



Primary Cutaneous Mucormycosis of the Lower Extremity in a Male Patient With Diabetes
Abstract
Introduction. Mucormycosis is a rare but serious angioinvasive fungal infection that can affect the cutaneous system. Primary cutaneous mucormycosis is caused by direct inoculation and is most prevalent in immunocompromised hosts, particularly those with diabetes. A high index of suspicion is necessary for this condition in patients with rapid and deep extension of necrosis despite aggressive surgical intervention. Deep tissue specimens should be sent for fungal culture and histologic analysis for confirmation of the diagnosis. Early and aggressive debridement to prevent spread to deeper tissues and organs, concurrent antifungal therapy, and medical management of comorbidities are paramount to the treatment of primary cutaneous mucormycosis. Case Report. This case report highlights the presentation and recommended treatment of primary cutaneous mucormycosis in 1 patient for reduced morbidity and mortality associated with this type of infection.
Introduction
Necrotizing soft tissue infection is commonly bacterial in origin; however, acute fungal infection can occur.1 Mucormycosis, also known as zygomycosis, is a rare but serious angioinvasive fungal infection caused by a group of saprophytic fungi in the order Mucorales, subphylum Mucoromycotina.1-5 These highly aggressive fungal organisms affect the rhino-orbital-cerebral, pulmonary, gastrointestinal, and cutaneous systems.1,2 Cutaneous mucormycosis is classified into primary and secondary infection. Primary infection is most frequently associated with direct inoculation via trauma when the spores enter the skin.3 The secondary form occurs via dissemination from other locations. If not treated early, cutaneous mucormycosis can invade fascia, muscle, tendon, and bone, and ultimately disseminate into the bloodstream, resulting in a considerably increased mortality rate.2 Common risk factors for cutaneous mucormycosis are hematologic malignancies, history of hematopoietic cell transplantation, and diabetes.1,2,4-7 This case report highlights a patient with cutaneous mucormycosis, including findings that led to increased suspicion of the diagnosis and recommended treatment to achieve reduced morbidity and mortality.
Case Report
A 78-year-old male presented to the emergency department in diabetic ketoacidosis and sepsis secondary to cellulitis surrounding a large and intact oval-shaped necrotic plaque on the left lower extremity. Pertinent past medical history included uncontrolled type 2 diabetes (HbA1c level of 16.5%), peripheral neuropathy, and peripheral arterial disease. The patient was stabilized, and a podiatrist was consulted for evaluation and management of the ulceration and infection of the left lower extremity. The patient could not recall information regarding the onset of the lesion. He denied pain, malodor, and drainage, but he confirmed loss of protective sensation in his feet.
Physical examination revealed an oval-shaped necrotic eschar measuring 8.3 cm × 6.1 cm on the left lower extremity. The eschar was unstable and fluctuant underneath, with surrounding erythema extending 5.0 cm beyond the border of the lesion (Figure 1A). Pedal pulses were faint on palpation. Toe pressure of the left hallux was 60 mm Hg, with a toe-brachial index of 0.56.

Abnormal laboratory findings included elevated glucose of 881 mg/dL, C-reactive protein level of 22.4 µg/mL, lactate of 50.4 mg/dL, β-hydroxybutyrate of 7.78 mg/dL, troponin I of 0.735 ng/mL, and erythrocyte sedimentation rate of 54 mm per hour. MRI showed non-enhancing soft tissue around the ulcer, which was indicative of soft tissue necrosis. There was no evidence of osteomyelitis or gas gangrene on a preoperative radiograph or MRI.
Owing to the severity of infection, the patient was immediately consented and taken to the operating room for emergent incision and drainage for infection control. A tourniquet was not applied to the lower extremity for the procedure.
During the initial procedure, it was noted that devitalized tissues extended from skin down to the level of the fascia, with minimal bleeding. All nonviable tissue was removed, and a deep tissue sample was obtained for culture. The eschar, which measured 8.3 cm × 6.1 cm × 0.3 cm, was excised; thick, dark serosanguineous exudate was evacuated; and the surgical site was irrigated using 3 L of normal saline. The site was packed open with 5 mL of resorbable synthetic calcium sulfate beads (OsteoSet; Stryker) mixed with 1 g of vancomycin powder hardened in a designated tray for 30 minutes and placed against the fascia of the left lower extremity (Figure 1B). The intraoperative deep tissue cultures were positive for Enterobacter aerogenes and E faecalis. An infectious diseases specialist tailored the antibiotics with amoxicillin-clavulanate 875/125 mg and ciprofloxacin 500 mg, both of which the patient received twice daily.
Repeat surgical debridement was performed 2 days later. Necrotic wound margins and widespread necrosis of the fascia, muscle, and tendon were present. In addition, grey discoloration to the exposed tibia was observed. All nonviable soft tissues were removed and sent for histopathologic analysis. After surgical control of the bacterial infection was achieved and concurrent antibiotic therapy administered, a vascular surgeon was consulted to address the compromised blood supply to the left lower extremity. Subsequently, the patient underwent left posterior tibial artery and tibioperoneal trunk angioplasty.
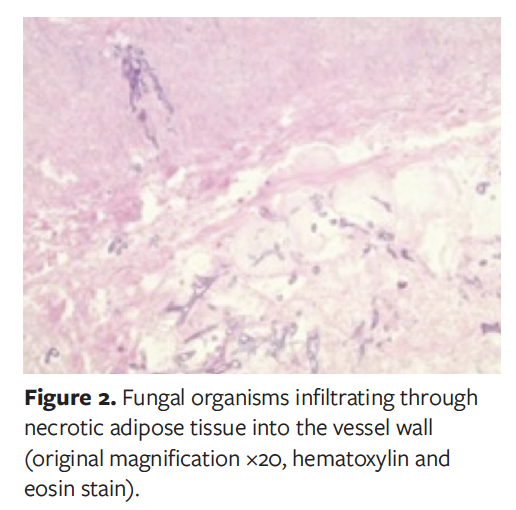
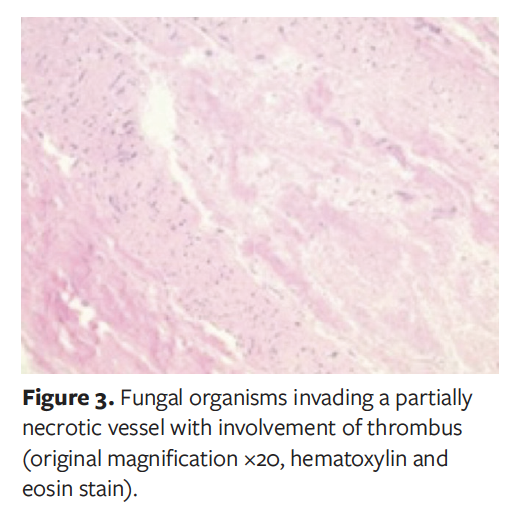
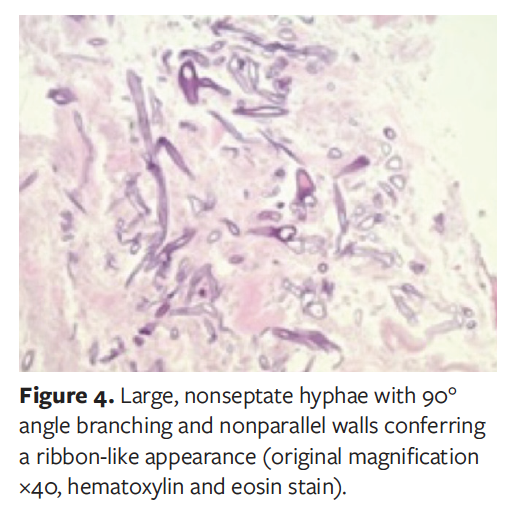
Morphologic and clinical features of the tissue sent for histologic analysis from the second procedure were suggestive of infection caused by cutaneous mucormycosis (Figures 2-4). The infectious disease specialist recommended transitioning to parenteral piperacillin/tazobactam 3.375 g every 8 hours and amphotericin B cholesteryl sulfate 25 mg per day. In addition, below-knee amputation was advised as a lifesaving measure. The patient refused this procedure along with all other medical treatments, left the hospital against medical advice, and did not return for further outpatient care.
Discussion
Mucormycosis is a rare, highly aggressive fungal infection that can affect the rhino-orbital-cerebral, pulmonary, gastrointestinal, and cutaneous systems.2 A literature review of English-language articles on zygomycosis identified 929 eligible cases for study, and the most common types of infection in these cases were sinus (359 patients [39%]), pulmonary (224 patients [24%]), and cutaneous (176 [19%]).7 In the cutaneous group, 43 of 176 infections (24%) were complicated by deep extension to tendon, muscle, or bone. In total, 20% of cutaneous infections had hematogenous dissemination (35/176), resulting in death in 94% of those patients (33/35).7
Cutaneous mucormycosis can present as either a primary source of infection, resulting from direct inoculation, or as a secondary manifestation of infection elsewhere. The upper and lower extremities are the most common anatomic areas affected.4,6,8
Risk factors for mucormycosis include trauma, which typically occurs in younger patients involved in motor vehicle accidents; intravenous drug use; preterm birth; bone marrow transplantation; deferoxamine treatment; an immunocompromised site; and diabetes.2,6 In patients with major primary risk factors, the inability of immune cells to mount a rapid and aggressive response to invasion of fungal spores leads to the accelerated course of this infectious organism.
Clinical presentation of primary cutaneous mucormycosis can vary. Lesions often start out as indurated, erythematous to purple plaques that become necrotic, with surrounding erythema.4,6,8,9 Extension to deep tissue layers may occur after the onset of necrotic ulceration.5,8 This type of lesion and continued tissue necrosis in the face of aggressive debridement warrants consideration of cutaneous mucormycosis in the differential diagnosis.8 Specimens should be obtained for fungal culture and sensitivity as well as histologic analysis.6 Sabouraud dextrose agar and potato dextrose agar are the media recommended for fungal cultures; media with antibiotics that can inhibit fungus growth should be avoided.1,4,6 Histologic examination also plays a vital role in confirming the diagnosis.1,4-6,8 Pathologic features of mucormycosis on histologic analysis include thrombosis, infarction, and inflammatory reaction that show polymorphonuclear cells, plasma cells, and eosinophils. Evidence of angioinvasion may be present as well, as indicated by thick, hyaline, nonseptated, bifurcated fungal hyphae within the blood vessels supplying the area of necrosis.2,4-6,9 Because of invasion of the dermal blood vessels, it is recommended that tissue samples down to the level of subcutaneous fat be taken from the center of the lesion.8 Newer molecular tests that target 18S ribosomal DNA can assist in precise identification of the infecting fungal organism; however, these tests can be costly and do not alter the recommended treatment plan for primary cutaneous mucormycosis.4-6,9
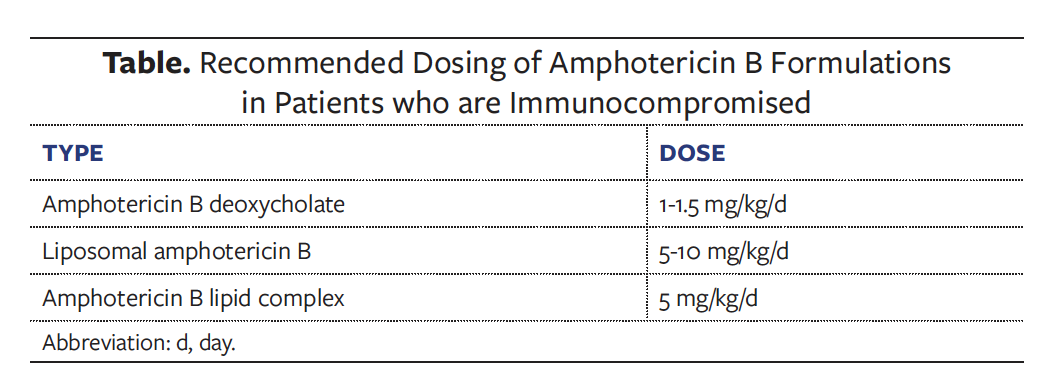
Early and aggressive debridement to prevent spread to deeper tissues and organs, concurrent antifungal therapy, and medical management of comorbid conditions are paramount in the management of primary cutaneous mucormycosis.1,3,5-8 Such treatment has been reported to reduce mortality rates from between 31% to 94% down to less than 10%.2 Early and aggressive debridement is particularly important in patients with diabetes. The preferred choice of antifungal is high-dose amphotericin B. However, its use can be complicated owing to the potential for nephrotoxicity, liver function impairment, and arrhythmia.6,8 Lipid formulation of amphotericin B is recommended owing to its better safety profile compared with other types of formulation. Recommended doses for the various formulations of amphotericin B are listed in the Table. Use of oral posaconazole 400 mg twice daily is another option that has been found to be beneficial in patients who are refractory or intolerant to amphotericin B or who require prolonged treatment.6,8
Few case reports of lower extremity mucormycosis infection have been published in the literature. A meta-analysis published in 2021 identified less than 200 cases reported in the literature, 37 of which involved deep extension into the tissues.5 A published case similar to the case presented herein involved cutaneous mucormycosis of the right lower extremity in a 73-year-old man who was immunocompromised and on regular prednisolone and azathioprine owing to a history of renal transplant.2 The initial clinical presentation and treatment were similar in that the patient discussed in Suthananthan et al2 had 2 ulcers requiring serial surgical debridement for continuous deterioration of the wound base with necrosis and affected periwound margins. The patient in that case report also had peripheral arterial disease on admission. Thus, treatment included right external iliac artery endarterectomy and liposomal amphotericin B 5 mg/kg per day after identification of fungal hyphae within blood vessels on histologic analysis. Despite the efforts of the health care team, 5 days after undergoing surgical debridement that patient died from multiorgan failure as a sequela of his disease.
Limitations
The limitation to this case study is that it was a single case, and the patient was lost to follow-up after identification and initiation of treatment for a rare and severe infection. More similar cases reported along with long-term follow up will provide insights for the development of treatment algorithms.
Conclusions
Health care providers must be aware of and possess a high index of suspicion for cutaneous mucormycosis when treating patients who are immunocompromised with necrotic wounds that exhibit continued rapid tissue destruction despite aggressive initial surgical debridement. In addition, histologic and microbiological analysis of tissue samples are essential for identifying the etiology of infection. Angioinvasion and acute thrombosis of blood vessels supplying the necrotic area are pathologic and clinical features of mucormycosis. Early and aggressive surgical debridement combined with parenteral amphotericin B are essential limb-saving and lifesaving measures to improve outcomes in patients with this rapidly progressive and potentially fatal condition.
Acknowledgments
Authors: Nicholas Chang, DPM1; James McKee, DPM2; Valerie Marmolejo, DPM3; and Arnold Paul C. Cua, MD2
Affiliations: 1Puget Sound Health Care System, Seattle, WA; 2MultiCare Auburn Medical Center, Auburn, WA; 3Scriptum Medica, DuPont, WA
Disclosure: The authors disclose no financial or other conflicts of interest.
Correspondence: Nicholas Chang, DPM; Puget Sound Health Care System, 1660 S Columbian Way Attn: S-112-Pod, Seattle, WA 98108; Nicholas.Chang0721@gmail.com
References
1. Stasiak M, Samet A, Lasek J, et al. Mucormycosis complicating lower limb crash injury in a multiple traumatised patient: an unusual case. BMJ Case Rep. 2009;2009:bcr10.2008.1170. doi:10.1136/bcr.10.2008.1170
2. Suthananthan AE, Koek SA, Sieunarine K. Cutaneous mucormycosis in an immunocompromised patient: a case report. J Surg Case Rep. 2017;2017(3):rjx056. doi:10.1093/jscr/rjx056
3. Wang Y, Zhu M, Bao Y, et al. Cutaneous mucormycosis caused by Rhizopus microsporus in an immunocompetent patient: a case report and review of literature. Medicine (Baltimore). 2018;97(25):e11141. doi:10.1097/MD.0000000000011141
4. Jia QY, Song YG, Li XQ, Mu ZL, Li RY, Li HM. Simultaneous infection of the skin surface and dermal tissue with two different fungus mimicking pyoderma gangrenosum: a case report. Clin Cosmet Investig Dermatol. 2021;14:163-167. doi:10.2147/CCID.S286582
5. Coerdt KM, Zolper EG, Starr AG, Fan KL, Attinger CE, Evans KK. Cutaneous mucormycosis of the lower extremity leading amputation in two diabetic patients. Arch Plast Surg. 2021;48(2):231-236. doi:10.5999/aps.2020.00549
6. Castrejón-Pérez AD, Welsh EC, Miranda I, Ocampo-Candiani J, Welsh O. Cutaneous mucormycosis. An Bras Dermatol. 2017;92(3):304-311. doi:10.1590/abd1806-4841.20176614
7. Roden MM, Zaoutis TE, Buchanan WL, et al. Epidemiology and outcome of zygomycosis: a review of 929 reported cases. Clin Infect Dis. 2005;41(5):634-653. doi:10.1086/432579
8. Skiada A, Petrikkos G. Cutaneous zygomycosis. Clin Microbiol Infect. 2009;15(S5):41-45. doi:10.1111/j.1469-0691.2009.02979.x
9. Antonov NK, Tang R, Grossman ME. Utility of touch preparation for rapid diagnosis of cutaneous mucormycosis. JAAD Case Rep. 2015;1(4):175-177. doi:10.1016/j.jdcr.2015.04.006






