



Palliative Management of a Recurrent Destructive Cutaneous Squamous Cell Carcinoma of the Scalp With Brain Exposure
Abstract
Introduction. Squamous cell carcinoma (SCC) is the second most prevalent malignant skin carcinoma. Bone infiltration is uncommon, and invasion of the dura mater and brain parenchyma is rare and possible only in the advanced stages of the disease. Treatment of advanced SCC is challenging and often requires the collaboration of a multidisciplinary team to provide local and systemic treatment. Management of advanced SCC of the scalp involving bones and meninges with brain exposure was described herein. Case Report. An 85-year-old male presented with advanced SCC of the scalp. A vegetative and infiltrating neoplastic ulcer of the frontal and parietal regions with exposure of the brain and extensive meningeal and bone destruction was observed. Because of comorbidities and decisions made by the patient and his family, he did not undergo immunotherapy, radiotherapy, or other invasive treatments. The neoplastic tissue was covered by blood, fibrin, and bacterial colonization. The patient received palliative care in a wound healing clinic twice monthly for 1 year, and daily dressing changes were performed at home. Binding bacteria dressings, silver dressings, and absorbent dressings were used to control exudate and infection. Alginate was used to manage bleeding, and charcoal dressings were used to manage odor. The dressings were covered with gauze and bandage. Additionally, swabs were performed when signs of infection were present and targeted systemic antibiotic treatment administered. Conclusions. Squamous cell carcinoma rarely presents with a devastating and rapid evolution. In this case, the local approach was based on the TIME (tissue, inflammation/infection, moisture imbalance, epithelial edge advancement) concept, with special attention paid to the most significant features of neoplastic wounds (eg, pain, exudate, bleeding, odor). Despite the patient’s serious conditions, he survived for a relatively long time.
How Do I Cite This?
Fidanzi C, Davini G, Dini V, et al. Palliative management of a recurrent destructive cutaneous squamous cell carcinoma of the scalp with brain exposure. Wounds. 2022;34(1):E7-E9. doi:10.25270/wnds/2022.e79
Introduction
Squamous cell carcinoma (SCC) is the second most prevalent malignant skin carcinoma.1 It generally occurs in older patients, and the head and neck are the most common location.1 The precise incidence is unknown, but it has increased in recent years.2 A recent study reported an incidence of advanced SCC of approximately 2.1%.3 Surgery is the first-line treatment, followed by radiotherapy and systemic therapies. Accurate prognosis in the early stages is possible; a 5-year survival rate of 90% has been reported.4 Currently, cemiplimab is the systemic therapy indicated for inoperable advanced SCC or metastatic SCC.5 Bone infiltration is uncommon, and invasion of the dura mater and brain parenchyma is rare and occurs only in advanced stages. Management of advanced SCC is challenging and often requires the collaboration of a multidisciplinary team to provide local and systemic treatment.6,7 The current case report described advanced SCC of the scalp involving bones and meninges with brain exposure.
Case Report
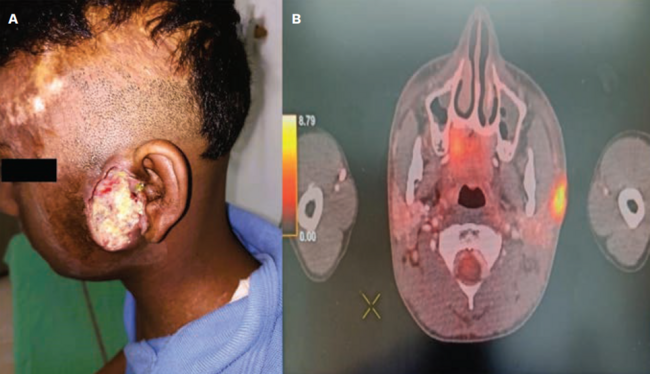
An 85-year-old male presented to the dermatology department for local management of an advanced SCC of the scalp. A vegetative and infiltrating ulcer of the frontal and parietal regions was observed, with exposure of the brain and extensive meningeal and bony destruction. Local invasion of the cranial bones was well documented radiologically (Figure 1). The neoplastic tissue was covered by blood, fibrin, and bacterial colonization (Figure 2A).
The brain parenchyma was not affected, and the patient showed no neurologic symptoms, except for numbness. Despite the invasiveness of the tumor, the patient felt no pain during everyday life; however, he experienced pain during dressing changes. The initial diagnosis of poorly differentiated SCC had been made 2 years previously. The SCC was treated surgically, but it recurred and grew rapidly and aggressively. A second excision was ruled out by the surgeon and the patient’s family because of the patient’s advanced age and comorbidities as well as the invasiveness of the SCC. The patient and his family also refused chemotherapy, immunotherapy, and radiotherapy.
At the initial visit to the dermatology department the patient completed a questionnaire to evaluate his health-related quality of life (HRQoL). The HRQoL was reevaluated every 2 weeks until the patient’s death.
The management and type of dressing were determined by a dermatologist who specializes in wound care. The patient received palliative care in the wound healing clinic twice monthly for 1 year. Additionally, specialized nurses from a public home assistance service performed daily dressing changes at the patient’s home. Binding bacteria dressings, silver dressings, and absorbent dressings were used to control exudate and infection. Alginate was used to manage bleeding, and charcoal dressings were used to manage odor. The dressings were covered with gauze and a bandage. Additionally, when signs of infection were present, swabs were performed; after which, targeted systemic antibiotics were administered. Over the course of 1 year, the patient had a minimum of 4 episodes of infection with fever, all of which were successfully managed with systemic antibiotic therapies. In the patient’s final month of life, his clinical condition deteriorated, and he experienced severe bleeding (Figure 2B, 2C).
Tranexamic acid and compressive alginate did not control the last bleeding episode, and the patient was hospitalized urgently. The patient died a few days later.
Discussion
Squamous cell carcinoma rarely presents with a devastating and rapid evolution. Immunosuppression, localization, recurrence, histology, and late diagnosis correlate with a poor prognosis.3 Extension to the calvarial bones and dura is rare in SCC and other cutaneous malignancies and can lead to devastating outcomes. Because of the patient’s comorbidities and the decisions made by himself and his family, he did not receive immunotherapy, radiotherapy, or other invasive treatments.
To the knowledge of the authors of the current study, few studies have focused on similar cases of advanced cutaneous malignancies of the scalp infiltrating the bones, meninges, and brain. In those studies, the neoplastic ulcers were managed either with surgery and palliative care,8 or with surgery and negative pressure wound therapy, though it is generally contraindicated for neoplastic wounds.9 The local approach to neoplastic wounds is palliative, and such care is fundamental for patients’ quality of life. In the present case, the local approach was based on the TIME (tissue, inflammation/infection, moisture imbalance, epithelial edge advancement) concept,10,11 with special attention paid to the most significant features of neoplastic wounds, such as pain, exudate, bleeding, and odor. In the initial phase of treatment, the dressings were changed every 2 days; however, this did not adequately contain the exudate and bad odor, so daily changes were prescribed. At times the dressings were insufficient to control the bacteria burden, and therefore, binding bacteria dressings were added. Secondary dressings (polyurethane foam dressings) were added to control the exudate. The alginate dressing helped manage bleeding, which occasionally occurred during dressing changes.
Limitations
The main limitation of this case report is that it includes only a single case. In addition, the therapy was only palliative.
Conclusions
Despite the seriousness of the patient's conditions reported herein, he survived for a relatively long time with only local dressings and systemic antibiotics. The patient experienced an approximately 35% improvement in HRQoL compared with the access visit. This HRQoL was maintained until just before the patient’s death.
Acknowledgments
Authors: Cristian Fidanzi, MD; Giulia Davini, RN; Valentina Dini, MD, PhD; Giammarco Granieri, MD; Antonella Vietina, RN; Marco Romanelli, MD, PhD; and Agata Janowska, MD
Affiliation: University of Pisa, Pisa, Italy
Disclosure: The authors disclose no financial or other conflicts of interest.
ORCID: Cristian Fidanzi, 0000-0002-9189-9204; Agata Janowska, 0000-0002-2271-3859; Valentina Dini, 0000-0002-8537-1999; Giulia Davini, 0000-0001-7545-649X; Marco Romanelli, 0000-0002-4127-0141
Correspondence: Agata Janowska, MD, Fellow, University of Pisa, Dermatology, Via Roma 67, Pisa, Pisa 56126 Italy; dottoressajanowska@gmail.com
Recommended Citation: Fidanzi C, Davini G, Dini V, et al. Palliative management of a recurrent destructive cutaneous squamous cell carcinoma of the scalp with brain exposure. Wounds. 2022;34(1):E7-E9. doi:10.25270/wnds/2022.e79
References
1. Waldman A, Schmults C. Cutaneous squamous cell carcinoma. Hematol Oncol Clin North Am. 2019;33(1):1–12. doi:10.1016/j.hoc.2018.08.001
2. Que SKT, Zwald FO, Schmults CD. Cutaneous squamous cell carcinoma: incidence, risk factors, diagnosis, and staging. J Am Acad Dermatol. 2018;78(2):237–247. doi:10.1016/j.jaad.2017.08.059
3. Venables ZC, Autier P, Nijsten T, et al. Nationwide incidence of metastatic cutaneous squamous cell carcinoma in England. JAMA Dermatol. 2019;155(3):298–306. doi:10.1001/jamadermatol.2018.4219
4. Bander TS, Nehal KS, Lee EH. Cutaneous squamous cell carcinoma: updates in staging and management. Dermatol Clin. 2019;37(3):241–251. doi:10.1016/j.det.2019.03.009
5. Ahmed SR, Petersen E, Patel R, Migden MR. Cemiplimab-rwlc as first and only treatment for advanced cutaneous squamous cell carcinoma. Expert Rev Clin Pharmacol. 2019;12(10):947–951. doi:10.1080/17512433.2019.1665026
6. Chabaane M, Ayadi K, Rkhami M, et al. Management of a recurrence of a squamous cell carcinoma of the scalp with extension to the brain: a case report and literature review. Surg Neurol Int. 2020;21;11:347. doi:10.25259/SNI_356_2020
7. Wollina U, Kittner T, Nowak A. Non melanoma skin cancer with skull infiltration and cranial involvement. Open Access Maced J Med Sci. 2019 30;7(18):3030–3033. doi:10.3889/oamjms.2019.416
8. Handler MZ, Goldberg DJ. Cutaneous squamous cell carcinoma of the scalp extending to the skull: a case report and review of the literature. J Cosmet Dermatol. 2018;17(2):232–234. doi:10.1111/jocd.12378
9. Cai SS, Gowda AU, Alexander RH, Silverman RP, Goldberg NH, Rasko YM. Use of negative pressure wound therapy on malignant wounds—a case report and review of literature. Int Wound J. 2017;14(4):661–665. doi:10.1111/iwj.12665
10. Janowska A, Davini G, Dini V, Iannone M, Morganti R, Romanelli M. Local management of malignant and unresectable fungating wounds: PEBO assessment. Int J Low Extrem Wounds. 2021:15347346211053478. doi:10.1177/15347346211053478
11. Janowska A, Dini V, Oranges T, Iannone M, Loggini B, Romanelli M. Atypical ulcers: diagnosis and management. Clin Interv Aging. 2019;14:2137–2143. doi:10.2147/CIA.S231896









{kind=link}
{kind=link}
{kind=link}