



Synergistic Clinical Application of Synthetic Electrospun Fiber Wound Matrix in the Management of a Complex Traumatic Wound: Degloving Left Groin and Thigh Auger Injury
© 2024 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Wounds or HMP Global, their employees, and affiliates.
Abstract
Background. Managing complex traumatic soft tissue wounds involving a large surface area while attempting to optimize healing, avoid infection, and promote favorable cosmetic outcomes is challenging. Regenerative materials such as ECMs are typically used in wound care to enhance the wound healing response and proliferative phase of tissue formation. Case Report. The case reported herein is an example of the efficacious use of an SEFM in the surgical management of a large complex traumatic wound involving the left lower extremity and lower abdominal region. The wound bed was successfully prepared for skin grafting over an area of 1200 cm2, making this among the largest applications of the SEFM reported in the literature. Conclusion. This case report demonstrates the clinical versatility of the SEFM and a synergistic approach to complex traumatic wound care. The SEFM was successfully used to achieve tissue granulation for a successful skin graft across a large surface in an anatomic region with complex topography.
Abbreviations
Abbreviations: ECM, extracellular matrix; HD, hospital day; HOCl, hypochlorous acid; NPWT, negative pressure wound therapy; POD, postoperative day; SEFM, synthetic electrospun fiber matrix; STSG, split-thickness skin graft.
Introduction
Complex cutaneous wounds involving a large surface area and varying depths are particularly challenging to manage and require initiation of wound care that optimizes healing, avoids infectious compromise, and promotes favorable cosmetic outcomes. Multiple wound care modalities are used in the management of traumatic wounds, including wet-to-dry dressings, NPWT, ECMs, and skin grafting.1
Wound healing is a dynamic and intricate cascade of events that serves to maintain homeostasis within the wound bed, promote granulation and tissue remodeling, and avoid infection while regenerating the dermal matrix. The 4 phases of general wound healing include hemostasis, inflammation, proliferation, and remodeling.2 Collagen and elastin are 2 of the most vital proteins comprising human ECM and provide tissue integrity and granular tissue generation within wound beds during the proliferation phase, leading to eventual neovascularization and epithelialization.2,3
Regenerative matrix materials are routinely used to mimic native tissue architecture and modulate the wound healing cascade and proliferation phase. These regenerative matrices are largely divided into 3 classes of materials: synthetic (eg, poly[lactic-co-glycolic acids], polyurethane, hyaluronic acid), allograft (harvested human donor tissue or cadaveric tissue), and xenograft (harvested animal tissue) materials.4,5 The SEFM used in the current case report (Restrata; Acera Surgical, Inc.) is a fully resorbable biocompatible, porous matrix stated to provide a moist environment for natural healing processes to occur.6 Additionally, as a synthetic, the SEFM has demonstrated the ability to resist enzymatic degradation and persist in complex wounds.4
The matrix is composed of 2 resorbable polymers that have been electrospun to resemble native human ECM.4 This engineered structure encourages cellular migration and differentiation, and subsequent neovascularization.4 The SEFM contains varying fiber sizes, which elicit different and complementary regenerative responses.4 At initial application, the fiber and pore sizes of the SEFM are best suited to support fibroblast ingrowth and retention.4 As the SEFM resorbs into the wound bed via hydrolysis, the porosity of the matrix increases, supporting additional tissue ingrowth and regeneration.4 As a synthetic material, it provides more enzymatic resistance compared with biologic materials, and therefore is well suited for traumatic wounds.4 Adequate evidence in the literature shows that the SEFM is safe and effective in the management of wounds such as diabetic foot ulcers, chronic lower extremity wounds, traumatic injuries, and surgical wounds.7-11
The current case study demonstrates the use of the SEFM in the surgical management of a large complex traumatic wound involving the left groin, lower abdominal region, and lower extremity. By mimicking the structure and architecture of human ECM, the novel SEFM provided a scaffold for cellular infiltration and subsequent granulation tissue formation. The synthetic nature of the SEFM facilitated resistance to enzymatic degradation and exhibited the ability to remain within the complex wound beds for extended periods of time, thereby supporting wound healing.9-12
Multiple sheets of the SEFM meshed at 3:1 were hydrated and applied to the wound bed in 2 different surgical interventions. During this time, a modified NPWT dressing was applied and covered with a lipidiocolloid dressing in conjunction with the SEFM. Weeks later, the patient underwent STSG, and 100% STSG take was eventually achieved.
Case Report
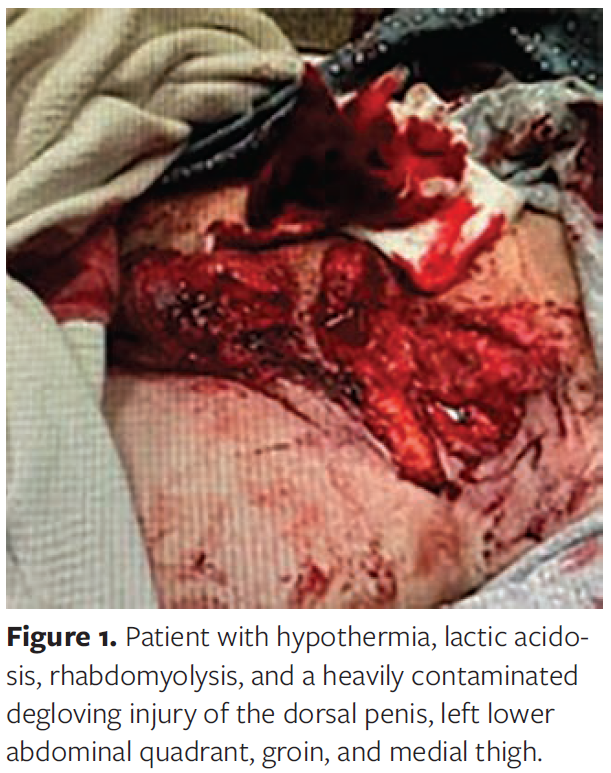
A 43-year-old male with a past medical history remarkable only for hypertension presented to the emergency department after his bilateral lower extremities became caught in an auger, requiring prolonged disentanglement. Upon arrival, the patient was alert and awake. Vital signs taken in the emergency department showed a systolic blood pressure of 132 and diastolic blood pressure of 71 mm Hg, heart rate of 89 beats per minute, body temperature of 94°F, and oxygen saturation of 100%. The patient was hypothermic, with lactic acidosis and rhabdomyolysis, closed left femoral shaft fracture, closed left distal tibial fracture, open Gustilo-Anderson type III fracture of the distal right tibia, and a closed left third finger fracture. Additionally, the patient had an extensive wound to the left lower extremity and left lower abdominal area. The wound measured 20 cm × 30 cm × 6 cm; in addition, he had a 10-cm × 10-cm × 1-cm scrotal laceration that extended to the base of the penis. There was extensive bruising across the glans and shaft of the penis as well (Figure 1).
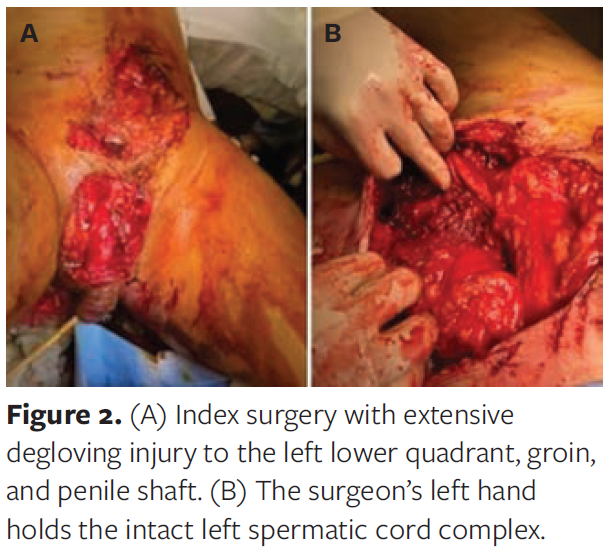
Tourniquets were placed and tranexamic acid was administered. The preliminary laboratory values included a white blood cell count of 35.7 x 109/L, hemoglobin level of 14.2 g/dL, lactic acid of 7.2 mmol/L, and creatine kinase level of 788 u/L. Due to developing respiratory distress the patient was intubated in the trauma bay, fluid resuscitation was initiated, and the patient was immediately taken to the operating room for exploration (Figure 2).
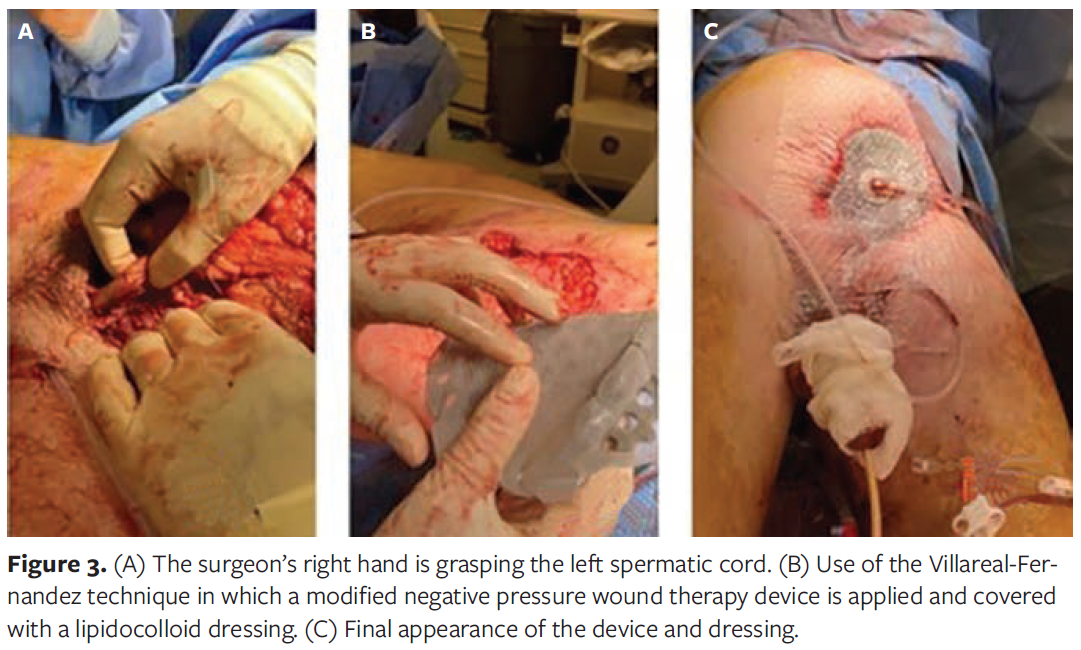
During the index surgery, irrigation of all open wounds was performed. The multiple areas of skin necrosis were sharply debrided. In addition, plastic reconstruction of the scrotum and penile shaft was completed, using 3-0 Vicryl suture (Ethicon). An NPWT device (V.A.C. Veraflo Cleanse Choice; 3M) and dressing was applied. The Villareal-Fernandez technique was used, in which a modified NPWT dressing was covered with a lipidocolloid dressing (UrgoTul; Urgo Medical North America), to protect the spermatic cord and other exposed vascular structures in the left femoral canal (Figure 3). An orthopedic surgeon performed bilateral external fixation of the tibial and fibular fractures and stabilization of the closed left femoral fracture.
Postoperatively, the patient was extubated and remained hemodynamically stable. Over the following days, the patient continued to undergo surgery for his orthopedic injuries, with the final surgery completed on POD 6.
On POD 7, the patient underwent surgical reexploration and debridement of the complex groin wound. Copious irrigation with HOCl (Vashe Wound Solution; Urgo Medical North America) was completed, and the spermatic cord was identified with good left spermatic artery vascular flow, as demonstrated by triphasic Doppler signals.
The NPWT dressing was replaced, and total parenteral nutrition was initiated. The patient underwent 6 additional surgical procedures and washouts via a wound debridement system (Pulsavac Plus AC; Zimmer Biomet), with 0.9% normal saline and HOCl irrigation, debridement of nonviable soft tissues, and replacement of NPWT.
On HD 22 from the index procedure, the complex wound was washed out and measured 1200 cm2, covering 5.4% of the patient's total body surface area as calculated using the Mosteller formula:
Diffuse granulation tissue was present, and the wound appeared clean without obvious signs of infection, purulence, active bleeding, or injury to anatomic structures. At that time, the decision was made to use the SEFM to promote granulation tissue and enhance wound healing prior to skin grafting (Figure 4).
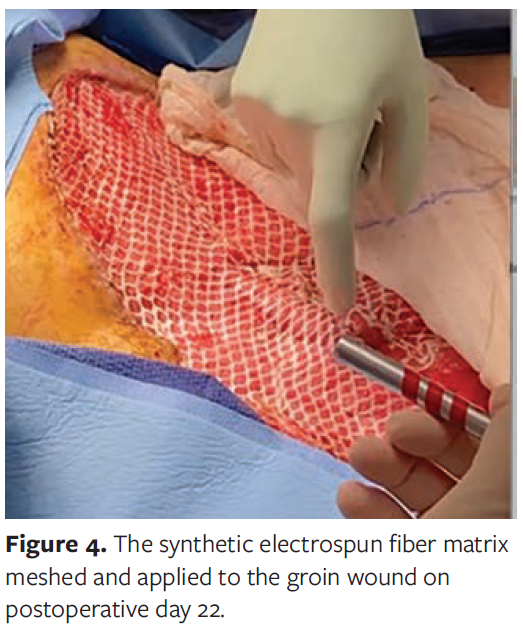
Two pieces of 4-cm × 5-cm SEFM and 1 piece of 1.5-cm × 7.5-cm SEFM were meshed while dry, then soaked in saline solution for 2 to 5 minutes and anchored within the wound bed using 4-0 absorbable interrupted sutures. Cut, hydrated strips of the SEFM were also placed within tunneling wounds noted on the medial left thigh near the Hunter canal. A lipidocolloid wound dressing was then placed atop the SEFM, and NPWT was initiated.
On HD 27 the wound was inspected, and healthy pink granulation tissue was noted throughout the wound bed, including the tunneling area near the Hunter canal. The wound was further irrigated with HOCl solution, and a new layer of SEFM was placed comprising 7.5-cm × 7.5-cm and 5-cm × 5-cm sheets that were meshed, hydrated, applied in full contact with the wound bed, and anchored with absorbable sutures. Morcellized pieces of the SEFM cut from full sheets were also hydrated and applied into the medial tunneling area, and an NPWT dressing was applied. Postoperatively, the patient continued to progress and was transferred out of the intensive care unit.
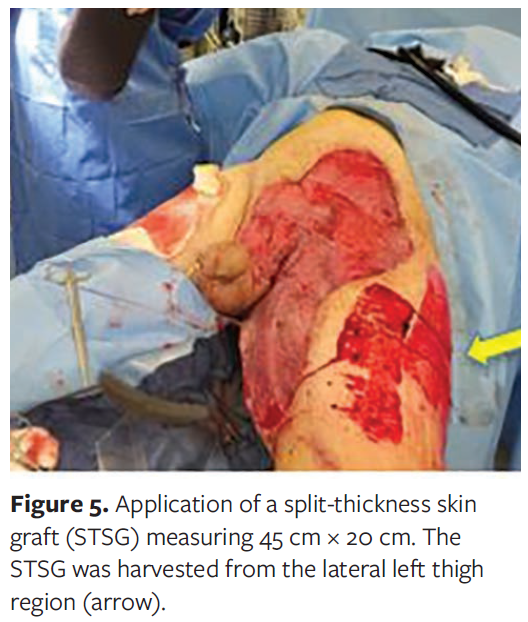
On HD 34, 12 days following application of the SEFM, the patient returned to the operating room for further debridement, irrigation, and application of an STSG measuring 45 cm × 20 cm. The STSG was harvested at 0.01-inch thickness, meshed at 1:1.5, and placed onto the wound bed while sparing the genitalia to prevent contracture in the region. The graft was secured to the wound bed with stainless steel staples, and an NPWT dressing was applied (Figure 5).
On HD 38 the NPWT dressing was removed, revealing greater than 95% take of the STSG to the underlying wound bed 4 days after application. At that time, the staples were removed, and the wound was dressed with an impregnated xeroform and petrolatum dressing and 4-cm × 4-cm sterile gauze (Figure 6).

The wound was subsequently re-dressed daily. The patient continued to improve and was discharged on HD 44 from the index surgery on prophylactic oral trimethoprim-sulfamethoxazole twice daily for 5 days. Excellent graft take was observed at discharge (10 days following STSG application) (Figure 7). Following discharge, the patient required several minor outpatient drainage procedures for a small seroma near the medial aspect of the wound. He was briefly readmitted for 24 hours of observation and subsequently discharged.

Three weeks after initial discharge, the patient was seen in the plastic surgery clinic with complete healing both of the donor site and the left-sided complex wound; this occurred 65 days after the index procedure, and 43 days after initial application of the SEFM (Figure 8). The patient was actively participating in physical therapy, and his pain was well controlled. No additional surgical procedures were required.

Discussion
Enhancing the wound healing process, especially in large complex traumatic wounds, is essential for achieving optimal outcomes. The use of regenerative matrices can be advantageous in optimizing wound healing.2,9-16 Specifically, in the current case the 3-dimensional SEFM was successfully used to encourage granulation tissue formation across a large complex wound bed in preparation for definitive closure via STSG.
Other large surface area wounds have been successfully treated with SEFM. Rodriguez et al12 described the case of a 7-year-old girl who sustained second-degree burns of the left shoulder, upper chest, and back, comprising approximately 6% total body surface area. Wound care comprised multiple surgical irrigations, debridements, and applications of the SEFM. Over the next 5 weeks, the SEFM was surgically replaced once and then allowed to slowly incorporate into the underlying wound bed without removal or need for skin grafting. Nearly complete wound healing was observed at 5-week follow-up, in addition to excellent return of skin pigmentation and no observed contracture.
It is important to remember that wound reconstruction involves not only subcutaneous tissues, but often other vital structures, including vessels, nerves, tendons, bone, and even spermatic cord, as noted in the current report. Bohn and Chaffin13 explained that although dermal matrices do not replace the reconstructive flap procedures required for deep tissue defects involving exposed underlying structure, they do provide a range of alternate therapies for patients unable or unwilling to undergo flap reconstruction. They successfully reconstructed 6 soft tissue defects with exposed structures using ovine-derived ECM grafts, achieving successful wound granulation and epithelialization for later skin graft and cosmetic interventions.
The engineered design and synthetic composition of the SEFM stimulates tissue regeneration with resistance to premature degradation, offering critical clinical benefits in the management of complex traumatic wounds.4,8,9 Traumatic wounds tend to be large and are often contaminated.15 This risk can be mitigated with thorough wound cleansing and debridement.16 In the current case, irrigation with HOCl was used, which has been shown to inhibit microbial contamination by decreasing the pH of the wound.17 The SEFM used in the current case may also elicit this effect as it degrades, as has been previously reported.4 Bioresorbable polymers, of which the novel SEFM is composed, have a demonstrated mildly acidic effect as they degrade.4 This effect is beneficial to wound healing, because acidic environments are more resistant to bacterial growth.4 Infection is a leading cause of delayed healing and may result in increased morbidity and mortality; thus, wound management therapies designed to mitigate the risk of infection both intraoperatively and during postoperative wound care are vital to successful healing outcomes.18,19 The SEFM used in the current case contains no additives or biologic materials, which limits the risk of chronic inflammatory response that can be elicited from collagen-based materials.4 By facilitating infection control, encouraging autologous cellular infiltration, and promoting formation of granulation tissue, the SEFM may be a valuable adjunct in successful healing and resolution of complex traumatic wounds.4,9,10
Limitations
The current study is limited in that it is a single case report with neither additional use cases nor a control group. The results of the study may not be optimal in generalizing the validity of the study or in establishing a cause-and-effect relationship. Due to its retrospective nature and focus on a rare case, the current study may suffer from selection biases. However, this report carefully illustrates the feasibility and effective clinical application of the SEFM in the management of a complex traumatic wound, which may be of benefit to surgeons faced with similar circumstances.
Conclusion
The current case report demonstrates the novel SEFM's durability and clinical versatility as an attractive therapeutic option for the management of large complex traumatic wounds.10-13 This case further illustrates the effectiveness of the SEFM as an adjunct to skin grafting for definitive wound closure. The matrix successfully promoted granulation tissue and adequate skin graft take in a complex, contaminated, large wound covering approximately 5.4% of the patient's total body surface area at the time of initial application. This wound was ragged and infection-prone, both suboptimal conditions for healing. Use of the SEFM to prepare a complex wound bed for skin grafting over an area of 1200 cm2 was effective for this patient.
To the knowledge of the authors of the current report, with the exception of Rodriguez et al,12 the current case is among the largest, most successful applications of the SEFM reported in the literature to date, adding to the growing body of clinical evidence of SEFM use following traumatic soft tissue damage. Individual clinical outcomes have been extensively documented; however, a review of published data in this field or a large clinical study could be beneficial to potentially further confirm outcomes and establish evidence-based SEFM treatment protocols.
Acknowledgments
Authors: Luis G. Fernandez, MD1-3; Carolina Orsi, MD4; Brandon Okeoke, MS5; Paige Moudy, DO4; Paul A. Critelli, MD6; Scott Norwood, MD7-8; Marc R. Matthews, MD9; Paul J. Kim, DPM, MS10; Matthew MacEwan, PhD11; and Emily Sallade, BS11
Affiliations:1Dept. of Surgery, Division of Trauma Surgery/Surgical Critical Care, University of Texas Health Science Center, UT Health East Texas, The University of Texas SOM, Tyler, Texas; 2The University of Texas-Tyler School of Medicine Bill Barrett Endowed Chair in Trauma Surgery, Tyler, Texas; 3Trauma Wound Care, UT Health East, Tyler, Texas; ⁴Dept. of Surgery, University of Texas Health Science Center, UT Health East Texas, Tyler, Texas; ⁵School of Medicine, The University of Texas Medical Branch, Galveston, Texas; ⁶University of Texas Health Science Center, UT Health East Texas, The University of Texas SOM, Tyler, Texas; ⁷Dept. of Surgery, The University of Texas Health Science Center, Tyler, Texas; ⁸Trauma Services, The University of Texas Health – Tyler, Tyler, Texas; ⁹Division of Trauma, Surgical Critical Care, Burns, and Acute Care Surgery, Banner University of Arizona/University Medical Center, Tucson, Arizona; 10Dept. of Plastic Surgery, Dept. of Orthopedic Surgery, University of Texas Southwestern, Dallas, Texas; 11Acera Surgical, Inc., St. Louis, MO
Disclosure: Dr Fernandez is a paid consultant for Acera Surgical, Inc. Dr MacEwan and Ms Sallade are employees of and have stock options held in Acera Surgical, Inc. Financial support in the form of consultant fees was provided for time spent on data collection for manuscript drafting.
Correspondence: Luis G. Fernandez, MD; UT Health East Texas Physicians Tyler, Department of Surgery, 6801 Hollytree Circle, Tyler, TX 75703; thebigkahuna115@gmail.com
Manuscript Accepted: February 27, 2024
References
1. Singh M, Nuutila K, Kruse C, Robson MC, Caterson E, Eriksson E. Challenging the conventional therapy: Emerging skin graft techniques for wound healing. Plast Reconstr Surg. 2015;136(4):524e-530e. doi:10.1097/PRS.0000000000001634
2. Diller RB, Tabor AJ. The role of the extracellular matrix (ECM) in wound healing: a review. Biomimetics (Basel). 2022;7(3):87. doi:10.3390/biomimetics7030087
3. Häkkinen L, Larjava H, Koivisto L. Granulation tissue formation and remodeling. In: Oral Wound Healing. Endodontic Topics. 2013:94-129. doi:10.1002/9781118704509.ch6
4. MacEwan M, Jeng L, Kovács T, Sallade E. Clinical application of bioresorbable, synthetic, electrospun matrix in wound healing. Bioengineering (Basel). 2022;10(1):9. doi:10.3390/bioengineering10010009
5. Mouw JK, Ou G, Weaver VM. Extracellular matrix assembly: a multiscale reconstruction. Nat Rev Mol Cell Biol. 2014; 15(12):771-785. doi:10.1038/nrm3902
6. Restrata. Acera Surgical Inc. Accessed May 29, 2023.
7. Regulski MJ. Clinical evaluation of a novel nanofiber wound matrix for the treatment of chronic lower extremity wounds. J Dermatol Ther. 2018;2(1):35-38.
8. Martini CJ, Burgess B, Ghodasra JH. Treatment of traumatic crush injury using a synthetic hybrid-scale fiber matrix in conjunction with split-thickness skin graft. Foot Ankle Surg (N Y). 2022;2(1):1001122. doi:10.1016/j.fastrc.2021.100112
9. Fernandez L, Shar A, Matthews M, et al. Synthetic hybrid-scale fiber matrix in the trauma and acute care surgical practice. Wounds. 2021;33(9):237-244.
10. Fernandez LG, Matthews MR, Kim PJ. A synthetic hybrid-scale fiber matrix for complex surgical wounds: consensus guidelines. Wounds. 2023;35(5): E160-E168. doi:10.25270/wnds/22067
11. Herron K. Treatment of a complex pressure ulcer using a synthetic hybrid-scale fiber matrix. Cureus. 2021;13(4)e14515. doi:10.7759/cureus.14515
12. Rodriguez JC, Chen AH, Carney DE. Treatment of superficial second-degree burns with a nanofiber tissue matrix: a case report. Burns Open. 2022;6(4):173-176. doi:10.1016/j.burnso.2022.09.002
13. Bohn GA, Chaffin AE. Extracellular matrix graft for reconstruction over exposed structures: a pilot case series. J Wound Care. 2020;2(29):742-749. doi:10.12968/jowc.2020.29.12.742
14. Kalva SN, Augustine R, AL Mamun A, Dalvi YB, Vijay N, Hasan A. Active agents loaded extracellular matrix mimetic electrospun membranes for wound healing applications. J Drug Deliv Sci Technol. 2021;63:102500. doi:10.1016/j.jddst.2021.102500
15. Bhartiya SK, Prasad R, Sharma S, Shukla V, Nath G, Kumar R. Biological therapy on infected traumatic wounds: a case control study. Int J Low Extrem Wounds. 2022;15347346211072779. doi:10.1177/15347346211072779
16. Leaper DJ. Traumatic and surgical wounds. BMJ. 2006;332(7540):532-535. doi:10.1136/bmj.332.7540.532
17. Wang L, Bassiri M, Najafi R, et al. Hypochlorous acid as a potential would care agent: part I. Stabilized hypochlorous acid: a component of the inorganic armamentarium of innate immunity. J Burns Wounds. 2007;6:e5.
18. Bessa LJ, Fazii P, Di Giulioi M, Cellini L. Bacterial isolates from infected wounds and their antibiotic susceptibility pattern: some remarks about wound infection. Int Wound J. 2015;12(1):47-52. doi: 10.1111/iwj.12049
19.Zabaglo M, Sharman T. Postoperative wound infection. In: StatPearls [Internet]. StatPearls Publishing; 2023.






