Three-Year Experience With Combined Complex Skin Repair in Patients With Extensive Burns: A Retrospective Study
Abstract
Introduction. The Meek micrografting technique used in STSG expansion is effective in achieving wide and rapid coverage of burn wounds. Certain growth factors have also been shown to modulate or mediate wound healing. Objective. In this study, a combined treatment approach for severe burns involving the Meek micrografting technique, systemic application of rhGH, and topical application of rhEGF was evaluated. Materials and Methods. A retrospective study was conducted of 7 extensively burned patients who were treated with the Meek technique, systemic application of rhGH, and topical application of rhEGF between January 2017 and December 2019. Results. The mean percent TBSA burned was 89%. An average of 9.5 surgical procedures were performed to obtain skin cover, with an average of 5.8 Meek micrograft procedures performed in the 6 surviving patients. Complete wound healing was achieved at an average of 120 days in the 6 surviving patients. The mean graft take rate was 81%. Infection was the main reason for graft failure. Donor sites were used for up to 5 re-harvestings without additional morbidity. Conclusions. A multipronged treatment approach that combines the Meek micrografting technique, systemic application of rhGH, and topical application of rhEGF is a promising tool for the management of severe and extensive burns.
Abbreviations
EGF, epidermal growth factor; LOS, length of stay; rhEGF, recombinant human EGF; rhGH, rh growth hormone; STSG, split-thickness skin graft; TBSA, total body surface area.
Introduction
Mortality from severe burns in the early stages of treatment has decreased substantially owing to increased knowledge of burn pathophysiology and of fluid and electrolyte balance, as well as to improvements in intensive care, burn treatment modalities, infection control, and nutritional support. This has led to a growing number of survivors requiring skin grafting procedures.1 However, limited donor site availability remains a challenge for achieving rapid closure of burn wounds. Various skin grafting techniques, such as Meek micrografting and meshed grafting, have been developed to allow skin graft expansion to cope with restricted donor site availability.2
Cicero Parker Meek first described his eponymous micrografting technique in 1958.3 It involves harvesting STSGs and expanding them to achieve a desired expansion ratio of up to 1:9. However, the Meek technique fell out of favor following introduction of the mesh skin graft by James C. Tanner and colleagues in 1964, which was more user-friendly and was therefore rapidly and widely adopted.4 Although technically easier, the mesh technique was limited by a lower expansion rate, and thus, the donor site deficit remained a challenge in patients with extensive burns.4 In 1993, R. W. Kreis and colleagues modified the Meek technique to make it faster and more efficient, and it gained the attention of burn surgeons as an effective alternative for the treatment of patients with massive burns.5
Large burn injuries promote a hypermetabolic state that involves an imbalance in protein metabolism, namely, protein catabolism. Protein catabolism is characterized by a decrease in protein synthesis and an increase in protein breakdown. There is some evidence that protein catabolism delays healing of the burn wound and of the donor and/or recipient areas.6 This hypercatabolic state can be attenuated or even reversed by treatment with anabolic agents such as rhGH.6 Herndon et al7 reported that use of rhGH reduced donor site healing time in children with burns. In addition, a review published in 2014 demonstrated that use of rhGH therapy in patients with severe burns resulted in more rapid healing of the donor sites and burn wounds.6
Wound healing is a dynamic process that involves several overlapping stages, including inflammation, the formation of granulation tissue, reepithelialization, and formation and remodelling of matrix.8 This complex process is finely regulated by multiple interactions between growth factors9 based on their biological functions, and by the biological characteristics of wound healing.10 EGF is produced by platelets, monocytes, and macrophages. EGF has a major effect on wound healing by stimulating the migration and proliferation of epithelial cells, keratinocytes, endothelial cells, and fibroblasts, and by facilitating the formation of granulation tissue.11 Some clinical studies have demonstrated that EGF reduces wound healing time. Xing et al12 reported that topical application of rhEGF in wound dressings at donor sites was associated with more rapid reepithelialization and faster wound healing compared with application of saline gauze.
Based on the aforementioned findings, the authors of the current study evaluated a combined treatment approach for severe burns that involved the Meek micrografting technique, systemic application of rhGH, and topical application of rhEGF.
Materials and Methods
Patients
The authors retrospectively reviewed the medical records of all severe burn patients admitted to the burns unit at The First Affiliated Hospital of Guangxi Medical University, Nanning, Guangxi, China, between January 2017 and December 2019 and who were treated with the Meek technique in conjunction with systemic application of rhGH and topical application of rhEGF. The following data were collected for each patient: demographics, details of their burns, surgical management, clinical course, and outcomes. All patients were followed up for 14 to 24 months in the outpatient clinic after discharge from the hospital. The institutional review board of the authors’ hospital approved this study.
Management
Initial fluid was determined based on the Third Military Medical University (TMMU) formula, and further use of colloid solution was based on clinical manifestations. Decompression of limb compartments was performed as indicated. Patients were placed in specialty beds that provide air-fluidized therapy (Fluid Air), which helped restore a dry wound and skin microenvironment and helped reduce sheer stress. Air-fluidized therapy has been shown to be effective in reducing pressure ulcers, minimizing bacterial infection, and enhancing wound healing.13 Initially, silver sulfadiazine was used to cover burn wounds. After informed consent was obtained from the legal guardian or guardians, all patients were treated with rhGH (batch number 20170110, 20181025, 20190105; Anhui Anke Bioengineering Co., Ltd.) at 0.2 mg/kg daily and administered subcutaneously once daily until complete wound healing was achieved. Throughout the treatment course, all patients continued to receive topically applied ointment and/or elastic devices to minimize scarring.
Surgical technique
Tangential excision. Once patients were considered to be respiratory and hemodynamically stable, they were taken to the operating room for early tangential excision of burned skin. The Humby knife and Weck knife were most frequently used to shave the burned skin down to healthy tissue (as identified by punctate bleeding) in preparation for grafting. The entire skin down to the fascia was removed as indicated. Hemostasis was maintained with electrocauterization and topical epinephrine, and blood volume was replenished as necessary.
The Meek graft technique. STSGs were obtained using a Meek dermatome and placed dermis side down on damp cork squares. The cork plate with the STSG was then passed through a cutting machine with 13 blades. This cut the graft into 14 strips of skin, each with a 3-mm width. After the first pass, the cork was rotated 90° and passed through the cutting machine once more. This cut the STSGs into 196 pieces of micro-size skin grafts, each measuring 3 mm × 3 mm.
The cut grafts were then transferred to folded gauze with an aluminium foil backing by removing the cork plate. The epidermal upper surface of the grafts was sprayed with an adhesive glue and allowed to dry for 10 to 15 minutes. The gauze was expanded in all directions until it was completely flattened and smooth, to obtain a graft with an expansion ratio of 1:6. The grafts with gauze backing were then placed onto the prepared wound bed with the dermis side down. The Meek micrografts received topical application of rhEGF (batch number 20161108, 20170710, 20180610, 20190302; Huashengyuan Genetic Engineering Development Co., Ltd.) on the skin squares and then adhered to the expandable carrier. The grafted wound was covered with a silver sulfate dressing and wrapped with cotton bolsters and bandages that remained in place until postoperative day 3. The gauze backing with grafts was left in place for 10 to 14 days, but the outer dressings were replaced every 2 days or earlier if clinically necessary. To accelerate healing of the Meek grafts, recipient areas received topical application of rhEGF placed on the backing gauze during each dressing change. During these dressing changes, the occurrence of any infection at the grafted site where the backing gauze tended to lift off could be readily detected.
Repeated harvesting of STSG. Subcutaneous injection of tumescent fluid at the skin graft donor site was done to facilitate skin graft harvesting with reduced donor site morbidity and to minimize intraoperative blood. STSGs were harvested using a Zimmer dermatome (Zimmer Biomet) with the thickness set to 0.20 mm to 0.25 mm. Owing to a shortage of available donor sites, it was necessary to re-harvest STSGs from the same anatomic areas. STSG donor sites were treated with a semi-open technique by using silver sulfate dressings to cover the wound immediately after harvesting. These dressings were left in place for 7 to 15 days to protect against infection during wound healing. To facilitate regeneration, donor areas were treated with rhEGF placed on the silver sulfate dressing twice daily.
Results
Demographics and burn injury profile
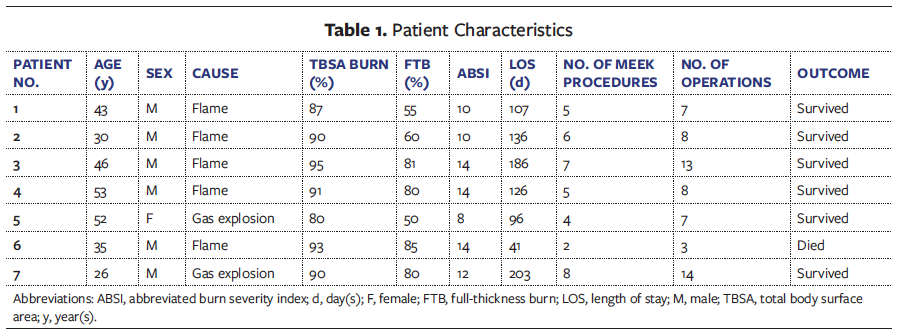
A total of 7 patients treated in the 3-year study period were identified (Table 1). The mean age at burn injury was 41 years (range, 26-53 years). Five cases were flame burns and 2 were gas explosion burns. All burns were deep dermal to full thickness, with an average of 89% TBSA burned (range, 80%-95%), and third-degree burns comprised 78% of all burns (range, 50%-85%). All 7 patients sustained deep partial- and full-thickness burns. Associated inhalation injury occurred in 5 patients; these patients underwent tracheotomy on admission, with 4 requiring mechanical ventilation for 28 to 55 days. The mean abbreviated burn severity index for the whole cohort was 11.7 (range, 8-14).
In the 6 surviving patients, complete wound healing was achieved at an average of 120 days (range, 84-162 days), which equated to 1.4 days per percentage burn, and the mean hospital LOS was 142 days (range, 96-203 days). One patient died of sepsis 41 days after admission, resulting in a survival rate of 85.7%.

The Meek technique
An average of 9.5 surgical procedures were performed (range, 7-14) to obtain skin cover, with an average of 5.8 Meek micrograft procedures (range, 4-8) performed in the 6 surviving patients. The modified Meek grafting achieved an overall mean take rate of 81% (range, 53%-95%) and a mean take rate of 82% (70%-95%) in the 6 surviving patients. The patient who died had undergone 2 Meek micrograft procedures during his treatment course, with a take rate of 70% and 50%. Wound infection was the main reason for graft failures and included swab cultures that were positive for Acinetobacter baumannii (3 cases) and Pseudomonas aeruginosa (1 case). Infected wounds were treated daily with 0.1% chlorhexidine acetate, followed by silver-impregnated dressing (Atrauman; Paul Hartmann Limited) until the infection resolved. All patients experienced small areas (8%-15%) of graft loss that required regrafting. The wounds treated with Meek grafts showed good aesthetic appearance and good pliability (Figure 1).
Repeated harvesting of STSG and rapid donor site healing
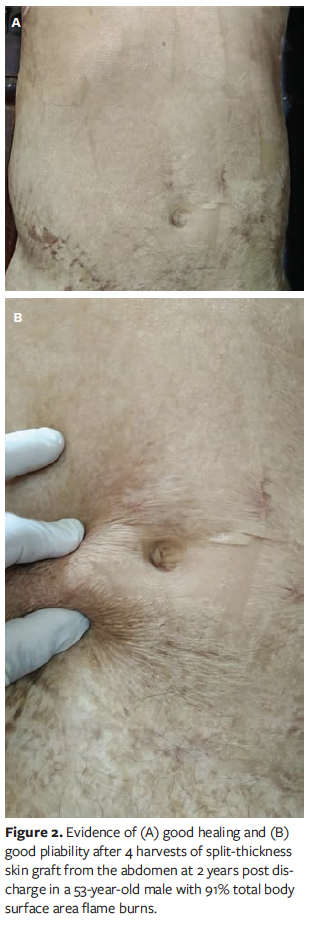
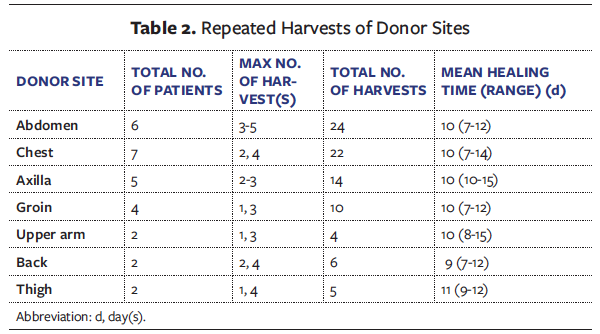
The chest and abdomen were the main sources of donor skin, followed by the axilla, groin area, upper arm, back, and thigh. The combined wound management approach allowed re-harvesting of up to 5 STSGs from the same anatomic area, especially from the abdomen. The mean donor site healing time was 10 days (range, 7-15 days) (Table 2). Despite repeated harvest of STSGs, donor sites showed good healing (Figure 2).

Representative case
A 53-year-old male was involved in an explosive burn injury and was admitted to the burns unit. He suffered extensive burns (91% TBSA) with deep partial-thickness burns on 11% of TBSA and full-thickness burns on 80% of TBSA. Non-burned skin remained on the chest, right abdominal area, right upper outer thigh, and bilateral plantar surface. During hospitalization, a total of 8 operations were performed to treat the burned skin, including 5 Meek micrograft procedures, 1 full-thickness skin graft procedure, and 2 debridements. Because of limited donor sites, STSG harvesting was repeated from the same areas, such as the chest and right abdomen. In total, 4 harvestings of STSGs were performed in the right abdominal area (interval between STSG procurement 7-11 days) and 2 harvestings in the chest within 8 to 12 days. The administration of rhGH was terminated on day 112 after admission when the burn wound was 99% closed. The patient had varying degrees of hypertrophic scarring and scar contracture on grafted areas. Despite repeated STSGs, there was good healing of donor sites without further morbidity. After 126 days of treatment in the burn unit, the patient was released to home care to be followed in the outpatient clinic (Figure 3).
Discussion
Lack of donor sites remains a challenge for achieving rapid wound closure, especially in patients with extensive burns. The modified Meek micrografting technique has become a valuable tool in the management of severe and extensive burns. When used in patients with more than 30% TBSA burns, the Meek technique allows faster wound healing, fewer surgical procedures, and a shorter LOS compared with traditional mesh grafting.14 In addition, Meek micrografting requires a smaller skin graft surface compared with mesh skin grafting.3,15 Another advantage of the Meek technique over meshed grafting is its higher clinically achievable expansion ratio.16 The Meek technique was introduced to the authors’ burns unit in 2008 and has since become the standard surgical approach for the treatment of severe burns at the authors’ institution.
In the current case series, Meek micrografting was used to cover a mean of 63% TBSA (range, 36%–80%), which is similar to the results reported in other studies. Lumenta et al17 used Meek micrografting to cover wounds of 61.7% TBSA (range, 36%–80%) in adult burn patients. Medina et al18 covered an average of 43% TBSA (range, 10%–75%) with Meek micrografting in 10 severely burned patients. The authors of the current study covered an average of 11.4% TBSA (range, 10%–30%) per procedure with Meek skin grafts. Other authors have reported similar results, with Lari and Gang19 covering an average of 16.4% TBSA (range, 15%–20%) per procedure in severely burned adolescents and adults, and Hsieh et al20 covering an average of 13.8% TBSA (range, 8%–25%) in children and adults with extensive burns.
In the current case series, the gauze backing was left in place for 10 to 14 days to prevent inadvertent graft removal with the backing, ensure graft adherence, and optimize graft take. Other providers have reported removing the gauze backing as early as 4 to 7 days after graft application, then placing cadaveric allograft to promote reepithelialization.19,21 However, an unreliable supply of allografts restricted the ability of the authors of the current study to use this strategy when needed. Furthermore, in the experience of the authors of the current study this measure seemed unnecessary, and the authors agree with Lumenta et al17 that satisfactory healing rates can be achieved with Meek grafts alone.
The mean graft take rate of 81% observed in this series is comparable with rates of 75% to 95% reported in the literature.4,19,20,22,23 Infection was the major contributing factor to graft failure in the current series, which is consistent with the findings of other published series.20,24 However, only some areas of breakdown required regrafting, which indicates that individual epithelial islands can recover after infection provided that sufficient time is allowed for recovery.22 The authors of the current study agree with previously published studies that Meek grafts tend to be less compromised and more resistant to infection compared with meshed skin grafts.17,20,25 Meshed skin grafts may be less tolerant to infection, possibly owing to the interconnecting skin bridges.20
A burn that involves more than 40% TBSA can affect the entire body. Patients with such major burns frequently experience a hypermetabolic response with increased protein catabolism, resulting in loss of lean body mass, muscle wasting, and delayed healing of the donor sites and burn wounds.7 Animal studies have shown that systemic application of rhGH promotes cellular proliferation, keratinocyte migration, granulation tissue formation, collagen synthesis, and extracellular matrix formation while decreasing the wound healing time.26-28 There is also some evidence that rhGH therapy can attenuate or reverse hypercatabolism following severe burn injuries, with such therapy resulting in accelerated protein synthesis, decreased protein catabolism, and faster healing of burn wounds and donor and/or recipient sites.7
A randomized prospective clinical study by Luo et al29 concluded that rhGH was effective in reducing donor site healing time. Other studies have shown that rhGH treatment is associated with improved wound healing and reduced hospital LOS.6 For metabolic indications, clinical treatment at a dose of 0.1 mg/kg to 0.2 mg/kg per day for a period of days to 1 year is recommended.30 Long-term treatment with rhGH is considered to be well tolerated and safe when used for approved indications and at the recommended dose.31
In the current study, the rhGH dose used was based on a previous investigation in which a plasma disappearance curve was constructed after administration of 0.1 mg/kg or 0.2 mg/kg per day.6 Other studies indicate that 0.2 mg/kg of rhGH per day can result in effective donor site healing.32 Herndon et al7 tested the effect of rhGH in patients with greater than or equal to 40% TBSA, or with 20% or more TBSA full-thickness burns. Their results indicated that donor site healing time was reduced by 2 to 4 days per 1% TBSA burn when rhGH was administered intramuscularly at 0.2 mg/kg per day. They also reported a reduction in overall LOS of 0.8 day per 1% TBSA burn. However, there was no significant difference in donor site healing time between subcutaneously administered rhGH (0.1 mg/kg/day) and placebo.
In another trial of rhGH treatment in patients with full-thickness burns covering more than 40% TBSA, Herndon et al33 reported that the mean healing time of donor sites decreased from 7.7 to 5.6 days in patients who received 0.2 mg/kg of rhGH per day. Although some experimental studies have reported that rhGH therapy induced abnormal scarring and fibrosis,34,35 de Oliveira et al reported no significant adverse effects of rhGH treatment on scar formation in humans.36 Currenttly, rhGH is an accepted option for clinical therapy of severe burn injuries.37
It is generally acknowledged that glucose metabolism can be influenced by rhGH. Published studies show that hyperglycemia was more frequent following rhGH therapy than following placebo therapy.6 In the current study, rhGH-induced hyperglycemia was observed in 5 patients. It was routinely treated with insulin to maintain a blood glucose level of between 6 mmol/L and 8 mmol/L.
EGF belongs to the group I EGF family, which is mitogenic for endothelial and epithelial cells, as well as for keratinocytes and fibroblasts. EGF has been shown to positively influence wound healing by promoting the reepithelialization and proliferation of healed dermis, increasing tensile strength, and improving wound healing overall.11,38 Brown et al39 reported that EGF improves healing quality and accelerates donor site healing.
Repeat donor site harvesting to cover extensive burns is an option when the availability of donor sites is limited. The interval between procedures may be 3 to 6 weeks depending on the patient’s condition, the thickness of the harvested skin graft, the type of dressing, and the anatomic location of the donor area.40 Acceleration of donor site healing is potentially beneficial for decreasing the time between repeat harvests, preventing wound complications such as infection and/or abnormal scarring, and shortening hospital LOS. Thus, reducing donor site healing time would enhance healing and lead to more favorable patient outcomes.30 In the experience of the authors of this study, the scalp is the most common donor area; however, it was involved in the burn injuries of all 7 cases in this study. Therefore, STSGs were also harvested from other residual areas, including the chest, abdomen, axilla, groin area, back, upper arm, and thigh.
Even small autograft remnants can be meshed into micrografts using the Meek technique. Owing to the shortage of donor sites in patients in the current study, STSGs were repeatedly harvested from the same anatomic areas. The current case series showed that re-harvesting of STSGs within 7 days (range, 7–15 days) is possible. Such wound management with good healing allowed up to 5 harvestings from the abdominal area and 4 harvestings from the chest, back, and thigh, compared with only 1 to 3 procedures following routine treatment.
In this case series, the authors’ experience using the combination technique of Meek micrografting, systemic application of rhGH, and topical application of rhEGF has been generally positive, with an average graft take rate of 81%, up to 5 re-harvestings from the same donor site without additional morbidity, complete wound healing after a mean of 120 days, a survival rate of 85.7%, and good long-term aesthetic and functional outcomes in all 6 surviving patients. The Meek micrografting technique was effective in addressing the challenge of limited skin graft donor areas. However, Meek micrografts do not achieve immediate biologic wound closure, leaving substantial areas of uncovered wound in the interstices. These denuded interstices expose patients to the dangers of open wounds, such as metabolic and/or infectious complications. Thus, the systemic application of rhGH and the topical use of rhEGF to facilitate the healing of Meek graft interstices has significant therapeutic benefit. Further experimental and clinical trials are warranted to explore the use of growth factor cocktails to promote wound closure in Meek graft interstices.
Limitations
This study has several limitations. The main limitations are the retrospective design, the small number of patients, and possible bias in the information available from medical records. Further research is needed to explore the effect of growth factor cocktails in the promotion of donor site healing and burn wound closure. Such research should include comparison of a group treated with growth factor with an untreated group, as well as comparison of a Meek technique plus growth factor group with a Meek technique only group.
Conclusions
The patients in the current case series had severe and extensive burns that were treated with a combination of simple and efficient methods for skin repair. Meek micrografting is an efficient technique that can be used in patients with burns and limited donor areas. Systemic application of rhGH and topical application of rhEGF also were used to promote healing of the burn wounds as well as the donor and recipient sites. This combined wound management approach allowed re-harvesting of up to 5 STSGs from the same anatomic area without significant morbidity. A combined treatment approach involving Meek micrografting, systemic application of rhGH, and topical application of rhEGF is a promising tool for the management of extensive burns.
Acknowledgments
Authors: Xingxin Gao, MD1; Min Zhang, MM2; Dezhi Song, MD3; Jialing Wei, MM1; Yuan Lin, MM1; Yajun Wu, MM1; Chaoyi Zhong, MM1; Dehui Li, MM1; and Bangde Xiang, MD4
Affiliations: 1Department of Burns and Plastic Surgery, First Affiliated Hospital of Guangxi Medical University, Nanning, Guangxi, China; 2Department of Critical Care Medicine, First Affiliated Hospital of Guangxi Medical University, Nanning, Guangxi, China; 3Research Centre for Regenerative Medicine, Guangxi Medical University, Nanning, Guangxi, China; 4Guangxi Medical University Cancer Hospital, Nanning, Guangxi, China
Disclosure: This work was supported financially by the National Science Foundation of China (Grant No. 81960450) and by the Health Department Fund Project of Guangxi Province (No. z20201184). The authors disclose no financial or other conflicts of interest.
Manuscript Accepted: July 27, 2023
Correspondence: Bangde Xiang, MD; Department of Hepatobiliary Surgery, Guangxi Medical University Cancer Hospital, Nanning 530021, Guangxi, China; xbd6689@163.com
References
1. Marc GJ, Margriet EB, Mashkoor AC, et al. Burn injury. Nat Rev Dis Primers. 2020;6(1):11. doi:10.1038/s41572-020-0145-5
2. Khosrow SH, Christian T, Ina N, et al. Five years experience with Meek grafting in the management of extensive burns in an adult burn center. Plast Surg. 2019;27(1):44-48. doi:10.1177/2292550318800331
3. Ottomann C, Hartmann B, Branski L, et al. A tribute to Cicero Parker Meek. Burns. 2015;41(8):1660-1663. doi:10.1016/j.burns.2015.06.013
4. Namal M, Jason W, Andrew I, Cleland H, Lo CH. Retrospective review of a tertiary adult burn center’s experience with modified Meek grafting. Burns Trauma. 2016;4:6. doi:10.1186/s41038-016-0031-2
5. Atanu B, Manish B, Craig H, et al. The micrograft concept for wound healing: strategies and applications. J Diabetes Sci Technol. 2010;4(4):808-819. doi:10.1177/193229681000400407
6. Breederveld RS, Tuinebreijer WE. Recombinant human growth hormone for treating burns and donor sites. Cochrane Database Syst Rev. 2014;9:CD008990. doi:10.1002/14651858.CD008990.pub3
7. Herndon DN, Barrow RE, Kunkel KR, Broemeling L, Rutan RL. Effects of recombinant human growth hormone on donor-site healing in severely burned children. Ann Surg. 1990;212(4):424-429. doi:10.1097/00000658-199010000-00005
8. Han G, Ceilley R. Chronic wound healing: a review of current management and treatments. Adv Ther. 2017;34(3):599-610. doi:10.1007/s12325-017-0478-y
9. Dolati S, Ahmadi M, Rikhtegar R, et al. Changes in Th17 cells function after nanocurcumin use to treat multiple sclerosis. Int Immunopharmacol. 2018;61:74-81. doi:10.1016/j.intimp.2018.05.018
10. Viana-Mendieta P, Sanchez ML, Benavides J. Rational selection of bioactive principles for wound healing applications: growth factors and antioxidants. Int Wound J. 2022;19(1):100-113. doi:10.1111/iwj.13602
11. Alemdaroğlu C, Degim Z, Celebi N, Sengezer M, Alömeroglu M, Nacar A. Investigation of epidermal growth factor containing liposome formulation effects on burn wound healing. J Biomed Mater Res A. 2008;85(1):271-283. doi:10.1002/jbm.a.31588
12. Xing G, Mei-yun T, Li G, Ai-bing X, Yue-gang L, Xiao-chuan H. Reparation of skin donor site wound using recombinant human epidermal growth factor. Chinese J Tissue Eng Res. 2010;14(5):862-865. doi:10.3969/j.issn.1673-8225.2010.05.024
13. VanGilder C, Lachenbruch CA. Air-fluidized therapy: physical properties and clinical uses. Ann Plast Surg. 2010;65(3):364-370. doi:10.1097/SAP.0b013e3181cd3d73
14. Quintero EC, Machado JFE, Robles RAD. Meek micrografting history, indications, technique, physiology and experience: a review article. J Wound Care. 2018;27(suppl 2):S12-S18. doi:10.12968/jowc.2018.27.Sup2.S12
15. Kok YO, Chong SJ, Liang WH, Tan BK, Tan KC. Revolutionizing major burns management with micrografting – improved healthcare costs, time and burns resources. Plast Reconstr Surg. 2015;136(4S):64. doi:10.1097/01.prs.0000472360.79962.7a
16. Sánchez-García A, Vanaclocha N, García-Vilariño E, Salmerón-González E, Vicente-Pardo A, Pérez-Del Caz MD. Use of the Meek micrografting technique for coverage of extensive burns: a case report. Plast Surg Nurs. 2019;39(2):44-47. doi:10.1097/PSN.0000000000000262
17. Lumenta DB, Kamolza LP, Frey M. Adult burn patients with more than 60% TBSA involved-Meek and other techniques to overcome restricted skin harvest availability: the Viennese concept. J Burn Care Res. 2009;30(2):231-242. doi:10.1097/BCR.0b013e318198a2d6
18. Medina A, Riege T, Nystad D, et al. Modified Meek micrografting technique for wound coverage in extensive burn injuries. J Burn Res. 2016;37(5):305-313. doi:10.1097/BCR.0000000000000244
19. Lari AR, Gang PK. Expansion technique for skin graft (Meek technique) in the treatment of severely burned patients. Burns. 2001;27(1):61-66. doi:10.1016/s0305-4179(00)00066-8
20. Hsieh CS, Schuong JY, Huang WS, Huang TT. Five years’ experience of the modified Meek technique in the management of extensive burns. Burns. 2008;34(3):350-354. doi:10.1016/j.burns.2007.05.005
21. Papp A, Härmä M. A collagen based dermal substitute and the modified Meek technique in extensive burns. Report of three cases. Burns. 2003;29(2):167–171. doi:10.1016/s0305-4179(02)00234-6
22. Rode H, Martinez R, Potgieter D, Adams S, Rogers AD. Experience and outcomes of micrografting for major paediatric burns. Burns. 2017;43(5):1103-1110. doi:10.1016/j.burns.2017.02.008
23. Rijpma D, Claes K, Hoeksema H, et al. The Meek micrograft technique for burns; review on its outcomes: Searching for the superior skin grafting technique. Burns. 2022;48(6):1287-1300. doi:10.1016/j.burns.2022.05.011
24. Chua AW, Khoo YC, Tan BK, Tan KC, Foo CL, Chong SJ. Skin tissue engineering advances in severe burns: review and therapeutic applications. Burns Trauma. 2016;4:3. doi:10.1186/s41038-016-0027-y
25. Zermani RG, Zarabini A, Trivisononno A. Micrografting in the treatment of severely burned patients. Burns. 1997;23(7-8):604-607. doi:10.1016/s0305-4179(97)00032-6
26. Thorey IS, Hinz B, Hoeflflich A, et al. Transgenic mice reveal novel activities of growth hormone in wound repair, angiogenesis, and myofibroblast differentiation. J Biol Chem. 2004;279(25):26674–26684. doi:10.1074/jbc.M311467200
27. Gimeno MJ, García-Esteo F, García-Honduvilla N, San Román J, Bellón JM, Buján J. A novel controlled drug-delivery system for growth hormone applied to healing skin wounds in diabetic rats. J Biomater Sci Polym Ed. 2003;14(8):821-835. doi:10.1163/156856203768366549
28. Lee SW, Kim SH, Kim JY, Lee Y. The effect of growth hormone on fibroblast proliferation and keratinocyte migration. J Plast Reconstr Aesthet Surg. 2010;63(4):e364-369. doi:10.1016/j.bjps.2009.10.027
29. Luo X, Cen Y, Yu R, et al. Effectiveness of recombinant human growth hormone treatment for severe burn injury. Article in Chinese. Hua Xi Yi Ke Da Xue Xue Bao. 2000;31(3):399-401.
30. Van Loon K. Safety of high doses of recombinant human growth hormone. Horm Res. 1998;49(suppl):78-81.
31. Allen DB, Backeljauw P, Bidlingmaier M, et al. GH safety workshop position paper: a critical appraisal of recombinant human GH therapy in children and adults. Eur J Endocrinol. 2016;174(2):P1–P9. doi:10.1530/EJE-15-0873
32. Gilpin DA, Barrow RE, Rutan RL, Broemeling L, Herndon DN. Recombinant human growth hormone accelerates wound healing in children with large cutaneous burns. Ann Surg. 1994;220(1):19-24. doi:10.1097/00000658-199407000-00004
33. Herndon DN, Hawkins HK, Nguyen TT, Pierre E, Cox R, Barrow RE. Characterization of growth hormone enhanced donor site healing in patients with large cutaneous burns. Ann Surg. 1995;221(6):649-656. doi:10.1097/00000658-199506000-00004
34. Nahas AM, Bassett AH, Cope GH, Le Carpentier JE. Role of growth hormone in the development of experimental renal scarring. Kidney Int. 1991;40(1):29-34. doi:10.1038/ki.1991.175.
35. Bowers D, McKenzie D, Dutta D, Wheeless CR, Cohen WR. Growth hormone treatment after cesarean delivery in rats increases the strength of the uterine scar. Am J Obstet Gynecol. 2001;185(3):614-617. doi:10.1067/mob.2001.117185.
36. de Oliveira GV, Sanford AP, Murphy KD, et al. Hypertrophic scar formation: a randomized controlled trial of 62 burned children. Wound Repair Regen. 2004;12(4):404-411. doi:10.1111/j.1067-1927.2004.012407.x
37. Gauglitz GG, Williams FN, Herndon DN, Jeschke MG. Burns: where are we standing with propranolol, oxandrolone, recombinant human growth hormone, and the new incretin analogues? Curr Opin Clin Nutr Metab Care. 2011;14(2):176-181. doi:10.1097/MCO.0b013e3283428df1
38. You-Hei C, Thomas LS, Yvonne NP, Robson MC, Payne WG. The use of growth factor and other humoral agents to accelerate and enhance burn wound healing. Eplasty. 2011;11:e41.
39. Brown GL, Nanney LB, Griffen J, et al. Enhancement of wound healing by topical treatment with epidermal growth factor. N Engl J Med. 1989;321(2):76-79. doi:10.1056/NEJM198907133210203
40. Malpass KG, Snelling CF, Tron V. Comparison of donor-site healing under Xeroform and Jelonet dressings: unexpected findings. Plast Reconstr Surg. 2003;112(2):430-439. doi:10.1097/01.PRS.0000070408.33700.C7