Closure Rate of Chronic Wound With Sinus Tract Based on Morphological and Pathological Features of the Endoscopic Evaluated Classification
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Wounds or HMP Global, their employees, and affiliates.
Abstract
Background. The endoscopic evaluated classification known in China as the China-Lu classification is a morphological and pathological feature-based classification for chronic wound with sinus tract (CWST). Objective. To investigate the closure rate for different types of CWST according to the endoscopic evaluated classification. Materials and Methods. This prospective case series study enrolled patients with CWST who were admitted to the Wound Healing Center of Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, China, between November 2017 and October 2021. Results. A total of 89 patients were enrolled (46 males [51.7%], 43 females [48.3%]). The CWST was classified as simple in 46 patients, morphologically complex in 13, pathologically complex in 23, and refractory in 7. After standard treatment, the overall closure rate was 86.52%. The closure rate was 97.83% for the simple type, 84.62% for the morphologically complex type, 86.96% for the pathologically complex type, and only 14.29% for the refractory type. Conclusions. The closure rate of CWST may vary by classification and may be favorable in most cases. However, a high proportion of patients with refractory wounds have a poor prognosis.
A chronic wound with sinus tract (CWST) is a complex tunneling wound connecting underlying tissue with 1 or more openings in the skin.1 Etiologically, in the majority of cases development of the sinus tract is related to direct tissue trauma or infection of the wound site (acute or chronic).2,3 Collagenopathy and iatrogenic injury have also been reported but less frequently.4,5 Surgical site infection and delayed wound healing due to inflammation often lead to the formation of multiple maze-like branches or special pathological features inside the wound that require a specific treatment approach.6,7 Moreover, the presence of multiple cyst channels poses a notable diagnostic challenge regardless of etiology.8
The traditional method of managing CWST consists of drainage therapy or surgical excision.9,10 However, there is a high rate of treatment failure (persistent inflammation or recurrence), most likely due to incomplete drainage or incomplete resection of wound tunnels.11 A percutaneous endoscopic approach was previously proposed for the diagnosis and management of tunnel wounds, including bullet channels12 and delayed wound healing after tendon suture repair.13 Despite the reported effectiveness of endoscopic management of the wound tunnel, the process is time-consuming and its application is questionable, with the published evidence limited to a few case reports.
Satisfactory results were obtained in a previous study in which endoscopy was used to observe deep sinus wounds, with the imaging examination helping the clinician fully understand the 3-dimensional shape of the sinus wound and its relationship to the surrounding organs.14 Management of the wound and supporting tissues using the endoscopic approach resulted in partial wound healing. Based on the aforementioned experience, the endoscopic evaluated classification for CWST (ie, the China-Lu classification) was proposed.15
The present case series was conducted to further explore the differences in closure rate between different types of CWST according to the morphological and pathological features of the endoscopic evaluated classification.
Materials and Methods
Study design and participants
This prospective case series study was conducted at the Wound Healing Center of Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, China, between November 2017 and October 2021. Patients with chronic sinus wounds in the form of a duct or cavity with an opening on the mucosal surface of the skin that did not properly heal within 30 days were included, regardless of age or sex. Patients with a trauma diameter less than 2.7 mm (limited by the diameter of the endoscope) and patients with certain diseases who could not be examined or treated endoscopically were excluded.
The research adhered to the Declaration of Helsinki and was approved by the Ethics Committee of Ruijin Hospital, and written informed consent was obtained from all patients. In this study, the cost of the therapy was paid for by the national health insurance program in China.
Procedures
At the beginning of the present study, all patients underwent computed tomography (CT) examination and endoscopy to assess wound status (Figure 1A). A 1:50 dilution of contrast agent was injected into the sinus tract and left for 3 minutes to allow the contrast agent to fill all branches for CT imaging. The resulting images were measured using the supporting software for the CT equipment, and information such as the number of branches and whether there was bony involvement was recorded. A hard endoscope was then inserted into the sinus wound to observe and record the deep parts. Special features were recorded, such as exudation, foreign bodies, necrosis, and involvement of the periosteum.
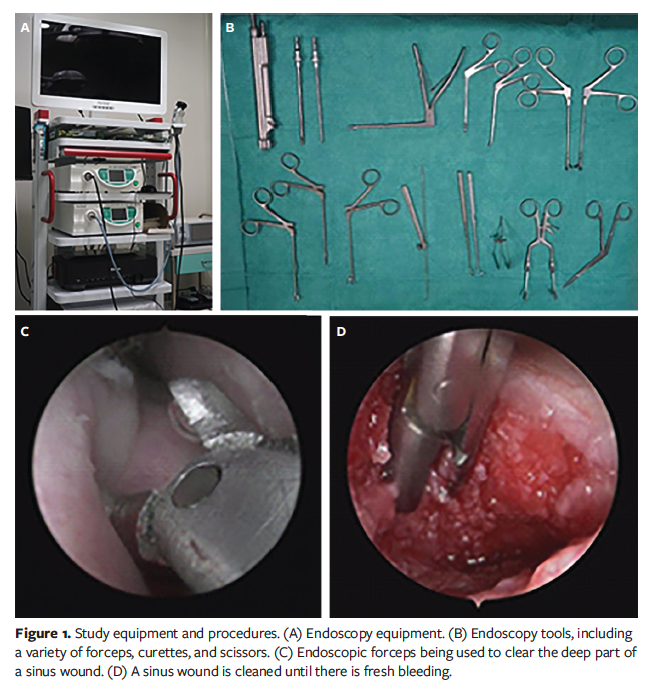
Standard treatment of sinus tract wounds, such as wound debridement, packing, and drainage, was performed using endoscopy and special tools for endoscopy (Figure 1B). Specifically, for fibrotic and necrotic tissue, a curette was used to scrape out the tissue; for particularly hard tissue, endoscopic special forceps were used to remove the fibrous tissue out of the sinus tract; for exudation, a long syringe was used to perform a high-pressure flush and place a drain; and for foreign bodies, such as surgical sutures, endoscopic special scissors were used to snip them off, after which the endoscopic special forceps were used to remove the foreign bodies. All of these operations were performed endoscopically. Although negative pressure wound therapy (NPWT) has been a standard treatment, drainage materials often cannot be placed in all of the sinus tract trauma, especially in more complex sinus tracts. In the present study, NPWT was not used; instead, gauze was used in cases in which drainage was needed. Local anesthesia was administered with topical lidocaine ointment prior to this type of procedure. During the treatment, most patients did not feel significant pain or discomfort.
All special morphological and pathological features of the wounds were documented and photographed for the patient’s record (Figure 1C, 1D). Closure was defined as the formation of fibrous connection in the sinus tract or sinus cavity with disappearance of the original cavity and closure of the opening in the skin or mucosal surface.
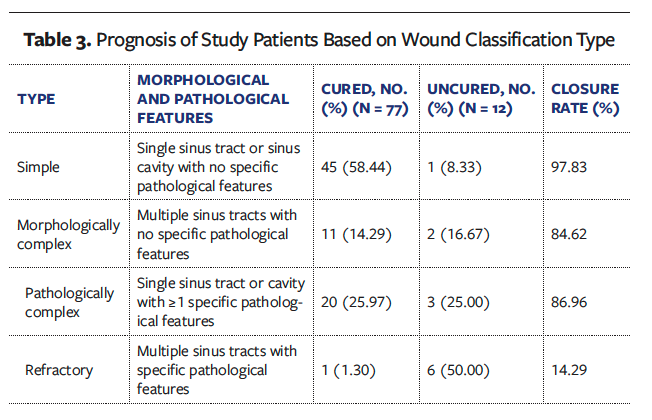
All wounds were classified according to the endoscopic evaluated classification.15 A wound with a single sinus tract or sinus cavity and no special pathological features was classified as simple, a wound with multiple sinus tracts with no special pathological features was classified as morphologically complex, the presence of 1 or more special pathological features in a single sinus tract or sinus cavity (eg, fibrosis, exudate accumulation, foreign bodies, necrotic tissue) was classified as pathologically complex, and a wound with multiple sinus tracts with special pathological features was classified as refractory.
Statistical analysis
All data were analyzed using SPSS version 21.0 (IBM Corporation). Continuous data were expressed as mean (SD), and the categorical data were presented as number (percentage). Only descriptive statistics were used.
Results
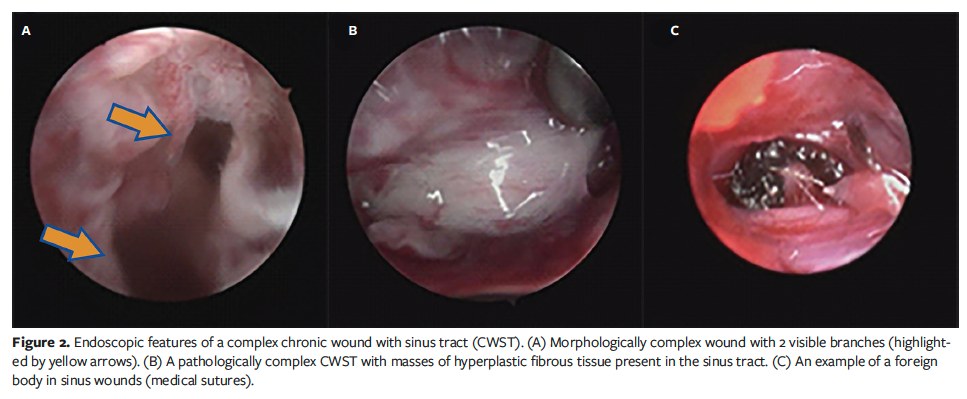
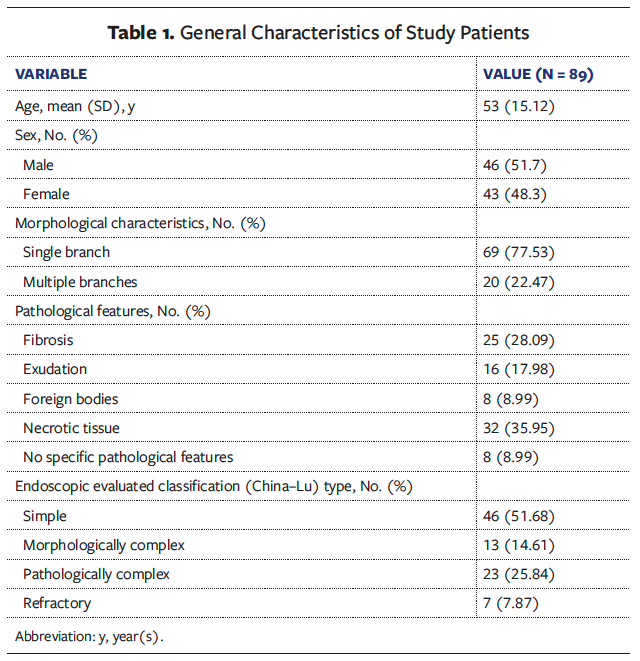
A total of 89 cases of CWST were included, with an average patient age of 53 years (range, 21 years–82 years). There were 46 male patients (51.7%) and 43 female patients (48.3%). Of the total 89 patients, 69 (77.53%) had a single branch wound tunnel and 20 (22.47%) had a wound tunnel with multiple branches. Twenty-five patients (28.09%) had wound fibrosis, 16 (17.98%) had exudation, 8 (8.99%) had foreign bodies in the wound tunnel, 32 (35.95%) had necrotic tissue, and 8 (8.99%) had no special pathological features. Based on morphological and pathological features of the wounds, 46 patients had simple wounds, 13 had morphologically complex wounds (Figure 2A), 23 had pathologically complex wounds (Figure 2B, 2C), and 7 had refractory wounds (Table 1).
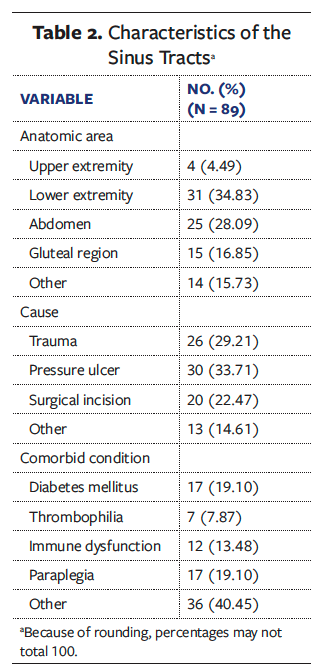
Of the 89 cases, 4 were located in the upper extremity, 31 in the lower extremity, 25 in the abdomen, 15 in the gluteal region, and 14 in other anatomic areas. The cause was trauma in 26 cases, pressure ulcers in 30 cases, surgical incisions in 20 cases, and other in 13 cases. All 89 patients had a comorbidity: 17 had diabetes mellitus, 7 had thrombophilia, 12 had immune dysfunction, 17 had paraplegia, and 36 had other conditions (Table 2).
After the 45-day follow-up period, the chronic wound was closed in 77 of 89 patients (overall cure rate, 86.52%). The closure rate was 97.83% for simple wounds, 84.62% for morphologically complex wounds, 86.96% for pathologically complex wounds, and 14.29% for refractory wounds (Table 3).
Discussion
This case series explores the prognosis of different types of CWST per the endoscopic evaluated classification, which is based on morphological and pathological features. The closure rate of CWST varies by type and is particularly low in patients with the refractory type. It is hoped that this study will help increase understanding of CWST in clinical practice.
According to outpatient data at the wound treatment center of the authors of the present study, chronic sinus wounds are relatively rare but are rising in prevalence. During the 4-year period of the present study, there were 89 cases of CWST at the authors’ institution. To the best of the knowledge of the authors of the present study, this study is the first to apply wound endoscopy in a relatively large sample and report the distinctive characteristics of different wound types. The majority of previously reported data on such chronic wounds are limited to case reports without any commonly accepted morphological or pathological classification to serve as the basis of diagnosis and management. In the present study, a cohort of patients with CWST were recruited to address this question, and the 4 wound types with distinctive features are described according to the endoscopic evaluated classification: simple, morphologically complex, pathologically complex, and refractory.
Based on the experience of the authors of the present study and on previously published data,8,15,16 it was hypothesized that the presence of a single or multiple wound tunnels and special pathological features are the key factors affecting the healing of chronic sinus wounds. Therefore, complex morphology and special pathological features are negative factors for wound closure. The complexity of wound morphology and wound presentation are the 2 main dimensions for wound evaluation, which confirmed the applicability of a 2-dimensional classification.
As noted previously, a simple wound has a simple morphology (ie, single sinus tract or sinus cavity) with no special pathological features. The structure of the sinus wound and the condition of the wound are relatively simple and easy to observe and treat, so the closure prognosis is relatively good. One study demonstrated the benefits of applying the endoscopy technique (using a choledochoscope) for this type of wound.17 In the present study, in 45 of 46 patients with a simple CWST, the wound was fully closed after 45 days—a cure rate of 97.83%, compared with the overall closure rate of 86.52%.
The morphologically complex wound is characterized by multiple branches, but it lacks special pathological features. The prognosis may be worse for this type of wound due to the limited treatment scope; the metal rod lens of the rigid endoscope or specialized tools may not reach branches that are too angled from the main wound tunnel. In the present study, the prevalence of the morphologically complex wound type was comparatively low (13 of 89), and the closure rate was 84.62%.
Pathologically complex wounds are characterized by the presence of 1 or more special pathological features (eg, fibrosis, exudate accumulation, foreign bodies, necrotic tissue) in a single branch sinus. Because of the limits of endoscopic instruments used in the present study, adequate removal of some pathological features (eg, fibrous lamina) was challenging, and this may be a reason closure was not achieved in some pathologically complex wounds.4,18
A refractory wound is a multibranch sinus wound with special pathological features. Although the total number of such wounds is small, the closure rate was less than 15% in the present study. Refractory wounds are the most complex type of chronic sinus wounds. Analysis of patients in the present study indicates that comorbidities are the main reason for the low closure rate of such wounds.
The aforementioned results suggest that with increased morphological complexity and the presence of various special pathological features, there is a corresponding decrease in the closure rate of sinus wounds, especially in patients who exhibit both factors. Complex sinus tracts with multiple branches may have insufficient drainage of some areas, and some branches with a large angle to the main trunk cannot be cleared; some unique pathological factors in the sinus tract may be difficult to remove entirely. These results are in line with the widely applied theory of wound closure, which states that negative factors may stop the normal repair process of chronic wounds resulting from insufficient drainage, foreign body rejection, or biofilm formation.19
In addition, the previously discussed difficulty managing sinus wounds is based on the fact that the deep part of the wound is hidden in the subcutaneous tissue and is difficult to visualize.17,20 Since 2018, the Wound Healing Center has used a rigid endoscope to observe sinus wounds and has performed an imaging examination after filling the cavity with a contrast agent to clarify the number of branches of the sinus tract and the relationship between the sinus tract and surrounding tissues or organs. This approach, which is based on the best practice recommendations framework for wound assessment proposed by Keast et al16 in 2004, has been proven to be quite effective in endoscopic therapy with matching tools to clear the sinus wound, especially for the deep part of the tract. In a 2019 study, several of the authors of the current case series reported that endoscopy methods aided in obtaining more comprehensive information on the wound and applying more precise treatment.15 However, some sinus wounds described in the present study still did not close as expected. After analyzing the conditions of these wounds, the authors of the present case series found that they were either quite complex in shape or had several special pathological features—such as foreign bodies, massive exudate or empyema, or fibrous lamina—which is in line with previous observations.15 These wounds were categorized as refractory, and the closure rate was lowest in this group. Patients with refractory wounds required surgical excision and reconstruction. However, currently available endoscopic equipment and supporting tools have performance defects that render them insufficient to meet the requirements of either excision or reconstruction. Improved equipment and supporting tools are needed to achieve precise and minimally invasive endoscopic surgical management of refractory sinus tract wounds, with the goal of improving closure rates.
Limitations
This study has some limitations. It is a case series, and although the sample size was large enough, it was not powered to evaluate for statistically significant differences between groups. In addition, the results demonstrate the experience of a single center; wound endoscopy has a comparatively long learning curve, which may influence treatment results. Finally, this study did not take etiology into account, which in some cases may affect the closure process. Despite these limitations, the study demonstrates the benefits and necessity of the sinus wound classification discussed, which can serve as the basis for larger-scale research and clinical practice in the future.
Conclusion
The closure rate of CWST may vary by classification, with a high proportion of refractory wounds exhibiting a poor prognosis. The endoscopic evaluated classification, known in China as the China-Lu classification, may help clinicians understand the key points and difficulties of the wound morphology and pathology, correctly evaluate the complexity of the sinus disease, and formulate treatment strategies. Multicenter studies with large sample sizes are needed to confirm these findings.
Author and Public Information
Authors: Xian Ma, PhD; Yakupu Aobuliaximu, MS; Di Zhang, PhD; Yiwen Niu, PhD; Jiajun Tang, PhD; Yingkai Liu, PhD; Mingjie Wu, PhD; Lifang Huang, BS; Jingqi Zhou, MS; Fangyi Wu, BS; Chunlan Wang, BS; Jiaoyun Dong, PhD; Ming Tian, PhD; Fei Song, BS; Xiaozan Cao, BS; Yong Lu, PhD; Hanqi Wang, PhD; and Shuliang Lu, PhD
Affiliations: Wound Healing Center, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai 200025, China
Author Contributions: X.M., S.L., and Y.A. carried out the studies, participated in data collection, and drafted the manuscript. D.Z., Y.N., J.T., Y.L., M.W., L.H., J.Z., F.W., C.W., and J.D. analyzed data. M.T., F.S., X.C., Y.L., and H.W. performed the statistical analysis and participated in its design. All authors read and approved the final manuscript.
Disclosure: The authors disclose no financial or other conflicts of interest.
Ethics: The research followed the Declaration of Helsinki guidance and was approved by the Ethics Committee of Ruijin Hospital, and written informed consent was obtained from all patients. All methods were performed in accordance with the relevant guidelines and regulations.
Correspondence: Shuliang Lu, PhD; Wound Healing Center, Shanghai Jiao Tong University Medical School Affiliated Ruijin Hospital, Shanghai 200025, China; 13901738685@139.com
Manuscript Accepted: May 24, 2024
References
1. Bowers S, Franco E. Chronic wounds: evaluation and management. Am Fam Physician. 2020;101(3):159-166.
2. Hoversten KP, Kiemele LJ, Stolp AM, Takahashi PY, Verdoorn BP. Prevention, diagnosis, and management of chronic wounds in older adults. Mayo Clin Proc. 2020;95(9):2021-2034. doi:10.1016/j.mayocp.2019.10.014
3. Andrews KL, Derby KM, Jacobson TM, Slevers BA, Kiemele LJ. Prevention and management of chronic wounds. In: Braddom’s Physical Medicine and Rehabilitation. Elsevier; 2021:469-484.e4. doi:10.1016/B978-0-323-62539-5.00024-2
4. Bellingeri A, Falciani F, Traspedini P, et al. Effect of a wound cleansing solution on wound bed preparation and inflammation in chronic wounds: a single-blind RCT. J Wound Care. 2016;25(3):160-168.
5. Martinengo L, Olsson M, Bajpai R, et al. Prevalence of chronic wounds in the general population: systematic review and meta-analysis of observational studies. Ann Epidemiol. 2019; 29: 8-15. doi:10.12968/jowc.2016.25.3.160
6. Teixeira PA, Sousa PA, Coimbra M. Computer vision challenges for chronic wounds assessment. 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC); 2020:1840-1843. doi:10.1109/EMBC44109.2020.9175713
7. Ngo QC, Ogrin R, Kumar DK. Computerised prediction of healing for venous leg ulcers. Sci Rep. 2022;12:17962.
8. Li S, Mohamedi AH, Senkowsky J, Tang L. Imaging in chronic wound diagnostics. Adv Wound Care (New Rochelle). 2020;9(5):245-263. doi:10.1089/wound.2019.0967
9. Sequeira JB, Coelho A, Marinho AS, Bonet B, Carvalho F, Moreira-Pinto J. Endoscopic pilonidal sinus treatment versus total excision with primary closure for sacrococcygeal pilonidal sinus disease in the pediatric population. J Pediatr Surg. 2018;53(10):2003-2007. doi:10.1016/j.jpedsurg.2018.02.094
10. Las Heras K, Igartua M, Santos-Vizcaino E, Hernandez RM. Chronic wounds: current status, available strategies and emerging therapeutic solutions. J Control Release. 2020;328:532-550. doi:10.1016/j.jconrel.2020.09.039
11. Kehoe A, Elmore MF. Woundoscopy: a new technique for examining deep, nonhealing wounds. Ostomy Wound Manage. 2002;48(4):30-33.
12. Kravtsov MN, Manukovsky VA, Bulyshchenko GG, Mirzametov SD, Byvaltsev VA. Case report: full-endoscopic surgery for bullet wounds of the spine: a report of three cases. Front Surg. 2022;9:873365. Published 2022 Mar 25. doi:10.3389/fsurg.2022.873365
13. Yang YP, Chen HY, Cui GQ, et al. Endoscopic surgery for delayed wound healing after achilles tendon suture repair: a report of three cases. Orthop Surg. 2021;13(3):1126-1131. doi:10.1111/os.12995
14. Tang JJ, Lu SL, Ma X, et al. [Application value of endoscope in probing chronic wound with sinus tract in clinic]. Zhonghua Shao Shang Za Zhi. 2018;34(6):365-369. doi:10.3760/cma.j.issn.1009-2587.2018.06.010
15. Ma X, Tang JJ, Wu MJ, et al. [Diagnosis and treatment standard for treatment with endoscopy technique in chronic wounds with sinus tract (trial version)]. Zhonghua Shao Shang Za Zhi. 2019;35(12):833-838. doi:10.3760/cma.j.issn.1009-2587.2019.12.001
16. Keast DH, Bowering CK, Evans AW, Mackean GL, Burrows C, D’Souza L. MEASURE: A proposed assessment framework for developing best practice recommendations for wound assessment. Wound Repair Regen. 2004;12(3 Suppl):S1-S17. doi:10.1111/j.1067-1927.2004.0123S1.x
17. Wang H, Dou X, Hu X, Yu J, Wang S. Effectiveness and safety of endoscopy for treatment of surgical site infection: a randomized control trial. Exp Ther Med. 2014;8(6):1727-1730. doi:10.3892/etm.2014.2028
18. Diegelmann RF, Evans MC. Wound healing: an overview of acute, fibrotic and delayed healing. Front Biosci. 2004;9:283-289. doi:10.2741/1184
19. Wilkinson HN, Hardman MJ. Wound healing: cellular mechanisms and pathological outcomes. Open Biol. 2020;10(9):200223. doi:10.1098/rsob.200223
20. Choi EJ, Kim SY, Kim HG, Shon HS, Kim TK, Kim KH. Percutaneous endoscopic debridement and drainage with four different approach methods for the treatment of spinal infection. Pain Physician. 2017;20(6):E933-E940.