



Reconstruction of Post-Mohs Surgical Wounds Using a Novel Nanofiber Matrix
Abstract
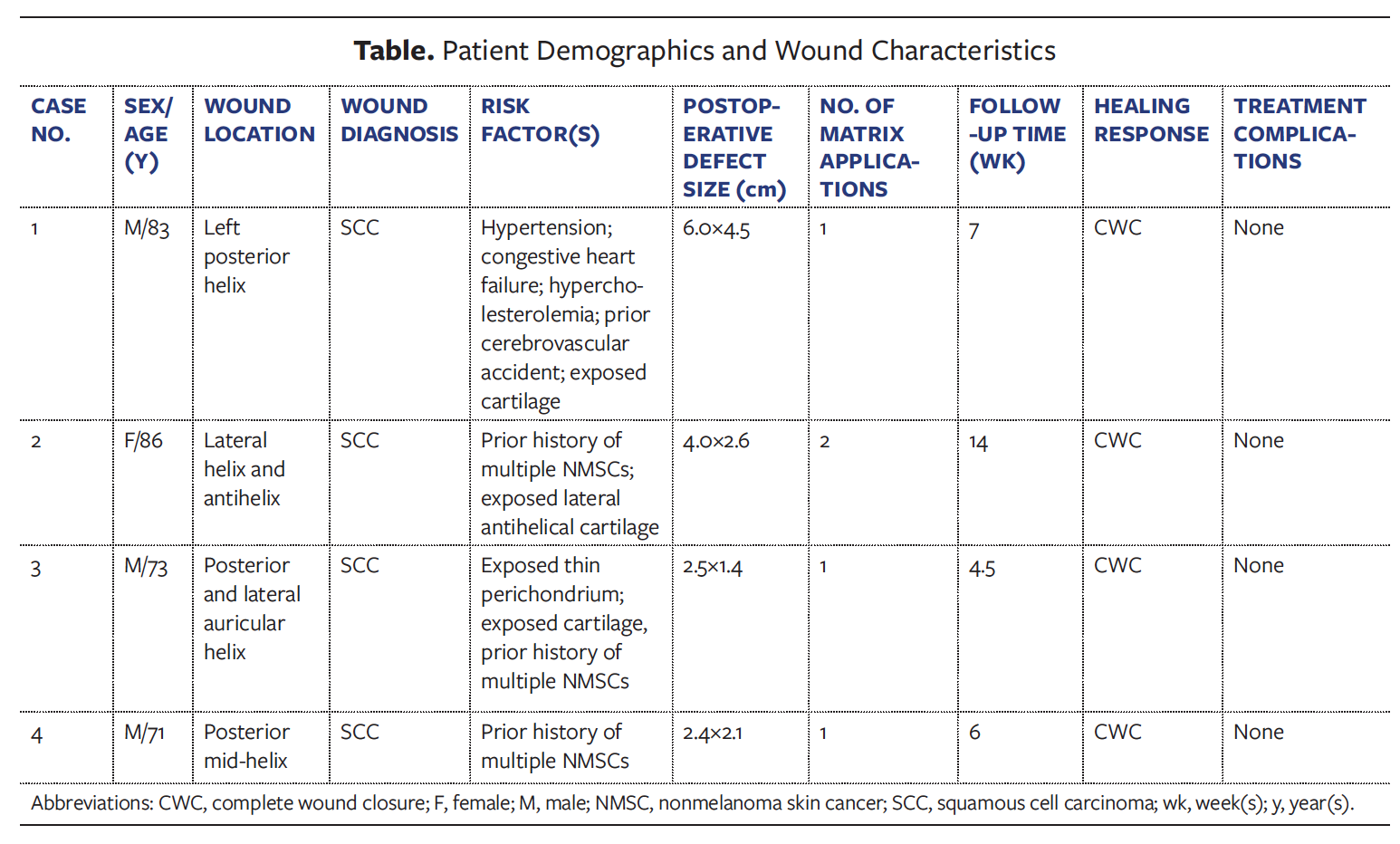
Introduction. Surgical wound healing after Mohs micrographic surgery can be challenging. Achieving an optimal aesthetic outcome is another important consideration, especially for facial lesions. Objective. This case series evaluates the use of a novel synthetic nanofiber matrix after Mohs surgery to achieve desired results. Materials and Methods. Four patients with NMSCs on the auricular helix underwent Mohs micrographic surgery at a single cancer center. The synthetic nanofiber matrix was applied to the prepared Mohs surgical defect and covered with a dressing. The wounds were evaluated regularly for healing progress, and an additional synthetic nanofiber matrix was applied as needed. Results. Wounds were treated with an average of 1.25 applications ± 0.50 standard deviation of synthetic nanofiber matrix. The initial average wound size was 11.8 cm2. All wounds healed in 7.9 weeks ± 4.2 with excellent aesthetic results, minimal scar formation, and no skin deformity. In cases with exposed structures (cartilage and perichondrium), the synthetic nanofiber material promoted complete closure and healing. No complications were reported. Treatment using a synthetic nanofiber matrix resulted in complete wound healing in all patients. Conclusions. This study shows the synthetic nanofiber matrix is a viable option for the reconstruction of post-Mohs surgical defects.
Abbreviations
CVA, cerebrovascular accident; ECM, extracellular matrix; FTSG, full-thickness skin graft; NMSCs, nonmelanoma skin cancers; PLGA, poly(lactin-co-glycolic acid); SCC, squamous cell carcinoma.
Introduction
Mohs micrographic surgery is a common procedure used to remove NMSCs and melanoma skin cancers on the head and neck. Mohs surgery and tumor removal results in a tumor-free surgical defect. Postoperative wound healing after Mohs surgery often is challenging, depending on tumor size, location, and depth, as well as the prevalence of exposed underlying structures.1 Achieving an aesthetic outcome may be an additional expectation, especially for facial lesions.2 Depending on the patient’s medical comorbidities, wound size and/or location, and surgeon-specific preferences, multiple reconstructive approaches may be considered.
One simple method for wound healing involves allowing the wound to self-heal by contraction and epithelialization. In a study of 38 patients with postoperative defects with exposed bone who underwent secondary intention healing, time to epithelialization was 13 weeks.3 This method works well for small circular wounds; however, second intention healing may result in distortion and poor aesthetic outcomes for larger wounds and in certain anatomic locations.4 Alternatively, a common, very simple reconstructive approach is the use of a FTSG. In a clinical study of 50 patients, lower leg defects were treated with FTSGs.5 Thirty days after application, 90% or higher graft take (as an outcome of treatment success) had occurred in 44 patients. Although studies show variable rates of postoperative graft survival, complications associated with skin grafts include graft rejection (10%), infection (11%), and hematoma formation (2.5%).1 Moreover, skin grafts require an additional surgery to harvest the skin from the donor site, thus increasing the rate of postoperative complications, the potential for donor site morbidity, and, often, the total cost of care.
A newer method to treat wounds after Mohs micrographic surgery involves the use of a synthetic nanofiber matrix, such as Restrata (Acera Surgical, Inc.), which is an electrospun biodegradable synthetic nanofiber matrix with an architecture similar to that of human ECM.⁶ This product received US Food and Drug Administration 510(k) clearance in early 2017.⁷ The synthetic nanofiber matrix has a range of fiber diameters and pore sizes that mimic the hierarchical organization of native tissue, and thus support cellular ingrowth, retention, neovascularization, and granulation tissue formation.6 As the fibers gradually degrade over time the porosity opens further, allowing for additional tissue ingrowth and skin regeneration. The synthetic matrix is composed of 2 biocompatible polymers: PLGA (10:90) and polydioxanone. The matrix conforms well to the wound site, due to its flexibility, and has excellent biocompatibility properties. Because of its unique design, the synthetic nanofiber matrix persists in the wound bed, slowly degrades via hydrolysis, and is resistant to enzymatic degradation. The engineered properties and ease of use of the synthetic nanofiber matrix offer an alternative to existing amniotic, allogenic, and/or biologic products, providing a terminally sterilized product with a 2-year shelf life at room temperature that does not require tissue tracking.7
A previous study evaluating chronic lower extremity wounds showed that wounds treated with the synthetic nanofiber matrix demonstrated progressive wound area reduction over the course of treatment and that the matrix could support the natural wound healing process.8 The current study evaluates the efficacy of the synthetic nanofiber matrix for treating wounds after Mohs micrographic surgery in 4 patients. Following application of the synthetic nanofiber matrix, wounds were monitored to evaluate how the material supported the healing process.
Materials and Methods
This single-arm retrospective clinical study was conducted at the South Carolina Skin Cancer Center in Greenville, South Carolina. Patients enrolled in this study were diagnosed with skin cancer, needed treatment for post-Mohs defects, and had no known sensitivity to absorbable sutures or synthetic wound matrices. Four patients who met the inclusion criteria for the study had skin cancers on the auricular helix. All patients underwent Mohs micrographic surgery until tumor-free wound margins were obtained.
A treatment regimen that used the synthetic nanofiber matrix was chosen to reconstruct the post-Mohs wounds. To apply the matrix, the material was cut to the shape and size of the wound and fenestrated by the surgeon using a herringbone pattern. The synthetic matrix was hydrated for 10 minutes in the saline solution before application. The synthetic nanofiber matrix was placed in complete contact with the wound bed and anchored with poliglecaprone 25 or 5-0 fast-absorbing surgical gut suture. A bolster pressure dressing was sewn to the graft to facilitate optimal adhesion to the underlying wound bed. The bolster was composed of xeroform gauze and sewn to the wound bed using 5-0 nylon nonabsorbable suture. An additional layer of petrolatum was applied over and around the xeroform bolster and covered with a dressing that was changed as necessary during the treatment period. Patients applied additional petrolatum and rebandaged their wounds daily using nonabsorbent gauze and surgical tape. Wound evaluations were performed weekly to monitor wound healing progress and report any observed complications, and the matrix was reapplied as needed.
Results
In this study, 4 patients with post-Mohs wounds on the auricular helix were enrolled (Table). Wounds were treated by applying an appropriately sized synthetic nanofiber matrix to cover the wound bed. The healing response of each patient is presented here.
Patient 1 is an 83-year-old male with multiple medical comorbidities, including hypertension, congestive heart failure, hypercholesterolemia, and prior CVA, residing in an assisted living facility. The patient presented with a keratoacanthoma-type SCC of the left posterior helix measuring 3.5 cm × 2.0 cm on the day of biopsy (Figure 1A). On initial presentation, the lesion presented as a firm noduloulcerative plaque that was concerning for NMSC.
The patient was referred for Mohs micrographic surgery, and after 2 stages, tumor-free margins were obtained. The SCC measured 5.5 cm × 3.5 cm preoperatively on the day of Mohs surgery (Figure 1B). The tumor had expanded extensively since the date of biopsy and demonstrated a violaceous, rolled, undermined border indicative of central necrosis. Intraoperative curettage was performed before Mohs surgery stage I, which extended down to the layer of the auricular cartilage.
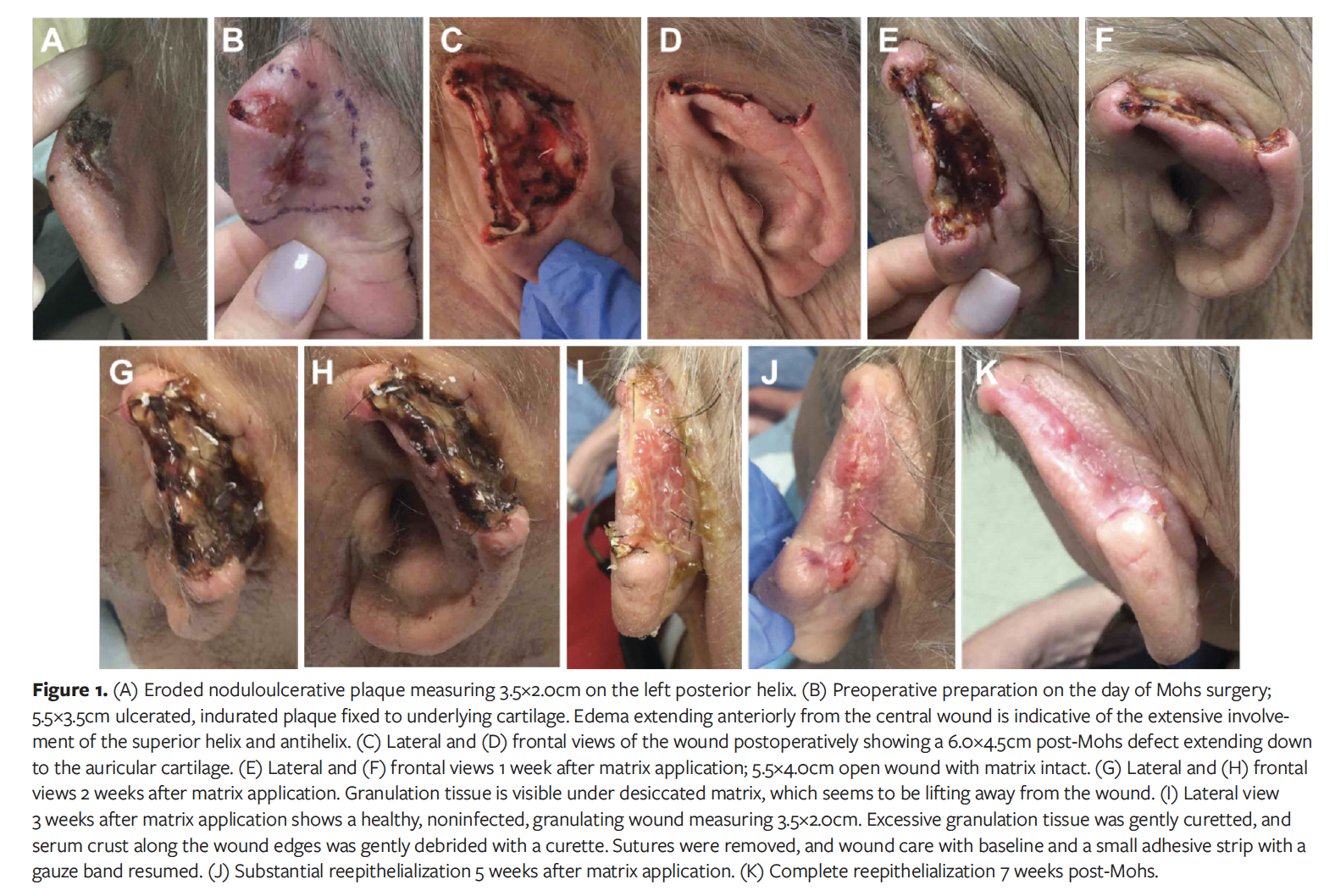
Microscopically, extensive tumor involvement throughout the dermis and subcutaneous fat was noted. Tumor morphology showed keratoacanthoma-like features with epidermal invaginations and keratinocytic atypia. Foci of moderately differentiated, invasive SCC were visualized. The resultant Mohs defect was large and deep, extending down to the layer of auricular cartilage and involving much of the anterosuperior helix and posterior auricle. The postoperative defect measured 6.0 cm × 4.5 cm after achieving tumor-free margins (Figure 1C, 1D). Because of the size and depth of the postoperative defect, limited reconstructive options were available. Because of the patient’s multiple medical comorbidities, concurrent anticoagulation, and advanced age, he declined a large mastoid pedicle interpolation flap. Instead, the patient and his family expressed a preference for other treatment modalities to expedite wound healing.
Because the postoperative defect was large and deep, synthetic nanofiber matrix was used to promote efficient granulation and reepithelialization. Seven days after Mohs surgery, moderate debridement was performed to freshen the epidermal edges and remove residual cautery artifact resulting from Mohs surgery. A 7.5-cm × 7.5-cm piece of the synthetic nanofiber matrix was trimmed, fenestrated, hydrated, and sutured to the open wound bed. The wound was hydrated with daily applications of a hydrogel under a Mepilex (Mölnlycke Health Care) bandage. One week after application of the synthetic matrix, the wound had decreased in size to 5.5 cm × 4.0 cm (Figure 1E, 1F). Two weeks after matrix application (Figure 1G, 1H), significant granulation tissue had formed, the wound size had reduced to 5.0 cm × 3.0 cm (equal to 44% wound area reduction), and previously exposed cartilage was completely covered. Desiccated matrix and eschar were removed using moderate debridement with a No. 15 scalpel. Here, the term eschar is used to describe the clinical appearance of agminated, black, thickened serum crusts that are tightly bound to the wound bed. In contradistinction to its use historically, here eschar does not in any way signify tissue death but instead represents a dynamic process of tissue regeneration. The patient was followed up at approximately weekly intervals, and continuous epithelialization and granulation tissue formation were observed (Figure 1I, 1J) until complete reepithelialization was noted 7 weeks later (Figure 1K). No complications were reported during the course of treatment.
Patient 2 is an 86-year-old female with a prior history of multiple NMSCs who resided in an assisted living facility. The patient presented with an invasive SCC on the lateral helix and antihelix. Keratoacanthoma-type SCC at the left posterior helix measured 1.3 cm × 1.4 cm on the day of biopsy (Figure 2A). At the time of Mohs micrographic surgery, the lesion presented as a crusted, hyperkeratotic plaque and central scar measuring 2.0 cm × 1.5 cm. Cancer-free margins were obtained after 3 stages, due to extensive superficial SCC in situ with adnexal involvement.
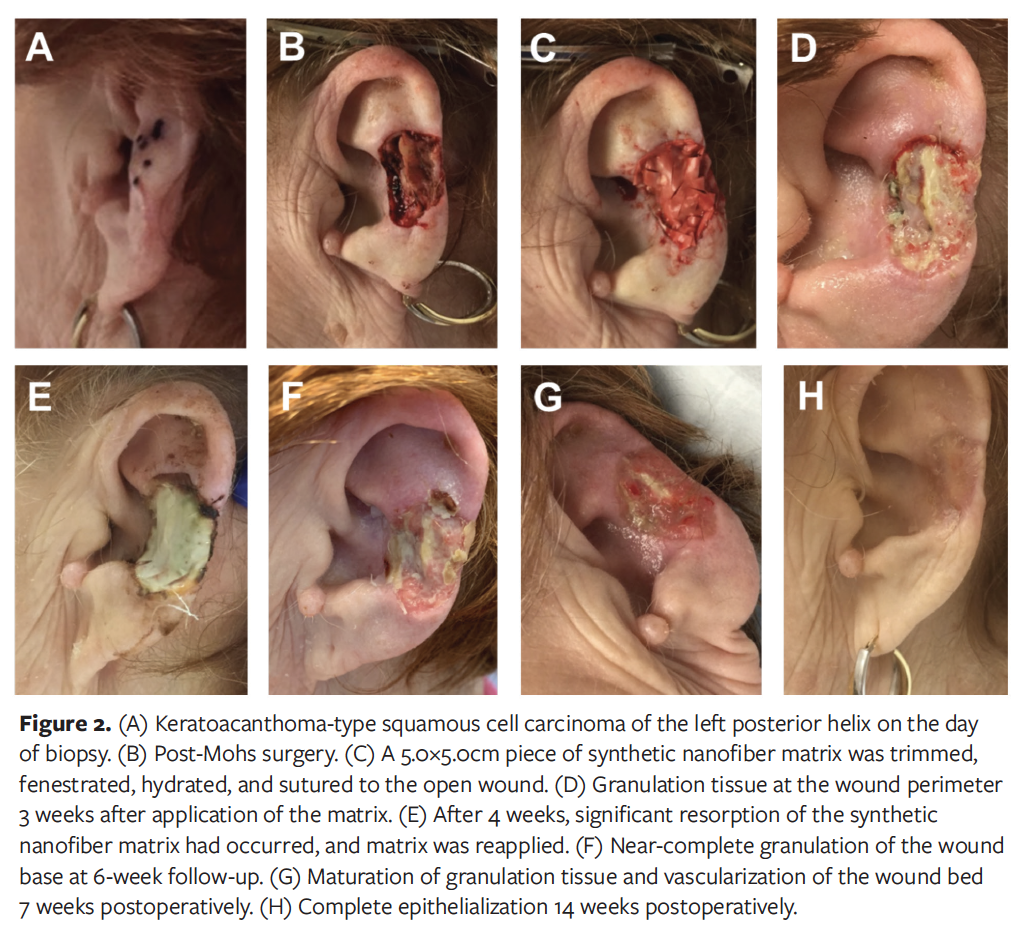
The resultant Mohs defect measured 4.0 cm × 2.6 cm and demonstrated a 1.5-cm focus of exposed lateral antihelical cartilage that prevented the execution of an FTSG (Figure 2B). The remainder of the wound was insulated with only a thin, delicate layer of perichondrium that was susceptible to desiccation and poor wound healing. Because of the complicated auricular anatomic site, exposed cartilage, and vulnerability of the delicate perichondrial layer, in addition to the patient’s older age and limited access to consistent, proper wound care, the synthetic nanofiber matrix was chosen for reconstruction.
The matrix application was performed after histologic clearance with Mohs surgery. On postoperative day 0, a 5.0-cm × 5.0-cm piece of the material was trimmed, fenestrated, hydrated, and sutured to the open wound using 5-0 fast-absorbing gut suture (Figure 2C). The patient was followed up at approximately weekly intervals. At 3 weeks postoperatively and after gentle debridement was performed at that visit, granulation tissue was apparent at the wound perimeter and fibrinous primitive perichondrium was noted (Figure 2D). Reepithelialization was noted along the perimeter of the wound followed by a moist layer of primitive granulation tissue. The wound dimensions measured 3.2 cm × 2.2 cm (equal to 32% wound area reduction). After 4 weeks, significant resorption of the synthetic nanofiber matrix was observed, and the matrix was reapplied (Figure 2E). Gentle debridement was performed on the edges only. Near-complete granulation of the wound base was observed at 6-week follow-up (Figure 2F). Maturation of granulation tissue and vascularization of the wound bed were noted at 7 weeks postoperatively (Figure 2G). Follow-up continued until complete reepithelialization at the wound site was noted 14 weeks later, with an excellent aesthetic result and no complications (Figure 2H).
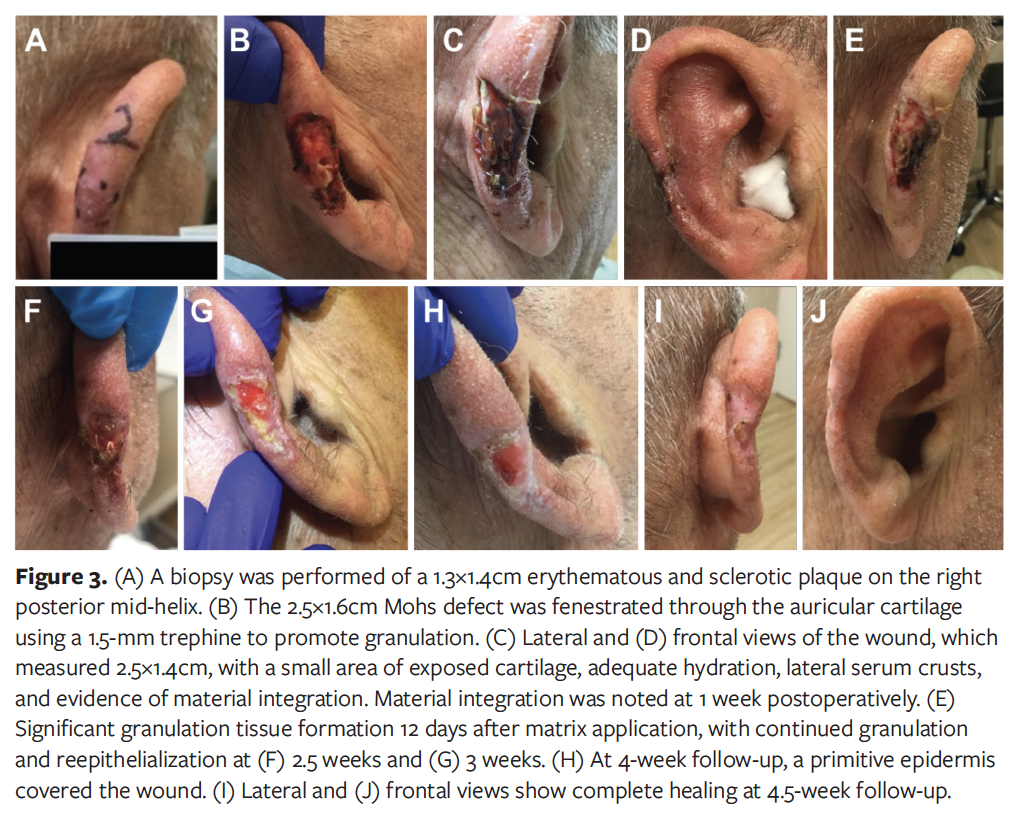
Patient 3 is a 73-year-old male with a prior history of multiple NMSCs. The patient presented with an invasive SCC on the posterior and lateral auricular helix measuring 1.3 cm × 1.4 cm on the date of biopsy (Figure 3A). Two stages of Mohs micrographic surgery were required to obtain cancer-free margins, resulting in a 2.5-cm × 1.6-cm deficit with exposed thin perichondrium and a small focus of exposed cartilage (Figure 3B). Small fenestrations were made through the lateral and posterior helical cartilage using a 1.5-mm trephine to facilitate more rapid granulation.
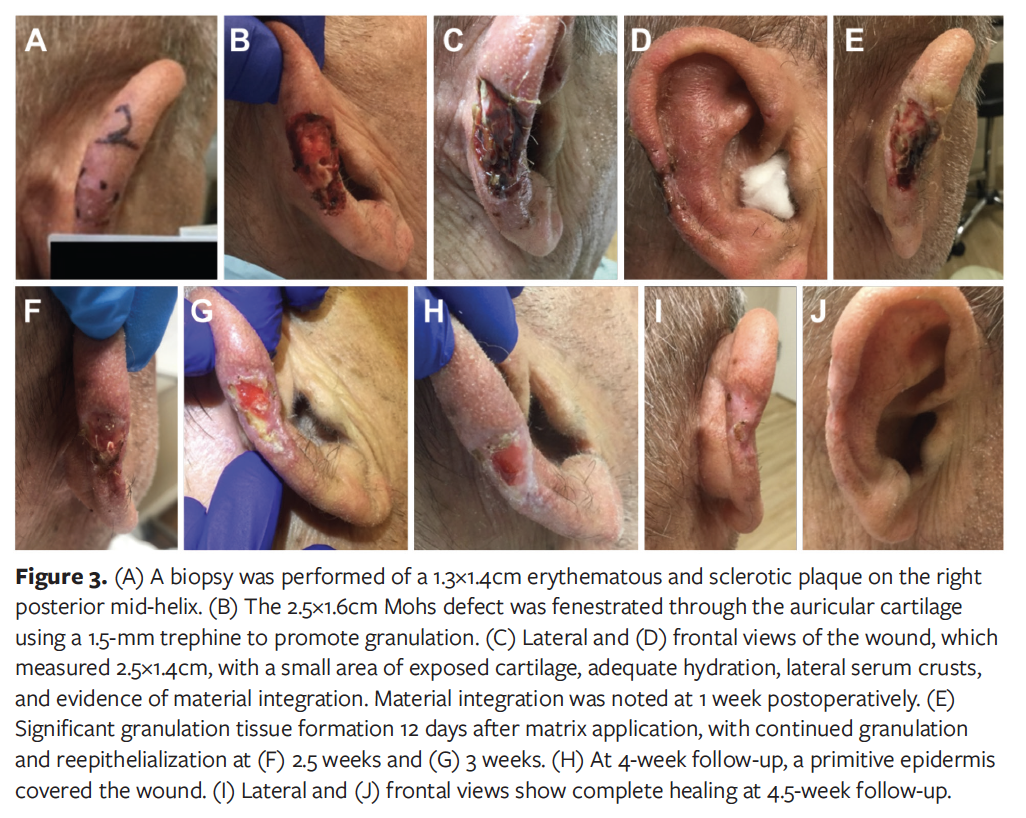
The defect was located on the posterior auricular helix and, thus, was not easily accessible or visible. The patient lived at home and alone (no one home to assist with wound care), and expressed concern about being able to self-administer adequate wound care due to the location of the wound. For this reason, as well as the moderate size and depth and potential for protracted wound healing, a 2.5-cm synthetic nanofiber matrix was used for reconstruction. Four days after Mohs surgery, a gentle debridement was performed, after which a 2.5-cm matrix graft was placed using poliglecaprone 25 and 5-0 surgical gut absorbable suture to ensure a tight seal between the product and the wound bed.
The patient was followed up regularly, and gentle debridement was performed when necessary. One week after application of the synthetic nanofiber matrix, gentle debridement was performed peripherally to remove serum crusts without disturbing the material. The wound measured 2.5 cm × 1.4 cm, with a small area of exposed cartilage, adequate hydration, lateral serum crusts, and evidence of product integration (Figure 3C, 3D). At day 12, debridement was performed, and after debridement, dramatic granulation was noted posteriorly where prior serum crusts and thick black eschar was removed (Figure 3E). Anteriorly, along the lateral helix where the perichondrium is thinner, the eschar was more tightly bound down. The eschar represented active integration of the synthetic nanofiber matrix and was not excessively debrided, because of the potential for such trauma to the tissue to interfere with full material integration. The wound dimensions were 2.3 cm × 1.3 cm. Dramatic reepithelialization and granulation at the wound site were evident 2.5 weeks after matrix application, at which time the wound measured 1.4 cm × 0.8 cm (Figure 3F). Near-complete healing occurred 3 weeks after the synthetic nanofiber matrix application. A thin rim of pseudo-desiccation outlined central granulation tissue with continued reepithelialization. The wound measured 1.3 cm × 0.7 cm (Figure 3G). Four weeks after matrix application, a thin, primitive epidermis covered the entire wound (Figure 3H), and at 4.5 weeks, wound healing was complete (Figure 3I, 3J). The wound was fully epithelialized and the helix was reconstructed with minimal signs of scar and no complications.
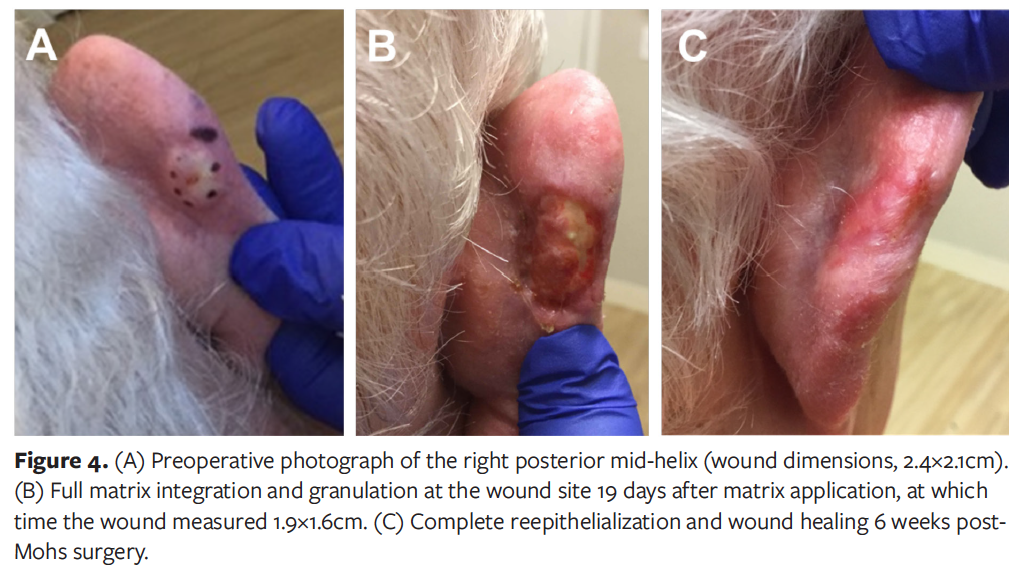
Patient 4 is a 71-year-old healthy male with a biopsy-proven sclerosing basal cell carcinoma on the posterior mid-helix (Figure 4A). This patient had also experienced multiple prior NMSCs. Four stages of Mohs micrographic surgery were required to clear the tumor, and the resultant postoperative defect was measured. Multiple reconstructive options were considered, including FTSG vs reconstruction with the synthetic nanofiber matrix, and the patient emphatically expressed a preference for the latter because of its relative ease and the minimal need for further extensive or invasive surgery. Granulation tissue formation and complete reepithelialization were observed at 19 days and 6 weeks, respectively, after matrix application (Figure 4B, 4C). No complications were reported.
Discussion
Although NMSCs continue to increase in incidence and prevalence, certain anatomic locations, notably the ear, require a particularly aggressive clinical course9; this approach may be needed due to the proximity of the epidermis to the fascial or perichondrial layer. Large auricular wounds that result from microscopic clearance of such aggressive cancers are not unfamiliar to the Mohs micrographic surgeon. Such postoperative wounds with large surface areas, exposed cartilage, or exposed delicate perichondrium are a reconstructive challenge.10 Until recently, Mohs micrographic surgeons relied on continued wound care, frequent postoperative visits, protracted wound healing, and the possibility of a delayed graft when managing NMSCs. However, grafting over exposed cartilage or a delicate network of avascular perichondrium is contraindicated and results in a poor healing response. In an aging population with the potential for medical comorbidities—including diabetes, vasculopathy of multiple etiologies, and malnutrition—rates of granulation are unpredictable and, in many instances, difficult to manage. Wound care is impossible to standardize and quite difficult functionally for certain patients who do not have a caregiver to assist in consistent, proper bandage changes.
In the past 2 decades, there has been a proliferation of skin substitutes, including newer allogenic dehydrated human amnion/chorion membrane (EpiFix; MiMedx) and its predecessor, porcine small intestine submucosa (Oasis; Smith + Nephew). Both skin substitutes are composed of a thin disk with epidermal growth factors, which are involved in wound healing.11,12 However, they are dispersed over a short time frame and are rapidly resorbed. Thus, multiple applications are necessary to sustain continued wound healing.
Wounds with exposed structure are particularly challenging to heal. Secondary intention healing would not be the ideal treatment for such wounds because it may result in prolonged healing with scar formation and skin deformity. Moreover, patients with multiple comorbidities may not qualify for skin grafts and may not be able to undergo an additional surgery for harvesting the graft. Advanced wound therapies, including amnion/chorion membrane and intestinal submucosa, require several applications, which adds to the overall labor and cost burden of the treatment. In contrast, the matrix used in this study was successfully applied to the wounds with exposed structure, thus avoiding the need for FTSG. Additionally, the matrix degrades slowly in the wound, which minimizes the need for multiple applications. The synthetic matrix may also offer additional benefits of shortening the treatment duration to achieve complete wound healing and reducing the number and severity of complications after application.
The matrix used in the current study is composed of synthetic nanofibers that preserve the structural integrity of the wound, and it has sufficient tensile strength to be sutured or stapled in place, which reduces the risk of product displacement and an undesirable outcome.7 The nanofiber matrix acts as a scaffold for cellular migration, proliferation, and differentiation; provides a framework for reepithelialization; and activates fibroblasts for continued wound maturation and scar remodeling.6 A preclinical study in a porcine model showed substantial granulation tissue formation with minimal inflammatory response when the full-thickness wound was managed with the synthetic nanofiber matrix.13 Moreover, the architecture of synthetic nanofiber matrix is similar to that of native ECM, allowing for tissue ingrowth as well as neovascularization of the newly forming tissue.6 This dynamic cascade of events allows the natural healing process to occur. The fully healed wounds with excellent aesthetic results presented in this study demonstrate that the synthetic nanofiber matrix can support nearly scarless wound healing.
Three of the 4 patients included in this study were male (average age, 78 years). Major comorbidities included hypertension, congestive heart failure, and CVA. Exposed cartilage and perichondrium were present in 3 wounds. Wounds were treated with an average of 1.25 applications ± 0.50 of synthetic nanofiber matrix. The average size of the initial wounds was 11.8 cm2. All wounds completely healed in 7.9 weeks ± 4.2, with excellent aesthetic results, minimal scar formation, and absence of skin deformity. In cases with exposed structures (cartilage and perichondrium), the synthetic nanofiber material promoted complete closure and healing. No complications were reported.
Application of the synthetic nanofiber matrix to large auricular wounds appears to reduce the time to wound healing. Because of the biomimetic nature of the synthetic nanofiber matrix, it is recognized as a receptive tissue scaffold; it prompts robust and sustained cellular infiltration, neovascularization, and new tissue formation critical to native wound healing.⁶ It is hypothesized that such a continued burst of cellular activity causes a protracted and prolonged burst of growth factors and cytokines critical to the acute wound healing process, which ultimately results in a rapid and dramatic host granulation and reepithelialization response.11
The cellular changes that occur are important because of the cascade of cytokines or growth factors that each cell line offers to the local milieu. During inflammation, the neutrophil is vitally important. It is drawn in immediately and attracted to the initial clot formation on the day of surgery. Granulation occurs after this initial neutrophil surge; however, for large auricular wounds with central exposed areas of relatively avascular cartilage and perichondrium, there is no route for the neutrophil to reach the wound. Thus, these wounds are neutrophil-deficient and fibroblast-deficient. The final stage is wound contraction or maturation, a phase that continues for months to years, during which attenuated fibroblasts called myofibroblasts continue to refine the newly synthesized epidermis to its original tensile strength.
Because the synthetic nanofiber matrix provides a structural framework that gradually integrates into the postoperative wound, the material provides a scaffold that may harness the heightened and accentuated pro-regenerative cellular response originating in the wound bed. The honey-colored serum crusts and pseudo-desiccated appearance observed around week 5 after application (not to be confused with impetiginization) reflect the formation of a substrate that traps moisture into the base of the wound, where vigorous granulation tissue formation is occurring.
The treatment in case 3 demonstrated an even deeper understanding of the dynamic wound healing that occurs after reconstruction with the synthetic nanofiber matrix. In addition to expediting wound healing, the synthetic nanofiber matrix is an important reconstructive option for patients who are unsure, nonparticipatory, or reticent about wound care. The author used this opportunity to facilitate close clinical observation and to deliver customized, frequent wound care to this patient. Frequent wound checks (per patient request) facilitated frequent debridement, clinical surveillance, and digital photography. The post-matrix wound in Figure 3E at 12 days after product placement demonstrates the centripetal progression of matrix integration wherein a black eschar first appeared peripherally at the interface between the synthetic nanofiber matrix and the actively regenerating skin edge. This dynamic interface reaction can be displayed visually as a peripheral halo of black eschar evolving into a near-complete eschar covering most of the surface area of the wound bed. This process is referred to as a dynamic centripetal interface reaction.
The rate at which the matrix integrates into the postoperative wound is designed to parallel the rate at which granulation occurs.4 Thus, intraoperative surgical execution, postoperative wound care, and choice of the correct emollient are quite important. The author recommends sewing the matrix to the wound using absorbable sutures, such as the poliglecaprone 25 or 5-0 fast-absorbing surgical gut sutures that were used in this series. Sutures are very important in the use of matrices for reconstruction, because they allow the matrix to maintain a tightly adherent so-called seal with the wound bed, resulting in rapid integration and wound healing. Also, owing to the complex geometry of the auricular surface, maintaining a tight seal can be more difficult than on other, flatter surfaces. Moreover, wound care using a thin layer of a silicone foam dressing and copious hydrogel provides protection, insulation, and moisture balance for the matrix. The silicone foam dressing is removed daily so that hydrogel can be applied over the absorbent foam dressing porous dressing. Replacing the layer of silicone foam dressing can help waterproof the wound, especially when the patient adheres with instructions to avoid submerging or immersing the wound in water.
The pseudo-desiccated appearance of wounds after matrix application can sometimes give the illusion of noncompliance or poor host response. Despite its appearance, however, progress is occurring at the cellular level and is contributing to the rapid granulation and wound healing process.
Limitations
While this initial case series shows promising results, there are limitations within the design of the study. This study involved only 4 patients with no control group at a single site. To fully investigate the efficacy of the synthetic nanofiber matrix in the treatment of post-Mohs surgical wounds, a multicenter, randomized clinical trial should be considered.
Conclusions
Synthetic nanofiber matrices are a novel option for reconstructing post-Mohs surgical wounds. This method accelerates the healing process by facilitating cellular infiltration, granulation tissue formation, and neovascularization. Future studies can be conducted to investigate the efficiency of this nanofiber matrix in the treatment of defects in other anatomic areas and with larger patient populations.
Acknowledgments
Author: Joseph McGowan, MD
Affiliation: South Carolina Skin Cancer Center, Dermatologic Surgery, Greenville, SC
Disclosure: Dr. McGowan has received financial compensation as a consultant for Acera Surgical within the past 3 years.
Correspondence: Joseph McGowan, MD, MOHS Surgeon, South Carolina Skin Cancer Center, Dermatologic Surgery, 300 Ashby Park Lane, Greenville, SC 29607; jmcgowaniv@gmail.com
References
1. Oganesyan G, Jarell AD, Srivastava M, Jiang SIB. Efficacy and complication rates of full-thickness skin graft repair of lower extremity wounds after Mohs micrographic surgery. Dermatol Surg. 2013;39(9):1334-1339. doi:10.1111/dsu.12254
2. Faulhaber J, Géraud C, Goerdt S, Koenen W. Functional and aesthetic reconstruction of full-thickness defects of the lower lip after tumor resection: analysis of 59 cases and discussion of a surgical approach. Dermatol Surg. 2010;36(6):859-867. doi:10.1111/j.1524-4725.2010.01561.x
3. Becker GD, Adams LA, Levin BC. Second intention healing of exposed scalp and forehead bone after Mohs surgery. Otolaryngol Head Neck Surg. 1999;121(6):751-754. doi:10.1053/hn.1999.v121.a98216
4. Dobke MK, Miller SH. Tissue repair after Mohs surgery. a plastic surgeon’s view. Dermatol Surg. 1997;23(11): 1061-1066. doi:10.1111/j.1524-4725.1997.tb00448.x
5. Audrain H, Bray A, De Berker D. Full-thickness skin grafts for lower leg defects: an effective repair option. Dermatol Surg. 2015;41(4):493-498. doi:10.1097/DSS.0000000000000330
6. MacEwan MR, MacEwan S, Kovacs TR, Batts J. What makes the optimal wound healing material? A review of current science and introduction of a synthetic nanofabricated wound care scaffold. Cureus. 2017;9(10):e1736. doi:10.7759/cureus.1736
7. Restrata. Acera Surgical Inc. Accessed July 22, 2020. https://acera-surgical.com/restrata/
8. Regulski MJ, MacEwan MR. Implantable nanomedical scaffold facilitates healing of chronic lower extremity wounds. Wounds. 2018;30(8):E77-E80.
9. Duffy KL, McKenna JK, Hadley ML, Tristani-Firouzi P. Nonmelanoma skin cancers of the ear: correlation between subanatomic location and post-Mohs micrographic surgery defect size. Dermatol Surg. 2009;35(1):30-33. doi:10.1111/j.1524-4725.2008.34379.x
10. Galadari H, Abrou A, Rogers G. Fenestration of auricular cartilage to expedite secondary intention healing. Surg Pract. 2007;11(4):159-161.
11. Maan ZN, Rennert RC, Koob TJ, Januszyk M, Li WW, Gurtner GC. Cell recruitment by amnion chorion grafts promotes neovascularization. J Surg Res. 2015;193(2):953-962. doi:10.1016/j.jss.2014.08.045
12. Hodde JP, Ernst DMJ, Hiles MC. An investigation of the long-term bioactivity of endogenous growth factor in OASIS Wound Matrix. J Wound Care. 2005;14(1):23-25. doi:10.12968/jowc.2005.14.1.26721
13. MacEwan MR, MacEwan S, Wright AP, Kovacs TR, Batts J, Zhang L. Comparison of a fully synthetic electrospun matrix to a bi-layered xenograft in healing full thickness cutaneous wounds in a porcine model. Cureus. 2017;(9)8:e1614. doi:10.7759/cureus.1614





