



Flap Application in Reconstructive Surgery to Manage Severe Radiation-induced Ulcers: A Case Series
Abstract
Introduction. Radiation-induced ulceration is a late-stage skin reaction after RT for cancer treatment. Objective. The present study examined the use of a single-stage reconstructive procedure to manage radiation-related wounds. Materials and Methods. Nine patients with radiation-induced chronic ulcer with accompanying severe complications were admitted to the Plastic, Reconstructive, and Regenerative Center of Viet Nam National Burn Hospital between October 2015 and September 2019. The patients ranged in age from 49 to 77 years. Complications included exposed cheekbone (n = 1), exposed trachea (n = 1), exposed carotid artery (n = 2), exposed axillary artery (n = 2), exposed pleura (n = 1), and exposed pericardium (n = 2). Flap type used to achieve defect coverage after debridement was individualized to each patient and included ALT, LD, SCA, and DIEP flaps. Additionally, a high-density polyethylene was used to reconstruct the trachea to recover breathing function in the patient with exposed trachea. Results. Complete survival of all flaps was achieved. Most vital organs (the trachea, axillary artery, and carotid artery) were covered. Hospital length of stay ranged from 15 to 120 days. Conclusions. The successful management of patients with severe complications suggests that immediate single-stage reconstruction may be a valuable option for managing radiation-induced ulcers.
Abbreviations
ALT, anterolateral thigh; CT, computed tomography; DIEP, deep inferior epigastric artery perforator; LD, latissimus dorsi; PMM, pectoralis major muscle; RT, radiation therapy; SCA, superficial cervical artery; TRAM, transverse rectus abdominis musculocutaneous
Introduction
RT has a substantial impact on the treatment of cancer. It can cure some cancers in the early stages, and sometimes it is used to alleviate symptoms caused by cancer.1,2 However, RT-associated early and late side effects may affect various organs, such as the skin and mucosa, salivary glands, nervous system, thorax, lung, and heart.3 Skin injuries may be considered the most common of these undesired outcomes, with 95% of patients who receive RT sustaining such injuries.4 While acute radiation damage including mucositis, hypersensitivity, pain, and ulcer can be healed with appropriate management, some late complications, such as fibrosis and nonhealing ulcers, are often irreversible.4,5 More importantly, some nonhealing deep ulcers sometimes threaten vital organs. Inflammation, ischemia, and secondary wound infections could lead to poor quality of life.5 In severe cases, wide surgical debridement and reconstructive techniques have often been used to manage these ulcers.5,6 However, limited reports of complicated RT-induced ulcers in the literature have made it difficult for even the most skilled plastic surgeons to find the best treatment options for these cases.
This case series discusses 9 patients with severe RT-induced ulcers, including ulcer bases containing exposed cheekbone, exposed carotid artery, exposed axillary artery, exposed trachea, exposed pleura, and exposed pericardium. These wound types are not well represented in the literature. Additional treatments and surgical outcomes of these patients are also discussed. This study contributes to the current literature on the management of these rare cases.
Materials and Methods
Patients with RT-induced severe ulcers, including ulcer bases with exposed carotid artery, exposed trachea, exposed pleura, exposed pericardium, and exposed cheekbone, who presented to the Plastic, Reconstructive, and Regenerative Centre of the Viet Nam National Burn Hospital, Hanoi, Viet Nam, between October 2015 and September 2019, were recruited for this study. Surgical reconstruction was immediately required for all cases after meticulous physical examination. Appropriate surgical techniques were chosen based on the surgeons’ experience and the defect characteristics of the individual patients. Patients signed a consent form permitting use of their information for this publication.
Four male and 5 female patients with a mean age of 62 years (range, 49 years–77 years) were enrolled (Table). All the female patients had breast cancer. Ulcer-related complications included ulcer bases containing exposed cheekbone (n = 1), exposed trachea (n = 1), exposed carotid artery (n = 2), exposed axillary artery (n = 2), exposed pleura (n = 1), and exposed pericardium (n = 2).
Wound dimensions were also noted. Wide debridement was performed intraoperatively to provide a bleeding bed. Flaps such as ALT flap, skin flap, LD flap, SCA flap, and DIEP flap were created and transferred to achieve coverage of individual defects. Drainage was used in all patients and was removed 15 to 20 days postoperatively. Two or 3 types of antibiotics were used in each patient over the course of 2 to 3 weeks. CT and magnetic resonance imaging were performed when necessary to evaluate the extent of the defect.
Patients were followed up 2 years postoperatively in the outpatient clinic to assess for ulcer and cancer recurrence.
Results
All ulcers exhibited remarkable recovery postoperatively (Table). Hospital length of stay ranged from 15 to 120 days. Intraoperative hemorrhage occurred in only 1 patient, who had a damaged carotid artery owing to his deep ulcer. No other incidents occurred intraoperatively. Satisfactory aesthetic results were achieved with all flaps. No ulcer or tumor recurrences occurred within the follow-up period.
Case 1: Ulcer base containing exposed cheekbone
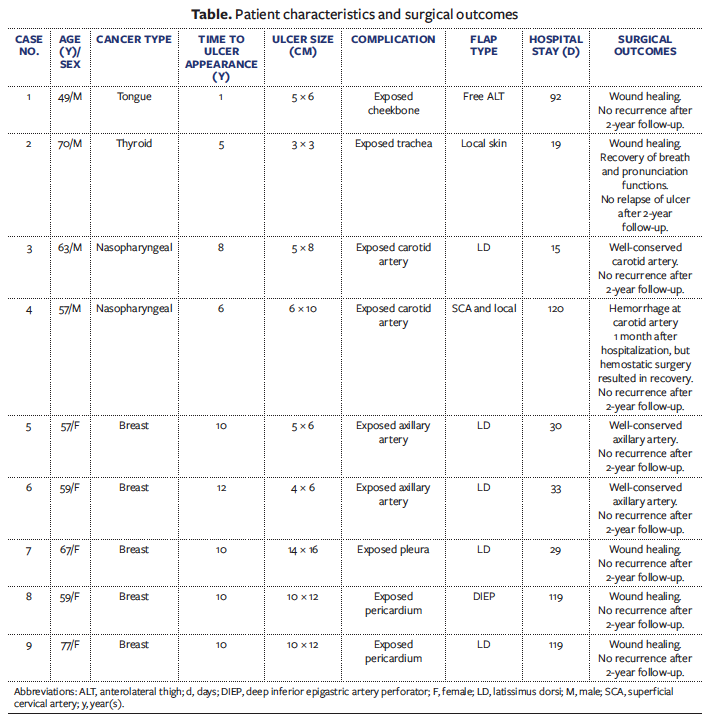
A 49-year-old male patient had a wide radiation-induced ulcer (5 cm × 6 cm) in the right cheek after 1 of year RT for tongue cancer. The cheekbone was exposed along with surrounding infiltrative tissues. Radical excision was performed, followed by partial excision of the necrotic and affected areas, design of an ALT flap, and flap elevation, after which the patient underwent immediate reconstruction with the ALT flap. The wound healed smoothly by 3 months postoperatively, with no ulcer recurrence (Figure 1).
Case 2: Ulcer base containing exposed trachea
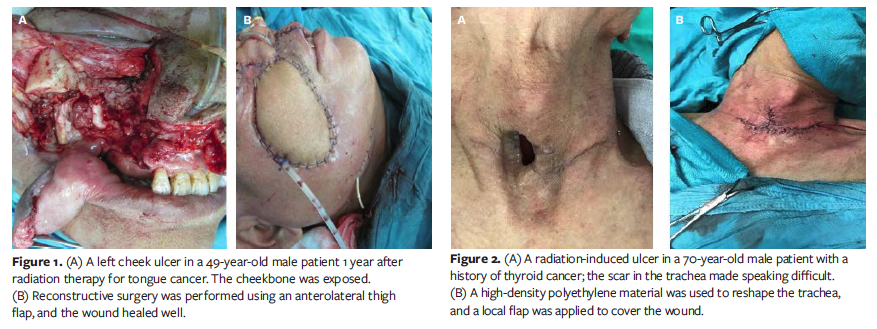
A 70-year-old male patient contracted thyroid cancer and developed an ulceration measuring 3 cm × 3 cm in the anterior neck with exposed trachea after 5 years of RT. The trachea was partially lost, resulting in a risk of infection and pneumonia because of the trachea leakage, and it had been invaded by cancer cells. Because of the risk of trachea collapse postoperatively with use of a skin flap alone, a high-density polyethylene (Medpor; Stryker) was used to cover the trachea defect before covering the ulcer with a local skin flap. After the lesion was removed, the trachea was reconstructed with the high-density polyethylene and the defect covered with a local skin flap (Figure 2). This patient recovered well, with normal breathing and pronunciation functions. The local wound healed. There was no ulcer recurrence.

Case 3: Ulcer base containing exposed carotid artery
A 63-year-old male patient with nasopharyngeal cancer had an ulcer measuring 5 cm × 8 cm on the left side of the neck as well as exposed carotid artery at the ulcer base after 8 years of RT. Many pseudomembranes were observed inside the lesions. Wound debridement resulted in a deep and wide infiltrative area that posed a threat to the carotid artery. Radical excision of the ulcerative site and surrounding infiltrative tissues was performed, followed by reconstruction with an LD flap (14 cm × 9 cm) (Figure 3A). The wound well healed with the conserved carotid artery.
Case 4: Complicated case of ulcer base containing exposed carotid artery
A 57-year-old male patient with nasopharyngeal cancer had an ulcer on the neck with exposed carotid artery at the ulcer base after 6 years of RT. This wound was severe, with a deep, hardening, wide lesion (6 cm × 10 cm) on the right neck. The carotid artery was slightly torn apart, showed caseation, and was hard to differentiate from surrounding tissues. The torn carotid artery wall was sewn using the nonabsorbable polypropylene interrupted X suture, after which SCA flap transfer was performed. Eight hours postoperatively, bleeding developed under the flap. The patient underwent a second surgery, in which ligature of the carotid artery was performed at the upper and lower margins of the ulcer. The patient was stable postoperatively, and the wound was washed and the bandage changed daily. Nevertheless, partial necrosis occurred in the transferred flap, resulting in a small lesion (2 cm × 3 cm × 2 cm). After 1 month, the wound bled again because of the extent of necrosis. Gauze was applied to the ulcer to temporarily stop the hemorrhage before hemostasis was obtained (Figure 3B). The artery was then covered with surrounding soft tissues. Necrosis and hemorrhage persisted 2 months postoperatively, during which time the patient remained hospitalized. It was necessary to sew the injury to stop the bleeding, after which the wound was covered with a local flap. The wound closed after this intervention.

Cases 5 and 6: Ulcer bases containing exposed axillary artery
A 57-year-old female patient and a 59-year-old female patient with breast cancer were hospitalized with ulcer bases containing exposed axillary artery. LD flaps were used to cover the defects (Figure 4). Lymphatic edema was also observed in case 6, and lymphovenous anastomosis was performed as well during the flap reconstruction surgery to recover her lymphatic system. Both patients recovered well postoperatively owing to the initial treatment. Preoperatively, they had difficulty with movement of the upper limbs. However, in both patients, postoperative range of motion of the glenohumeral joint was from 120° to 150° compared to a limited range of motion preoperatively, which was a significant improvement resulting from the treatment. The axillary artery was well conserved in both patients. No complications or incidents occurred intra- or postoperatively.

Cases 7, 8, and 9: Ulcer bases containing exposed pleura and pericardium
One female patient had an ulcer base containing exposed pleura (case 7), and 2 female patients had an ulcer base with exposed pericardium (cases 8 and 9). These 3 patients had the largest wounds among the 9 patients in this series. Necrosis of the rib was evident in cases 7 and 8. Additionally, an unclear margin between the wound and the pericardium on a CT scan in case 9 suggested a risk of pericardium damage.
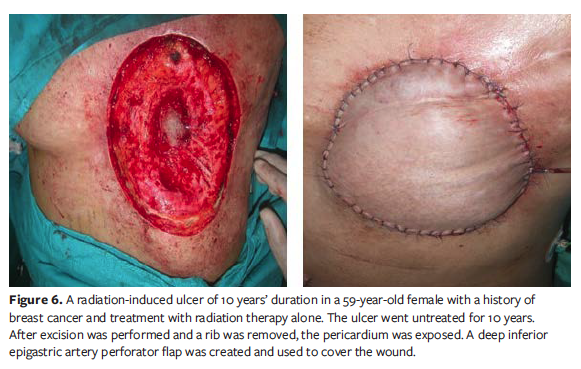
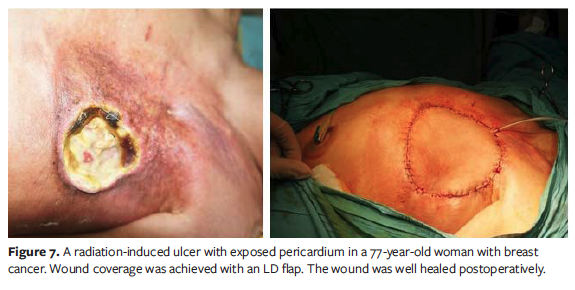
In the case with exposed pleura, the safety of the underlying vital organs and the process of wound healing were prioritized. An LD flap was used to cover the ulcer in case 7 (Figure 5). A DIEP flap was transferred to cover the defect in case 8 after wound debridement, and an LD flap was used for wound coverage in case 9 (Figures 6 and 7). All 3 patients recovered well without any visible damage, although both patients with exposed pericardium at the ulcer base required a prolonged hospital stay.
Discussion
Although RT has shown tremendous benefits for cancer treatment in recent decades, its side effects have been reported in many studies. Radiation-induced ulcers are a late-stage skin reaction after RT, and they have a considerable direct effect on patients’ lives.1 In a previous study, a moderate-to-severe skin reaction was seen in 85% of patients who underwent RT.7 It has been clearly documented that radiation-induced ulcers cannot be self-limited owing to the reduced blood supply in the surrounding tissue, fibrosis, and impaired cellular repair potential.2,3 Radiation-induced ulcers often become infected, reducing the viability of the granulation tissue.4,5 Therefore, the management of radiation-induced ulcers to reduce the complications of RT has emerged as a clinically important issue. As described in the literature, chronic radiation-induced ulcers can be managed with advanced treatments such as mesenchymal stem cells, hyperbaric oxygen therapy, superoxide dismutase, and low-intensity laser therapy.5,8 Additional study of some of these modalities is required, however. One study reported few benefits with hyperbaric oxygen therapy and conventional wound care.8 Another study also described the use of excision and reconstructive methods, such as pedicle flaps to increase blood supply and the usage of antibiotic for infection control.6 In addition, the authors of the present study performed partial and total excision to control the base of the ulcer. For less severe injuries, both the necrotic area and the entire affected area were completely excised, while partial excision was used for more severe ulcers because of the presence of highly vascular areas or because the wound lay over ribs. In the case that the base of the ulcer could not completely be controlled, often the drain tube was left in place for a longer time.
Surgical technique is selected based on the complications of RT and wound location. For example, microsurgical reconstruction is commonly used to manage RT-induced ulcers of the head and face.6 Historically, it has been challenging to use pedicle flaps for wound coverage at these sites. A TRAM flap or free LD flap is often used to cover large defects in the setting of advanced infection or in cases that require large flaps for coverage.6,9 These 2 flap types are large, however, and aesthetically they are not optimal for use on the face. Therefore, the authors of the present study used an ALT flap to cover the ulcer on the right cheek, which resulted in improved aesthetics postoperatively.
For a patient with partial loss of the trachea, rather than simply selecting a flap to cover the lesion without tracheal reconstruction, a surgical approach to cover the trachea should be considered owing to the risk of tracheal stenosis postoperatively. In the present case series, high-density polyethylene was efficacious in trachea reconstruction, which benefitted the surgical procedure and promoted the recovery of breathing function.
In general, the greatest challenge in the treatment of RT-induced ulcers, especially ulceration on the neck, is the devastation of the vascular system.10,11 Therefore, coverage of defects with pedicled flaps is prioritized because of the ability of such flaps to supply blood to the site. The current literature recommends the PMM flap, LD flap, SCA flap, and ALT flap in addition to microsurgical reconstruction to achieve coverage of RT-induced ulcers.
For ulcers of the neck, pedicled flaps such as the LD flap and PMM flap are used to cover defects.12 For cases 5 and 6 in the present series, the biggest challenge was the deep wounds with exposure of the underlying axillary artery, which had the potential to destroy the artery and cause hemorrhage postoperatively. However, the surgical results were promising, no hemorrhage occurred, and significant recovery occurred in both cases.
RT for breast cancer may cause deep ulcers and necrosis of the rib and sternum, leading to exposure of the pericardium and pleura. Therefore, chest wall reconstruction must prioritize the safety of the underlying organs, defect coverage, and wound healing. The skin flaps used in such cases include the DIEP, TRAM, vertical rectus abdominis myocutaneous, and LD flap. Of those, the LD flap is the most commonly used to manage RT-induced ulcers in the chest because such flaps contain a diverse large vascular system and do not cause disturbance at the donor site.13 LD and DIEP flaps were used in the present case series, and outcomes were promising. Thorough removal of infiltrative areas as well as injured areas of ribs and sternum is also required to ensure a clean lesion perioperatively. In these cases, it was also necessary to entirely remove unimportant tissues such as wide skin areas, bone, and cartilage until all injured areas were removed before starting the coverage procedure.
Limitations
One limitation of this study is that the reported cases were individuals with mostly varied patient characteristics, and flaps were used in each case. Thus, the authors of the present study could not identify and establish a general guideline for treating such severe ulcers. Another limitation is that all techniques used to manage RT-induced ulcers were reported in literature. However, this study highlighted the serious damages threatening the patients’ quality of life and recommended meticulous attention on the protection of vital organs when patients were treated with RT. In addition, the authors of this present report introduced their personal experience for types of flaps that produced satisfactory outcomes in terms of aesthetics and wound healing.
Conclusion
RT-induced severe ulcer is a dangerous complication that can negatively affect patients’ quality of life and poses challenges to surgeons owing to the difficulty of conserving anatomic structures intraoperatively. In this case series, additional flaps were suggested (different from those reported previously) that contributed to the successful surgical treatment of these cases. More importantly, this study emphasizes the importance of immediate single-stage reconstruction and the conservation of the surrounding damaged tissues caused by wide and deep ulceration in order to avoid undesirable events intraoperatively and the importance of selecting the appropriate surgical techniques to achieve ulcer coverage.
Acknowledgments
Authors: Hoang Thanh Tuan, MD, PhD1; Vu Quang Vinh, PhD1; Tran Van Anh, PhD1; Tong Thanh Hai, MD, MS1; Tran Quang Phu, MD, MS2; and Trinh Tuan Dung, PhD3
Affiliations: 1Plastic and Reconstructive Aesthetic Surgery Center, Viet Nam National Burn Hospital, Military Medical Institute, Hanoi, Vietnam; 2Adult Burns Department, Vietnam National Burn Hospital, Military Medical Institute, Hanoi, Vietnam; 3Anatomical Pathology Department, Tam Anh Hospital, Hanoi, Vietnam
Disclosure: The authors disclose no financial or other related conflicts of interest.
Correspondence: Hoang T. Tuan, MD, PhD, Plastic and Reconstructive Aesthetic Surgery Center, Viet Nam National Burn Hospital, Military Medical Institute, 160 Phung Hung, Phuc La, Ha Đong, Hanoi, Vietnam; tuanht.vb@gmail.com
References
1. Baskar R, Lee KA, Yeo R, Yeoh KW. Cancer and radiation therapy: current advances and future directions. Int J Med Sci. 2012;9(3):193-199. doi:10.7150/ijms.3635
2. Dilalla V, Chaput G, Williams T, Sultanem K. Radiotherapy side effects: integrating a survivorship clinical lens to better serve patients. Curr Oncol. 2020;27(2):107-112. doi:10.3747/co.27.6233
3. Majeed H, Gupta V. Adverse Effects Of Radiation Therapy. In: StatPearls. Treasure Island (FL): StatPearls Publishing; September 14, 2022.
4. Manna B, Cooper JS. Radiation Therapy Induced Skin Ulcer. In: StatPearls. Treasure Island (FL): StatPearls Publishing; August 10, 2022.
5. Iyer S, Balasubramanian D. Management of radiation wounds. Indian J Plast Surg. 2012;45(2):325-331. doi:10.4103/0970-0358.101311
6. Fujioka M. Surgical reconstruction of radiation injuries. Adv Wound Care (New Rochelle). 2014;3(1):25-37. doi:10.1089/wound.2012.0405
7. Salvo N, Barnes E, van Draanen J, et al. Prophylaxis and management of acute radiation-
induced skin reactions: a systematic review of the literature. Curr Oncol. 2010;17(4):94-112. doi:10.3747/co.v17i4.493
8. Wei J, Meng L, Hou X, et al. Radiation-induced skin reactions: mechanism and treatment.
Cancer Manag Res. 2018;11:167-177. doi:10.2147/CMAR.S188655
9. Jung JA, Kim YW, Kang SR. Reconstruction of unexpected huge chest wall defect after recurrent breast cancer excision using a TRAM flap combined with partial latissimus dorsi muscle flap. Arch Plast Surg. 2013;40(1):76-79. doi:10.5999/aps.2013.40.1.76
10. Koh AJ, Ng RW, Lee R, Lui WM. Radiation ulcers of the neck should not be neglected: a case of vertebral artery blowout. Asian J Surg. 2007;30(3):230-232. doi:10.1016/S1015-9584(08)60029-9
11. Hanasono MM, Barnea Y, Skoracki RJ. Microvascular surgery in the previously operated and irradiated neck. Microsurgery. 2009;29(1):1-7. doi:10.1002/micr.20560
12. Leonard AG. Musculocutaneous flaps in head and neck reconstruction. Ann R Coll Surg Engl. 1989;71(3):159-168.
13. Al Maksoud A, Moneer M, Barsoum AK. Combined TRAM flap with latissimus dorsi myocutaneous flap for reconstruction of a large breast post-radiation induced necrosis. J Surg Case Rep. 2017;2017(5):rjx079. doi:10.1093/jscr/rjx079






