



Comparison of Wound Surface Area Measurements Obtained Using Clinically Validated Artificial Intelligence-Based Technology Versus Manual Methods and the Effect of Measurement Method on Debridement Code Reimbursement Cost
Abstract
Background. Evidence shows that ongoing accurate wound assessments using valid and reliable measurement methods is essential to effective wound monitoring and better wound care management. Relying on subjective interpretation in measuring wound dimensions and assuming a rectilinear shape of all wounds renders an inconsistent and inaccurate wound area measurement. Objective. The authors investigated the discrepancy in wound area measurements using a DWMS versus TPR methods and compared debridement codes submitted for reimbursement by assessment method. Methods. The width and length of 177 wounds in 56 patients were measured at an outpatient clinic in the United States using the TPR method (width × length formula) and a DWMS (traced wound dimensions). The maximal allowable payment for debridement was calculated for both methods using the reported CPT codes based on each 20-cm2 estimated surface area. Results. The average wound surface area was significantly higher with the TPR method than with the DWMS (20.20 and 12.81, respectively; P = .025). For patients with dark skin tones, ill-defined wound edges, irregular wound shapes, unhealthy tissues, and the presence of necrotic tissues, the use of the DWMS resulted in significantly lower mean differences in wound area measurements of 14.4 cm2 (P < .008), 8.2 cm2 (P = .040), 6.8 cm2 (P = .045), 13.1 cm2 (P = .036), and 7.6 cm2 (P = .043), respectively, compared with the TPR method. Use of the DWMS for wound surface area measurement resulted in a 10.6% lower reimbursement amount for debridement, with 82 fewer submitted codes, compared with the TPR method. Conclusions. Compared with the DWMS, TPR measurements overestimated wound area more than 36.6%. This overestimation was associated with dark skin tones and wounds with irregular edges, irregular shapes, and necrotic tissue.
Abbreviations
AI, artificial intelligence; ANOVA, analysis of variance; BMI, body mass index; CI, confidence interval; CPT, Current Procedural Terminology; DWMS, digital wound management solution; FDA, US Food and Drug Administration; SD, standard deviation; TPR, traditional paper ruler.
Introduction
In clinical practice, a paper ruler is the most commonly used method to determine wound area measurements, because it is usually thought to be the most inexpensive and easy-to-adopt method.1 With this traditional, manual method of wound measurement, clinicians use different techniques to determine the width and length of wounds.1 Typically, clinicians measure the most extended length and most extended width of a wound, with or without a perpendicular alignment to each other, and adhering to either head-to-toe or side-to-side orientation.¹ In general, when using this method, clinicians usually calculate the wound surface area by multiplying the width and length of the wound.2,3 The major drawback of multiplying these 2-dimensional measurements is the assumption that all wounds fit a rectangular model, which is not the case.3
Evidence shows that ongoing accurate wound assessments using valid and reliable measurement methods is essential to effective wound monitoring and better wound care management.4 Relying on subjective interpretation in measuring wound dimensions and assuming that all wounds are rectilinear renders inconsistent and inaccurate wound area measurements.1 Evidence shows that the estimated area using the formula fitted for a rectangular model is always higher than the actual area measurement, especially for irregularly shaped and large wounds.3 For example, Langemo et al5 conducted a comparative study using 3 plaster wound models to evaluate the accuracy of wound area measurements using the different techniques of manual assessment when applying the 2-dimensional multiplication rule to different wound shapes. The authors reported an overestimated area measurement of 36% in L-shaped, 74% in pear-shaped, and 39% in circle-shaped wounds. Another study verified this finding.6 Those authors compared wound area measurements of 10 circular and oval wounds using the standard manual multiplication rule (length × width) with area measurements calculated using a specialized planimetric camera and reported a 40% overestimation of area measurements using the linear multiplication rule.6
Another method to calculate wound surface area is to place transparency film over a wound and trace the wound perimeter, and then place the tracing over graph paper to count the squares to determine the surface area. This is a more accurate and reliable method than standard multiplication of length by width to calculate wound surface area.3 However, the tracing method is tedious and time-consuming, especially for larger wounds. It can take up to 10 minutes to calculate a 70-cm² wound.7
With the recent advancements in wound care technology, especially those that integrate AI and machine visioning for more accurate and robust assessment techniques, the gathering of wound measurements and wound data collection are becoming more reliable and efficient. A growing evidence base indicates that digital wound assessment tools are a quick, accurate way to measure wounds.3,6,8,9
Noninvasive wound assessment technology that captures high-precision wound images and measurements integrates machine visioning and machine learning technologies to enhance data collection and analysis. This capability enables automatic calculation of the surface area of any wound of any size and shape, regardless of patient positioning or degree of lighting.9,10
For example, Wang et al9 used 15 photos of 15 plastic wound models (Pressure Injury Staging Model, Wilma Wound Foot, and Seymour II Wound Care Model; VATA Inc) to assess the accuracy of repeated measurements of wound surface area using a skin and wound care smartphone application compared with standardized digital planimeter (Placom KP-90N, Koizumi Sokki Mfg Co Ltd). The study reported high accuracy and reliability of the Swift Wound mobile application (Swift Medical) (intraclass correlation coefficient, 0.998 [95% CI, 0.996–0.999]) comparable to the standardized digital planimeter.
In contrast to the traditional manual methods, digital wound care technology has additional features not attainable with standard methods, such as the ability of color calibration to adjust for varying light conditions and different skin colors to guide the segmentation process.11,12 Owing to perspective changes, inflammation, and discoloration of the skin with uncontrolled lighting conditions and patient positioning, wound assessment varies markedly with each traditional examination.13,14 Determining a relationship between the constitutive skin color and accurate wound measurement may be helpful in successfully monitoring wound healing across different levels of skin pigmentation.15 However, knowledge remains limited regarding different skin tones and the level of accuracy of wound measurements. Therefore, a basic understanding of any association between skin color and level of accuracy of wound area measurement by method is of interest.
Moreover, digital technology in wound care uses edge enforcement and automatic threshold adjustment to accurately measure wounds with detected anomalies. For example, a retrospective study that assessed the technology’s accuracy in assessing wounds with the symptoms of swelling, granulation, infection, and necrosis reported 87.3% accuracy.16 According to another study, digital photo planimetry software was found to be more accurate and reliable than traditional manual methods for large, irregular wounds with epithelial islands. The study reported a 10% higher inter-rate reliability and accuracy with the use of digital photo planimetry software.17
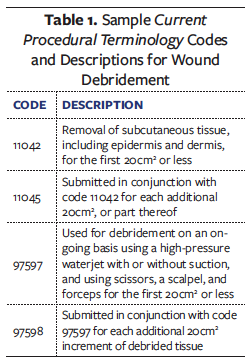
In addition to properly assessing wounds, another essential factor in promoting wound healing is preparing the wound for epithelialization. Debridement of nonviable tissues within wounds to remove biofilm, bioburden, and senescent cells is recommended.18,19 Physicians report on debridement procedures using many different CPT codes. An example of submitted CPT codes and their descriptions is listed in Table 1.20 A descriptive study was conducted in the United States to assess the trend in debridement reimbursements from 2012 to 2017.20 The study reported a 32% increase in debridements submitted for reimbursement, which resulted in a 24% increase in expenditure for these procedures from 2012 to 2017, a $24 950 230 increase.
Despite recent advances in and adoption of machine learning in clinical settings, little has been published on the discrepancy of area measurements between manual methods and digital methods, specifically with a large sample size of different wound types, shapes, and sizes in real-world settings. It is imperative to quantify the overestimation of wound area measurement using manual methods to avoid extra payment associated with the debridement procedures, especially with the increased use of debridement codes.
The current quality improvement study investigated the discrepancy in wound area measurements between manual TPR and digital wound care assessment methods in a real-world environment. The study also assessed the effect of different wound characteristics on area measurements using the digital, AI-based wound care application versus the manual TPR method. In addition, the study compared the proportion of debridement codes submitted for reimbursement and the payment rates by assessment method using the reported CPT codes for each 20-cm2 estimated surface area.
Methods
Study design and setting
This descriptive, quality improvement study was conducted at Abrazo West Campus Wound Care Clinic (Abrazo Clinic) in Arizona, United States, to analyze discrepancies in surface area measurements, debridement codes, and the associated reimbursement rates for each wound by the assessment method used. Wound assessment data were collected using a TPR versus the DWMS (Swift Skin and Wound mobile application [hereafter DWMS or mobile application]; Swift Medical).
The clinic has operated since 2011, with 6 rooms and 3 hyperbaric chambers offering wound care services. The outpatient wound clinic accepts all types of wounds, including but not limited to diabetic, venous stasis, and arterial ulcers; pressure injuries; surgical wounds; traumatic wounds; skin tears; blisters; and burns through referrals from hospitals, emergency centers, and primary care and specialty physician offices.
Data sources
The primary author (M.C.A.), an internal medicine physician at the clinic, assessed the wounds of patients referred to the clinic in May 2022. That physician measured the width and length of each wound during the wound assessment session using the TPR method and the DWMS. For the TPR method, the maximum head-to-toe length and greatest width measurements (perpendicular to the length) of each wound were documented. The surface area was calculated by multiplying the greatest width by the most extended length of the wound.¹ Per the standardized protocol, the clinician ensured consistency and accuracy in documenting wound images by following a strict procedure for lighting and backdrop. The clinician used consistent and adequate natural or evenly distributed artificial lighting to ensure clear visibility of the wound. Additionally, a plain, non-distracting background was used to provide clarity, with a clear view of the wound bed.
The physician then repeated the assessment on the same wounds during the same wound evaluation session using the DWMS. The digital application uses the smartphone’s built-in digital camera guided by the FDA-registered HealX (Swift Medical) fiducial marker, which is a small sticker that is placed beside the wound as a point of reference when capturing wound images. Only the wounds are visible; neither patients’ faces nor any other anatomic areas are captured as part of the assessment. The AI within the application autonomously identifies and traces the wound edges in the image; however, the clinician can adjust these edges to determine the final area of interest. The application software then automatically calculates the clinically validated measurements (length and width). Length is, by default, the maximum distance across the wound, and the maximum width is captured perpendicular to the length. After recording the length and width measurements of the wound, the digital application automatically calculates the actual wound surface area using the boundaries of the wound edges rather than the maximum length and width.
In addition, the DWMS automatically assigns a study image identification number (proprietary code) to each captured wound image, which is used as a study identification number for each wound evaluation included in the study. The captured images with the assigned Swift codes are available through an online interface (dashboard) that is accessible only to the study investigators. Other non-image data, such as time of evaluation, wound type, wound location, patient age and sex, and wound dimensions (length, width, and surface area) are also available and are automatically uploaded to the dashboard.
The DWMS is designed to adhere to industry best practices. It complies with all applicable industry standards in the jurisdictions in which it operates, such as the Personal Information Protection and Electronic Documents Act (Canada), Personal Health Information Protection Act (Ontario, Canada), Health Insurance Portability and Accountability Act (United States), and the Medical Device Single Audit Program (Australia, Brazil, Japan, Canada, United States) as per FDA standards.
Assessment of patients’ wounds was part of routine wound care provided at the clinic. Wound measurements did not involve any particular intervention or preparation other than the usual techniques for wound assessment and did not affect the standard wound care provided to patients. The institutional director approved the study protocol. The study protocol complies with the principles of the Declaration of Helsinki for human subject research. This is a noninterventional quality improvement study and therefore was exempt from the need for approval by an institutional review board.
Patients were informed that their wound images using the digital application would be taken, and that their wound measurements would be documented using both methods for study tracking purposes. Wound measurements and assessment information were documented in an Excel (Microsoft Corp) spreadsheet only when the patient consented verbally and was comfortable with sharing the unidentifiable information.
Data collection process
The primary author assessed wounds and recorded measurement data in the spreadsheet using the TPR method and the digital application. Wound measurements were recorded for eligible patients 18 years or older with active wounds, including diabetic, venous, and arterial ulcers, pressure injuries, surgical wounds, skin tears, abscesses, and traumatic wounds.
A total of 177 active wounds in 56 patients referred to the center during the study period were assessed using both manual and digital methods. Wound assessments were carried out over 1 month, starting May 1, 2022.
As stated previously, for each patient the physician first assessed wounds using a TPR method. The clinician then recorded in the spreadsheet the patient’s age, sex, number of wounds for each patient; date of assessment; wound width, length, and depth in centimeters; surface area (length × width); height in centimeters; weight in kilograms; BMI; wound type; and anatomic location.
Using the DWMS for the digital planimetry application, the physician captured an image of the same wound, then recorded the Swift code in the spreadsheet. The automatically measured wound length, width, and depth, as well as the automatically calculated surface area were extracted by a different researcher (H.T.M.) from the dashboard and added to the spreadsheet in columns adjacent to those containing each patient’s manually collected wound data.
The physician also recorded any debridement codes (surgical and selective) for each wound, using the reported CPT codes 97597, 97598, 11042, and 11045. The number of submitted codes and payment rates linked to each claimed code were also recorded based on each 20 cm2 of surface area calculated using both manual and digital methods. The maximum amount that can be paid for debridement services was determined by calculating the Medicare national average payment for the Medicare Physician Fee Schedule, based on the CPT codes in 2022 for such services provided in a non-facility setting.
Another study investigator (R.D.F.) reviewed the captured images on the application dashboard and recorded the following information in the same spreadsheet for each wound guided by the proprietary code ID: skin color tone (dark, olive moderate Brown, medium White, White fair), type of wound edges (diffuse, rolled, well defined), wound shape (regular, irregular), type of surrounding tissues (healthy, not healthy), and the presence or absence of necrotic tissue (absent; minimal, <25%; moderate, 25%-75%; excessive, >75%).
Statistical analysis
Data analysis was performed using SPSS (version 28; IBM Corp). The descriptive analysis was generated from numeric (age) and categorical (sex and wound characteristics, including the type of wound, skin tone, wound shape, defined wound edges, presence of necrotic tissues, and status of surrounding tissue) variables. The summary of findings was displayed as frequencies and mean ± SD.
Additionally, bivariate analyses were conducted. A paired sample t test was used to examine whether there was a mean difference in wound measurements (length, width, depth, and surface area) using a traditional manual method versus the digital application.
Two-way ANOVA tests were performed to determine the effects of interaction between each wound’s characteristics and the assessment method (manual vs. digital) on wound area measurements. Subgroups were created for wound edge (defined vs. ill-defined) and necrotic tissues (absent vs. present).
Data are presented as mean ± SD. Residual analysis was performed to test for the assumption of the 2-way ANOVA. Outliers were assessed by inspection of a box plot, normality was assessed using the Shapiro-Wilks normality test, and the Levene test was used to assess homogeneity of variances. All pairwise comparisons were run for each simple main effect with reported 95% CI and P value, with P less than .05 considered statistically significant for each simple main effect. An analysis of the simple main effect of the nominal variable (skin tone) was performed using a Bonferroni adjustment, with P less than .0125 considered statistically significant.
The total cost of wound care debridement was calculated using the reported CPT codes 97597, 97598, and 11042 through 11045 based on each 20-cm2 area.
Results
Overall wound characteristics assessed using manual and digital methods
A total of 56 patients were assessed for the study (30 females [53.6%], 26 males [46.4%]). Patient age ranged from 29 years to 89 years (mean, 64 years). Patient height ranged from 147.3 cm to 190.5 cm (average, 169.0 cm) and weight ranged from 40.9 kg to 203.6 kg (mean, 93.4 kg). BMI values were between 17 and 68.3 (average, 32.5, which falls in the obese range).
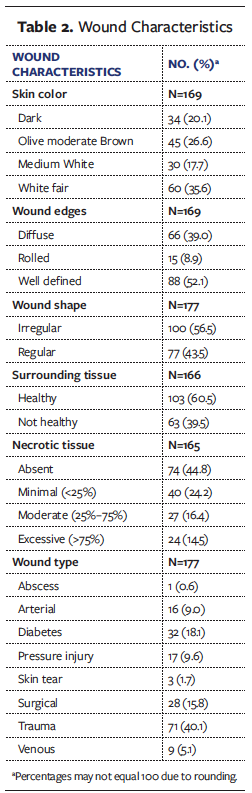
A total of 177 measurements were captured of a wide range of wound types. Of the total measurements, 71 (40.1%) were of traumatic wounds and 32 (18.1%) were of diabetic ulcers. In terms of wound characteristics, 56.5% of wounds had an irregular shape, 47.9% did not have a well-defined edge, and 55.1% were surrounded by necrotic tissues (Table 2).
Comparison of repeated wound measurements using manual and digital methods
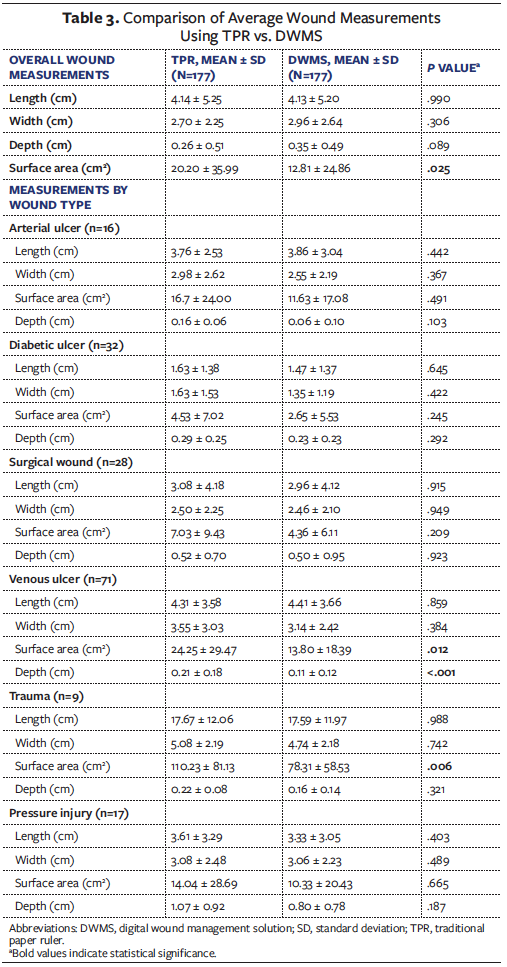
Overall wound length, width, depth, and surface area measurements by method of measurement are noted in Table 3. No significant differences were reported between wound length, width, or depth measurements using the manual method compared with the digital application. However, a significant difference was reported between the average wound surface area calculation using the manual length by width multiplication method compared with the digital technology (20.20 and 12.81, respectively; P = .025).
The calculated mean wound surface area was consistently higher with the manual method than the digital method. A significant difference in surface area by evaluation method was detected for traumatic wounds (TPR, 110.23 cm2 ± 81.13 vs. DWMS, 78.31 cm2 ± 58.53; P = .006) and venous ulcers (TPR, 24.25 cm2 ± 29.47 vs. DWMS, 13.80 cm² ± 18.39; P = .012) (Table 3).
Two-way ANOVA test and assessment of wound criteria on wound area measurements using different assessment methods
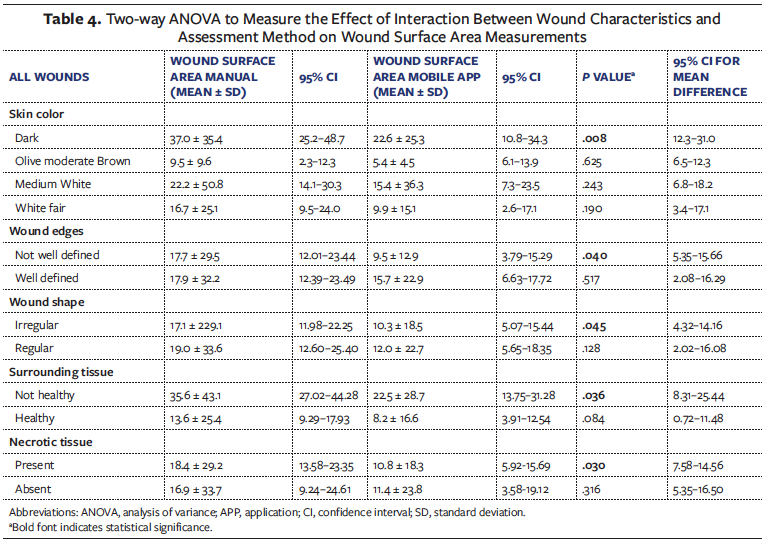
A 2-way ANOVA test was conducted to examine the effects of skin tone and assessment method on wound area measurements (Table 4). The analysis of simple main effects for skin tone using different assessment methods was performed. For wounds in patients with dark skin tones, use of the mobile application was associated with an estimated marginal mean for wound area measurement of 22.6 cm2 (95% CI, 10.8-34.3), which was a mean difference of 14.4 cm2 smaller than with the TPR method (37.0 cm2; 95% CI, 25.2-48.7); this difference was significant (P = .008 [95% CI, 12.3-31.0]). No significant differences in wound area measurement by assessment method were reported for the other skin tones.
Additionally, for wounds with ill-defined edges, irregular shapes, unhealthy surrounding tissues, and the presence of necrotic tissues, use of the mobile application was significantly associated with lower mean differences in wound area measurements of 8.2 cm2 (P = .040), 6.8 cm2 (P = .045), 13.1 cm2 (P = .036), and 7.6 cm2 (P = .030), respectively (Table 4).
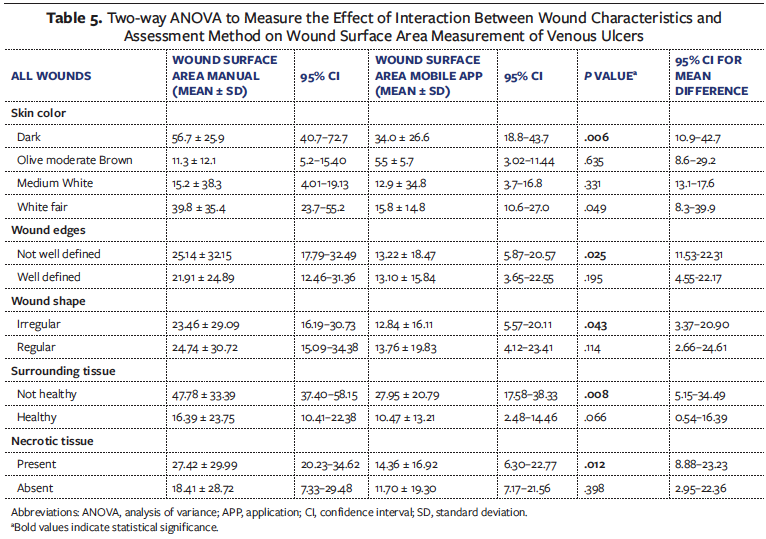
A 2-way ANOVA test was conducted to examine the effects of skin tone and assessment methods on wound area measurements in evaluations of venous ulcers (Table 5). Although traumatic wounds were also significant for size difference, the low sample size prevented subanalysis. For venous ulcers, the simple main effects test for skin tone using different assessment methods showed that in patients with dark skin, use of the mobile application was associated with a significantly lower mean difference in wound area measurement of 22.7 cm2 compared with the manual method (95% CI, 10.9-42.7; P = .006). There was no significant mean difference in wound surface area between methods for the other skin tones (Table 5).
Use of the mobile application was associated with lower estimated marginal mean wound area measurements for wounds with ill-defined edges, irregular shapes, surrounding unhealthy tissue, and necrotic tissue, with a significant mean difference of 11.9 cm2 (P = .025), 10.6 cm2 (P = .043), 19.8 cm2 (P = .008), and 13.1 cm2 (P = .012), respectively (Table 5).
Comparison of billing for debridement codes using manual and digital methods
Based on reimbursement rate for the non-facility Medicare average national payment schedule,21 in the current study the average payment per claim of a wound debridement was significantly higher using the wound area measurements calculated with the TPR method compared with the DWMS ($145 ± $76.40 and $130 ± $55.20, respectively; P = .045). The allowable reimbursement amount for manual wound area measurement was $25 246 for 321 debridement codes, compared with $22 574 with the DWMS for 239 codes, an increase in payment of $2672 (10.6%) with manual area measurement.
Discussion
The findings in this study both support the need to move away from monitoring wound closure by determining wound measurement based on length by width multiplication (due to the overestimation resulting from rectilinear measurements) and provide new analysis of the critical factors that result in poorer performance with this method.
The frequently cited article by Rogers et al6 included 10 patients and found 40% overestimation of wound area. The present study, which had a larger sample size of 177 wounds, found that the TPR method overestimated wound size by 36.6% compared with digital planimetry measurement. Both studies included a variety of wound etiologies. The larger sample size in the present study may have provided more detail about wound complexity, such as irregular wounds, diffuse wound edges, and skin tone, which can be linked to overestimation of wound sizes with manual measurement. The resulting large overestimation reinforces the concern regarding the use of manual length by width multiplication methods to calculate surface area.3,6 The representation with either a rectilinear area multiplication (length × width) does not denote the true shape of the wound.1,3 Clustered wounds and other complex presentations can create unique wound shapes that are not adequately represented by length by width multiplication measurement. Surface planimetry offers clinicians a more accurate, representative surface area measurement,3,6,8,9 with a more consistent value that better reflects changes in wound size.
Wound measurement is more than a documentation requirement and has the potential to offer insight into wound progress and treatment effectiveness.3 Inability to measure or inaccurate measurement of wound area using traditional methods results in missed opportunities to monitor wound progress and potentially identify non-progressing wounds.22 Foltynski et al³ recently suggested that wounds that do not progress by 50% in 4 weeks with standard therapy may require advanced therapy or interdisciplinary assessment. According to the predictive models of Margolis et al,22 an accurate measurement of wound size at the beginning of treatment can predict which wounds will heal by the 24th week of care. For example, wounds that are old and chronic (ie, present for >12 months) and have a larger surface area (>10 cm²) are at increased risk of not healing (78%) compared with smaller wounds of shorter duration.22
Larger surface areas or overestimation of surface areas from manual measurement may create bias when monitoring gross surface area reduction,23 which may result in failure to identify at-risk wounds. Identification of hard-to-heal wounds enables clinicians to reevaluate the underlying wound case, wound cleaning, debridement, moisture, and edges, as well as the opportunity for advanced dressings.24 Surface area can be used to create alerts for wound healing; when integrated into AI tools, it can be utilized as an element to predict wound risk and guide clinician’s efforts.25 Digital wound measurement can speed up clinical assessment and documentation,10 which can enhance clinical decision-making and support improved patient outcomes.
Beyond the overall risk of overestimation, certain subfactors were found to affect the accuracy of measurements. Wound size was significantly overestimated by manual measurements in patients with dark skin tones, as well as in wounds with ill-defined edges, irregular shapes, unhealthy surrounding tissue, and necrotic tissue. Certain clinical signs and symptoms (eg, erythema) are challenging to diagnose in patients with darker skin tones,26 and extra attention is required by the clinician in such situations.27 However, measurement may be another possible consideration in caring for patients with more pigmented skin tones to prevent overestimation. The literature supports the claim that poorer assessment of changes in patients with darker skin results in more severe wound development.26 For example, patients with darker skin tones have an increased likelihood of higher stage pressure injury,26 and historically, patients with non-White skin tones have had worse healing, more limb amputations, and more frequent complications.28 More accurate wound measurement and tracking through digital planimetry may help monitor treatment progress and identify wounds at risk of healing earlier, thus preventing clinical complications.
Accurate wound measurement may be complicated by wound-related factors. In the present analysis, wound characteristics (eg, poorly defined edges, irregular shape, necrotic tissue) caused a significant difference in wound overestimation. Poorly defined edges and irregular shape may make it difficult to visually determine the longest axis of a wound.29 Wound measurement is known to have interrater reliability challenges owing to the subjective assessment of where to measure the wound.30 Langemo et al5 found that all methods of manual measurement (eg, head-to-toe vs. maximum length and width) can result in wide variability in overestimation of surface area. Wound shape and presentation can vary due to wound pathophysiology, and wound shape geometry has been proposed as an indicator of wound healing.31 Patient-related factors (eg, venous stasis) can result in edema that causes change in shape and impairs healing. Length by width multiplication measurement is not sophisticated enough to detect these changes in wound shape. Digital planimetry using smartphone applications can decrease variability in measurement9 and can note more detailed changes in surface area due to changes in shape. Further, measuring wound areas under various lighting conditions and angles can be quite challenging. While the standard natural or evenly distributed artificial lighting protocol is usually adequate for capturing wound images, it may not always be enough. Complex wounds or variable lighting conditions in examination rooms can cause color bias, leading to incorrect assessments.10 Digital tools can help standardize wound assessment across clinicians.32 For example, the digital application evaluated in the present study uses a proprietary fiducial marker that helps calibrate and standardize wound images for color, size, and distance, and it provides a combination of color-based image analysis algorithms that are valuable in reducing the variability in wound measurements.10 Such variability leads to poor outcomes in at-risk populations.
Wound measurements affect patient outcomes and health system spending. Puri et al20 noted that Medicare spending on wound care continues to increase at a rate higher than the inflation rate and that the use of debridement procedures increased 32% between 2012 and 2017. Based on the findings of the present study, the use of manual methods for claims would result in 10% overbilling. Reimbursement for debridement codes for wounds larger than 20 cm² cost Medicare more than $17 million in 2017.20 Fees for procedural diagnosis codes have increased markedly since then; for example, in 2017 removal of tissue from wounds each additional 20-cm² payment rate was $8.26 (97598)20 and in 2022 that same code was $43.98.33 Therefore, if current wound care debridement costs are estimated to be approximately 5.32 times higher since 2017, or $90.4 million annually, then reducing payment by 10.6%, as seen in the present study, could save Medicare $8.5 million annually. Cost savings from reducing debridement costs could be directed toward the use of other advanced therapies that support wound closure in patients with hard-to-heal wounds.
Limitations
The present study adds to the literature by expanding the understanding of overestimation of wound measurement by manual TPR methods and by identifying contributing subfactors, but it has limitations. While the sample size was larger than in other studies,6 recruitment was done by a single physician at a single outpatient clinic. This may limit the generalizability to other wound care populations. Future research could incorporate other practice settings, such as acute care, and expand the patient age range to investigate variations in wound population. Overestimation was measured in the present study; however, clinical effect owing to lack of sensitivity is an important area for future studies. Digital wound measurement was proved to be advantageous in a single assessment; however, the effect of earlier identification of nonhealing wounds or the identification of appropriate treatments may support the adoption of digital planimetry. Future research could explore the various treatment types and dosages administered to wound patients based on wound length and width, as well as on surface area measurements obtained using manual techniques vs. a digital application, with the goal of more streamlined and effective care.
Conclusions
Documenting length and width is standard practice in wound care; however, in the present study TPR measurements overestimated wound size by 36.6% compared with digital planimetry measurement. Wounds in patients with dark skin tones, as well as wounds with diffuse edges, irregular shapes, necrotic tissue, and unhealthy surrounding tissue have an increased likelihood of size overestimation. These inaccuracies have implications for patient care as well as the health care system. According to the findings of the present study, using digital technology is cost-effective. Manual methods were associated with a 25.5% increase in submitted debridement codes, resulting in a 10.6% increase in payment. Accurate surface area tracking can serve as a better indicator of treatment efficiency and support modification of treatment plans. Precise measurements can be used for better risk management and prognostics. Using digital planimetry to ensure accuracy of wound measurement is critical to promoting superior patient outcomes, clinician experience, and health system sustainability.
Acknowledgments
Authors: Misael C. Alonso, MD, FACP, CWSP, FAPWCA1; Heba Tallah Mohammed, PhD, MD2; Robert D. Fraser, MN, RN2,3; Jose L. Ramirez Garcia Luna, MD, PhD4; and David Mannion, BA2
Affiliations: 1Abrazo Health Care, Arizona US; 2Swift Medical Inc, Toronto, Ontario, Canada; 3Western University, Arthur Labatt Family School of Nursing, London, Ontario, Canada; 4McGill University, Montreal, Quebec, Canada
ORCID: Mohammed, 0000-0002-0848-8384
Disclosures: Dr Mohammed and Mr Fraser are paid employees of Swift Medical. The author(s) received no specific funding for this work.
Correspondence: Heba Tallah Mohammed, PhD, MD; Associate Director, Research and Evaluation, Swift Medical Inc, Clinical Innovation, Validation and Research, Toronto, Ontario, Canada; heba@swiftmedical.com
Manuscript Accepted: September 14, 2023
How Do I Cite This?
Alonso MC, Mohammed HT, Fraser RD, Ramirez Garcia Luna JL, Mannion D. Comparison of wound surface area measurements obtained using clinically validated artificial intelligence-based technology versus manual methods and the effect of measurement method on debridement code selection and reimbursement cost. Wounds. 2023;35(10):E330-E338. doi:10.25270/wnds/23031
References
1. Mirzaalian Dastjerdi H, Töpfer D, Rupitsch SJ, Maier A. Measuring surface area of skin lesions with 2D and 3D algorithms. Int J Biomed Imaging. 2019;4035148. doi:10.1155/2019/4035148
2. Bien P, De Anda C, Prokocimer P. Comparison of digital planimetry and ruler technique to measure ABSSSI lesion sizes in the ESTABLISH-1 study. Surg Infect (Larchmt). 2014;15(2):105–110. doi:10.1089/sur.2013.070.
3. Foltynski P, Ciechanowska A, Ladyzynski P. Wound surface area measurement methods. Biocybernet Biomed Engin. 2021;41(4):1454-1465. doi:10.1016/j.bbe.2021.04.011.
4. Lucas Y, Niri R, Treuillet S, Douzi H, Castaneda B. Wound size imaging: ready for smart assessment and monitoring. Adv Wound Care (New Rochelle). 2021;10(11):641-661. doi:10.1089/wound.2018.0937
5. Langemo D, Anderson J, Hanson D, Hunter S, Thompson P. Measuring wound length, width, and area: which technique? Adv Skin Wound Care. 2008;21(1):42-45. doi:10.1097/01.ASW.0000284967.69863.2f
6. Rogers LC, Bevilacqua NJ, Armstrong DG, Andros G. Digital planimetry results in more accurate wound measurements: a comparison to standard ruler measurements. J Diabetes Sci Technol. 2010;4(4):799-802. doi:10.1177/193229681000400405.
7. Oien RF, Håkansson A, Hansen BU, Bjellerup M. Measuring the size of ulcers by planimetry: a useful method in the clinical setting. J Wound Care. 2002;11(5):165-168. doi:10.12968/jowc.2002.11.5.26399
8. Bowling FL, Paterson J, Ndip A. Applying 21st century imaging technology to wound healing: an Avant-Gardist approach. J Diabetes Sci Technol. 2013;7(5):1190-1194. doi:10.1177/193229681300700536
9. Wang SC, Anderson JAE, Evans R, et al. Point-of-care wound visioning technology: Reproducibility and accuracy of a wound measurement app. PLoS One. 2017;12(8):e0183139 doi:10.1371/journal.pone.0183139
10. Mohammed HT, Bartlett R, Babb D, et al. A time motion study of manual versus artificial intelligence methods for wound assessment. PLoS One. 2022; 17(7), e0271742. doi:10.1371/journal.pone.0271742
11. Li D, Mathews C. Automated measurement of pressure injury through image processing. J Clin Nurs. 2017;26(21-22):3564-3575. doi:10.1111/jocn.13726
12. Ramachandram D, Ramirez-GarciaLuna J, Fraser R, Martínez-Jiménez MA, Arriaga-Caballero JE, Allport J. Fully automated wound tissue segmentation using deep learning on mobile devices: cohort study. JMIR MHealth UHealth. 2022;10(4), e36977. doi:10.2196/36977
13. Scafide KN, Downing NR, Kutahyalioglu NS, Sebeh Y, Sheridan DJ, Hayat MJ. Quantifying the degree of bruise visibility observed under white light and an alternate light source. J Forensic Nurs. 2021;17(1):24-33. doi:10.1097/JFN.0000000000000304
14. Hettiarachchi NDJ, Mahindaratne RBH, Mendis GDC, Nanayakkara HT, Nanayakkara ND. Mobile based wound measurement. IEEE Point Care Healthc Technol. 2013;298-301. doi:10.1109/PHT.2013.6461344
15. Taylor SC, Cook-Bolden F. Defining skin of color. Cutis. 2002; 69(6):435-437.
16. Hsu J, Chen Y, Ho T, et al. Chronic wound assessment and infection detection method. BMC Med Inform Decis Mak. 2019;19(1):99. doi:10.1186/s12911-019-0813-0
17. Wendelken ME, Berg WT, Lichtenstein P, Markowitz L, Comfort C, Alvarez OM. Wounds measured from digital photographs using photodigital planimetry software: validation and rater reliability. Wounds. 2011;23(9):267-275.
18. Manna B, Nahirniak P, Morrison CA. Wound Debridement. In: StatPearls. StatPearls Publishing; 2022.
19. Wang LL, Adelekun A, Taylor SC, et al. Fee-for-service and structural forces may drive racial disparities in US dermatology. Br J Dermatol. 2020;183(4):750–751. doi:10.1111/bjd.19217
20. Puri P, Kaur P, Bhullar S, Baliga S. Trends in Medicare utilization and reimbursement for wound debridement procedures 2012–2017. J Dermatol Treat. 2022;33(2):1136-1139. doi:10.1080/09546634.2020.1800581
21. Wright Access. Reimbursement guide: BIOSKIN Amniotic Wound Matrix. 2021. Accessed November 30, 2022. http://www.wrightemedia.com/ProductFiles/Files/PDFs/AP-011961_EN_LR_LE.pdf
22. Margolis DJ, Allen-Taylor L, Hoffstad O, Berlin JA. The accuracy of venous leg ulcer prognostic models in a wound care system. Wound Repair Regen. 2004;12(2):163-168. doi:10.1111/j.1067-1927.2004.012207.x
23. Bull RH, Staines KL, Collarte AJ, Bain DB, Ivins NM, Harding KG. Measuring progress to healing: a challenge and an opportunity. Int Wound J. 2022;19(4):734–740. doi:10.1111/iwj.13669
24. Grey JE, Enoch S, Harding KG. Wound assessment. BMJ. 2006;332(7536):285-288. doi:10.1136/bmj.332.7536.285.
25. Gupta R, Goldstone L, Eisen S, et al. Towards an AI-based objective prognostic model for quantifying wound healing. IEEE J Biomed Health Inform. Published online March 3, 2023. doi:10.36227/techrxiv.21067261.v1
26. Ozageer Gunowa N, Hutchinson M, Brooke J, Jackson D. Pressure injuries in people with darker skin tones: a literature review. J Clin Nurs. 2018;27(17–18):3266–3275. doi:10.1111/jocn.14062
27. Black J, Simende A. Ten top tips: assessing darkly pigmented skin. Wounds Int. 2020;11(3):8–11.
28. Naga HI, Azoury SC, Othman S, et al. Short- and long-term outcomes following severe traumatic lower extremity reconstruction: the value of an orthoplastic limb salvage center to racially underserved communities. Plast Reconstr Surg. 2021;148(3):646-654. doi:10.1097/PRS.0000000000008277
29. Wang L, Pedersen P, Agu E, et al. Area determination of diabetic foot ulcer images using a cascaded two-stage SVM-based classification. IEEE Trans Biomed Eng. 2017;64(9):2098-2109. doi:10.1109/TBME.2016.2632522.
30. Chan KS, Lo ZJ. Wound assessment, imaging and monitoring systems in diabetic foot ulcers: a systematic review. Int Wound J. 2020;17(6):1909-1923. doi:10.1111/iwj.13481.
31. Cardinal M, Eisenbud DE, Armstrong DG. Wound shape geometry measurements correlate to eventual wound healing. Wound Repair Regen. 2009;17(2):173–178. doi:10.1111/j.1524-475X.2009.00464.x
32. Au Y, Beland B, Anderson J, Sasseville D, Wang SC. Time-saving comparison of wound measurement between the ruler method and the Swift Skin and Wound App. J Cutaneous Med Surg. 2019;23(2):226-228. doi:10.1177/1203475418800942.
33. American Medical Association. Appendix B for administrative order - physician fee schedule. 2022. Accessed October 14, 2023. https://wcd.oregon.gov/medical/Documents/payment-tables/appendix-b/4-22-Appendix-B.pdf






