassess the treatment and wound management outcomes.10
The TIME principles embrace holistic care and make patient needs and personal treatment goals a key focus. As appropriate, products with patient-friendly features can facilitate an increased role for patients and caregivers in wound management. For example, using a so-called shared care approach to decision making, health care professionals can work with patients to determine if they are willing to and capable of performing their own dressing changes.11-13 This approach could potentially free up time for wound care professionals to provide increased support to patients with complex wounds that require more frequent monitoring and dressing changes.11,14 Experiences with application of moisture management principles using a TIME CDST approach and a bespoke wound management resource with decision tree are shared in the following 3 case studies, demonstrating careful ongoing evaluation of the wound type and status and treatment goals, using the products available to the treating clinicians at the time within their institutions.
Case Reports
These cases examine the challenges of managing multiple wounds with varying exudate levels. The first case, from a community-based acute care facility, explores the complexities of managing a wound with no-to-low exudate levels with the aid of a decision tree (Figure 1). The second and third cases focus on patients treated in a community home health care setting. The second case discusses how multiple wounds of differing exudate levels were managed. The third case specifically highlights the treatment of a patient using a shared care approach for a particularly challenging surgical wound. These cases are intended for the education of wound care practitioners. Every effort has been made to maintain the anonymity of the patients.
Case 1
A 74-year-old male who sustained head injuries related to a fall at home and who had been lying on the floor for approximately 3 days, presented with an unstageable pressure injury to the right greater trochanter (Figure 3A). The patient had a history of type 2 diabetes, hypertension, hypothyroidism, acute kidney injury, osteoarthritis, and atrial fibrillation, and was taking an oral anticoagulant (apixaban). Daily use of an iodine-based sheet on the wound at the previous hospital had dehydrated the wound base. The wound was dry, leathery, ischemic, and sloughy, with a small amount of purulent discharge.
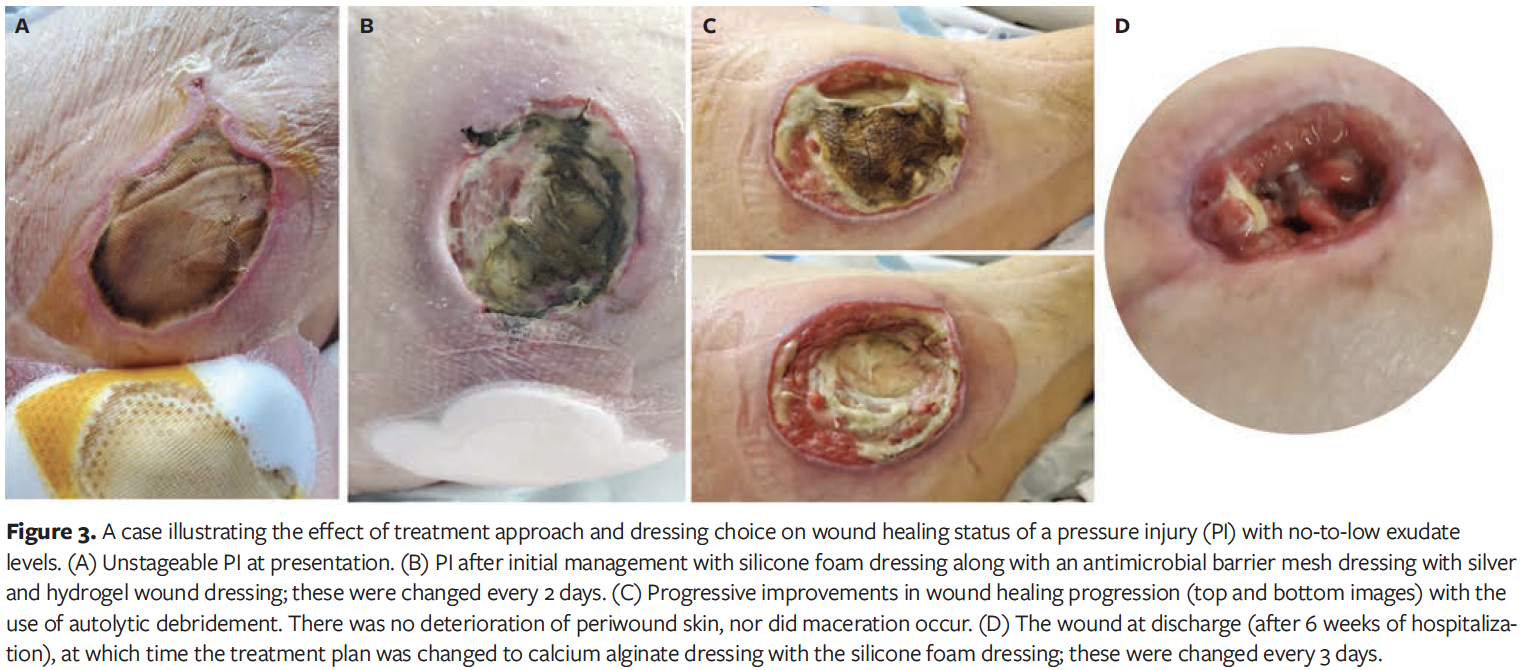
Sharp wound debridement would have been the first-choice treatment approach; however, this patient had a high risk of bleeding and therefore, conservative care was preferable. The wound was dry and the risk of infection was high due to the presence of purulent discharge (coupled with the patient’s age and comorbidities), therefore, the decision tree recommendation was to use a hydrogel wound dressing (INTRASITE Gel; Smith+Nephew) combined with an antimicrobial nanocrystalline barrier dressing with silver (ACTICOAT FLEX 3; Smith+Nephew) that was then covered with an absorbent silicone multilayer foam dressing (ALLEVYN LIFE; Smith+Nephew) to provide a moist wound healing environment (Figure 3B). There were no signs of spreading or systemic infection, and because swabbing necrotic tissue and pus can lead to false-positive results,15 the use of antibiotics was not considered appropriate. Treatment was applied every 2 days due to the risk of infection and an anticipated increase in wound drainage.
As autolytic debridement progressed, wound drainage also increased. Nevertheless, the surrounding skin remained intact and showed no signs of maceration, because the dressing was able to manage the excess fluid (Figure 3C). After 6 weeks in the hospital, the patient was discharged to a rehabilitation institution (Figure 3D). Autolytic debridement was no longer required, and the wound was on a healing trajectory; therefore, the treatment plan was changed to focus on absorption of exudate using an alginate dressing (ALGISITE M; Smith+Nephew), with the same absorbent silicone multilayer foam dressing applied every 3 days, as per the decision tree recommendation for “open wounds, not infected” with “moderate/high exudate levels” (Figure 1).
Case 2
A 30-year-old male who was hepatitis C–positive presented with multiple large lower limb ulcers on his bilateral lower legs. The ulcers were related to a traumatic injury combined with a lack of self-care/personal neglect. Two of the most severe ulcers were located above the heel and on the arch of the foot (Figure 4A). The patient had a complex medical history that included infective endocarditis, methicillin-resistant Staphylococcus aureus, diagnosed depression, and a history of opioid use; in addition, he had recently undergone cardiac tricuspid valve replacement. The patient also had asthma and nephrolithiasis (kidney stones), and follow-up could be difficult because at times it was impossible to contact the patient. The patient was in the hospital for almost 2 months and had several considerations for his wound care—other than the ongoing health conditions—which included recent use of intravenous vancomycin, visible tendon with greater than 2 cm of wound depth around the tendon, slight tunnelling, moderate to large amounts of drainage, and seropurulent discharge.

Despite previous use of a combination of bordered and non-bordered dressings, there was malodor and evidence of leakage and/or strikethrough (Figure 4B). The treatment plan was reevaluated to address ease of use, product comfort, and conformability; exudate volume, color, and consistency; and status of the periwound skin.
An absorbent gelling fibrous dressing containing silver (DURAFIBER Ag; Smith+Nephew) was selected to provide flexibility in addressing wound depth (2-cm depth around the tendon) with slight tunnelling as well as moisture levels, and to help manage any local infection. A non-bordered silicone foam dressing (ALLEVYN Non-Adhesive; Smith+Nephew) was used for additional absorption. The dressing was changed every 2 to 3 days. It was selected because it can be cut to size, thus increasing simplicity to address multiple wounds of various sizes; it is also slightly adherent and does not irritate the skin. Dressings were held in place with a multipurpose elasticized tubular bandage (Figure 4C). Exudate levels were controlled effectively using this revised approach, and substantial progress toward wound closure was achieved.
Case 3
A female with ulcerative colitis had a perianal wound that occurred after an initial abdominoperineal resection failed to close. The wound had been present for more than 1 year, lengthy hospital stays were required, and there were 10-cm tunnels requiring daily wound care. Elective surgery was needed to reopen the incision, perform wound washout, and reattempt primary wound closure. Due to the wound location and the patient’s medical history, the risk of dehiscence was deemed to be high.
After surgery, single-use NPWT at −80 mm Hg (PICO; Smith+Nephew) was used to bolster the incision line and help manage drainage effectively (Figure 5A). Approximately 2 weeks after surgery, the incision dehisced. The wound closest to the vaginal opening measured 3.0 cm wide by 5.5 cm deep; it was the widest wound and was producing moderate-to-large amounts of a creamy-/beige-colored seropurulent discharge. Cultures were positive, and antibiotics were required to help control the infection. The wound measured 3.0 cm to the top end of the incision line, where the depth was 13.0 cm and was producing a small amount of serosanguinous discharge.
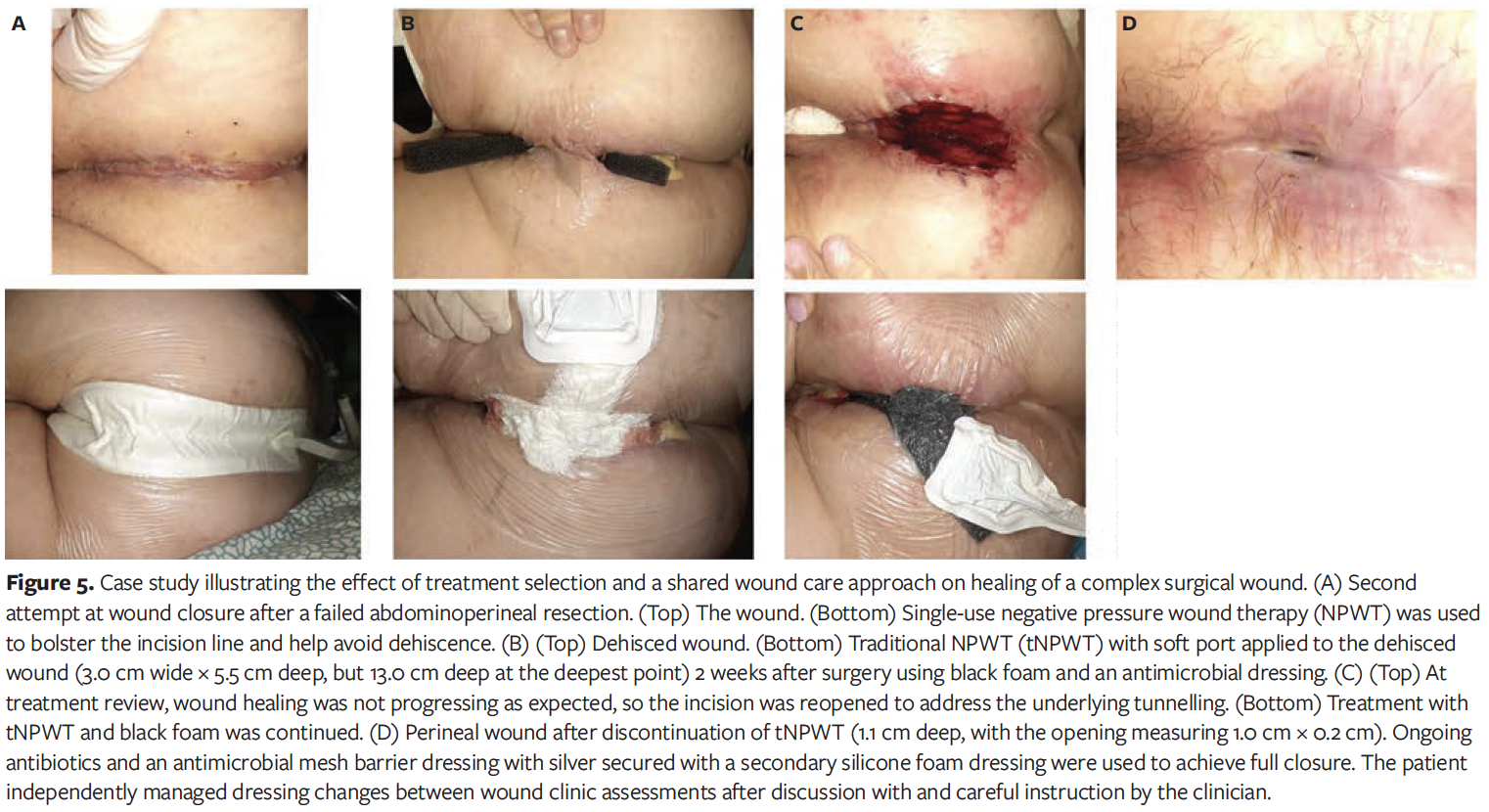
The treatment plan was reviewed and changed to traditional NPWT (−120 mm Hg continuous) using a soft port that avoided the need to track the port away (RENASYS; Smith+Nephew); black foam was used to address the tunnelling and to help wick fluid away more effectively. An antimicrobial dressing impregnated with polyhexamethylene biguanide (Kerlix AMD; H&R Healthcare) was used to connect the 2 tunnels along the incision line (Figure 5B). Wound healing was not progressing to plan, so the incision was reopened to address the tunnelling, and traditional NPWT was recommenced (Figure 5C). Drainage levels and type fluctuated throughout treatment from scant to moderate and from serosanguinous to seropurulent. As wound healing started to progress to plan, traditional NPWT was transitioned back to the aforementioned single-use NPWT system.
After several weeks the wound was approaching full closure, with the wound site closest to the vagina having a depth of 1.1 cm, and the opening measuring 1.0 cm × 0.2 cm (Figure 5D). Nanocrystalline silver dressings were used to help manage the risk of infection. These dressings were applied by the patient and were covered using multilayer silicone foam dressings after careful instruction by the clinician. The patient independently managed dressing changes between wound clinic assessments. Antibiotics were also used until wound closure was achieved.
Discussion
In all 3 cases presented herein, reduction in wound size and optimized quality of life were deemed possible to achieve after careful consideration of each patient’s circumstances and medical history. TIME wound assessment and management principles, including regular evaluation of the chosen treatment approach, were consistently applied. Use of the wound management decision tree made it easy to identify which treatment approach was most appropriate and which of the products available to the treating clinicians were most likely to provide an optimized wound healing environment.
Self-sufficient patients with less challenging wound profiles who are engaged, willing, and capable of self-care may have an increased likelihood of achieving wound healing targets and perhaps even reducing time to healing by being empowered to take more control of their wound management. One analysis estimated that there was potential for up to 45% of patients with a chronic (nonhealing) wound and/or their caregivers to benefit from increased involvement in their own care by participating in care planning and delivery rather than being passive recipients of services.11 Case 3 demonstrated the application of a shared wound care approach both in monitoring the NPWT device and dressing status, and later, once the wound became less challenging, decreasing the frequency of wound, ostomy, and continence nursing and general nursing visits.
Dressings with an evidenced wear time of up to 1 week have the potential to facilitate increased patient involvement in managing their wound care.14 The technology in advanced dressings, such as those included in the decision tree shown in Figure 1, can give patients confidence about a long wear time (with the understanding that exudate is locked away from the wound bed to prevent leakage) and in knowing when a new dressing is required (change indicator).16 It has been estimated that the use of long-wear advanced foam dressings within a shared care approach alone could release approximately 3.5 billion nursing hours globally by 2030 when coupled with supporting educational resources.14 Releasing this time has the potential to improve patient quality of life and allow wound care professionals to commit more time to cases where it is most needed, ultimately optimizing quality of care, wound healing outcomes, and resources.
In order to address a need to simplify and standardize practice, improve resource utilization, and optimize wound healing outcomes, the adoption of a validated wound management support tool (ie, TIME CDST) and a decision tree to aid appropriate product selection was found to be very beneficial. The 3 complex patient cases discussed above illustrate how such tools can be successfully applied in routine practice. Sharing these experiences may help in other health care settings in which a clear need has been identified to reduce the complexity of product selection, improve the consistency of wound care, and empower patients who want more involvement in managing their own wounds.
Limitations
The current case report has limitations. Wound healing outcomes can vary depending on a patient’s medical history and comorbidities, as well as the range of treatments and resources available to each wound care provider. Furthermore, results may differ for patients with similar wounds that are treated in the same way due to variations in local protocols and individualized patient treatment goals. The benefits of adopting wound assessment and management tools should be confirmed in a large group of patients with various challenging wound types.
Conclusion
These 3 cases illustrate how consistently applying the TIME principles of wound management and developing practical tools that simplify treatment decisions and product selection within a health care organization can help achieve individual wound management targets. Although the patients described in the first 2 cases were unable to manage their own wound care, it has been proposed that a considerable proportion of patients and caregivers have the potential to assume greater responsibility for achieving their treatment goals through partial or complete remote management, as illustrated in case 3. Embracing new approaches, such as adoption of shared care practices, could help alleviate the strain on wound care resources, allow wound care practitioners to focus on the most complex cases, and simultaneously enhance the patient experience.
Author & Publication Information
Acknowledgments: The authors would like to thank Ashley Hudson, RN, BSN, NSWOC, IIWCC, for her contribution to the drafting of the manuscript.
Authors: Amanda Loney, BScN, RN, NSWOC, WOCC(C), IIWCC1; Britney Butt, MClSc-WH, BScN, RN, NSWOC, WOCC(C)2; and Sophie Berry, BSc (Hons)3
Affiliations: 1Bayshore Home Health, Mississauga, Ontario, Canada; 2Derma Specialist Consultancy Inc., Toronto, Ontario, Canada; 3Smith+Nephew, Watford, Hertfordshire, UK
ORCID: Berry, 0000-0002-7806-3453
Ethical Approval: All patients provided informed consent for the publication of their cases and related images.
Disclosure: A.L. and B.B. received a consultancy fee for their time participating in the development and writing of this manuscript. S.B. is an employee of Smith+Nephew. No funding (monetary, wound care dressings, or medical devices) was provided by Smith+Nephew for the conduct of the reported case studies.
Correspondence: Sophie Berry; Lead - Global Clinical Strategy Advanced Wound Management, Global Clinical and Medical Affairs, Smith+Nephew, 5 Croxley Green Business Park, Hatters Way, Watford, Hertfordshire, WD18 8YE, UK; sophie.berry@smith-nephew.com
Manuscript Accepted: September 20, 2024
References
1. Schultz G, Tariq G, Harding K, et al. WUWHS Consensus Document—Wound exudate: effective assessment and management. Wounds Int. February 1, 2019. Accessed May 16, 2024. https://woundsinternational.com/world-union-resources/wuwhs-consensus-document-wound-exudate-effective-assessment-and-management/
2. Guest JF, Ayoub N, McIlwraith T, et al. Health economic burden that different wound types impose on the UK’s National Health Service. Int Wound J. 2017;14(2):322-330. doi:10.1111/iwj.12603
3. Guest JF, Fuller GW, Vowden P. Cohort study evaluating the burden of wounds to the UK’s National Health Service in 2017/2018: update from 2012/2013. BMJ Open. 2020;10(12):e045253. doi:10.1136/bmjopen-2020-045253
4. Dowsett C, Bellingeri A, Carville K, Garten A, Woo K. A route to more effective infection management: The Infection Management Pathway. Wounds Int. 2020;11(3):50-57.
5. Murphy C, Atkin L, Swanson T, et al. Defying hard-to-heal wounds with an early antibiofilm intervention strategy: wound hygiene. J Wound Care. 2020;29(Sup3b):S1-S26. doi:10.12968/jowc.2020.29.Sup3b.S1
6. James CV, Murray Q, Park SY, et al. Venous leg ulcers: potential algorithms of care. Wounds. 2022;34(12):288-296. doi:10.25270/wnds/21160
7. Eriksson E, Liu PY, Schultz GS, et al. Chronic wounds: treatment consensus. Wound Repair Regen. 2022;30(2):156-171. doi:10.1111/wrr.12994
8. Mahoney K. Part 4: dressing selection. JCN. 2020;34(5):28-35.
9. World Union of Wound Healing Societies. Strategies to reduce practice variation in wound assessment and management: The T.I.M.E. Clinical Decision Support Tool. Wounds International. 2020. Accessed May 16, 2024. https://woundsinternational.com/world-union-resources/strategies-reduce-practice-variation-wound-assessment-and-management-time-clinical-decision-support-tool/
10. Moore Z, Dowsett C, Smith G, et al. TIME CDST: an updated tool to address the current challenges in wound care. J Wound Care. 2019;28(3):154-161. doi:10.12968/jowc.2019.28.3.154
11. Moore Z, Coggins, T. Clinician attitudes to shared-care and perceptions on the current extent of patient engagement in wound care: results of a clinician survey. Wounds Int. 2021;12(1):48-53.
12. Moore Z, Probst S. Building the business case for shared wound care: a cost-benefit case for service providers. Wounds Int. 2023;14(3):28-33.
13. Loney A, Milne C. Shared wound care and the implementation tipping point: patient engagement to standardise practice. Wounds Int. 2023;14(2):46-53.
14. Moore Z, Loney A, Probst S, Ryan H, Milne C, Meaume S. 3.5 billion hours of nurse time released by 2030: potential efficiency gains from shared care and long-wear advanced foam dressings. Wounds Int. 2022;13(2):32-38.
15. International Wound Infection Institute (IWII) wound infection in clinical practice. Wounds Int. 2022. Accessed December 9, 2024. https://woundsinternational.com/consensus-documents/wound-infection-in-clinical-practice-principles-of-best-practice/
16. Allen D, Hurd T, Saunders C. Reduced weekly dressing changes with a five-layer foam dressing compared with other previosuly used dressings in wounds of mixed aeitiology: results from a systematic literature review and meta-analysis of clinical studies. Abstract. J Wound Manage. 2023:24(2):168.






