



Determinants of Delayed Wound Healing in Postoperative Patients: A Multihospital-Based Prospective Study Performed in South India
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Wounds or HMP Global, their employees, and affiliates.
Abstract
Background. Delayed wound healing (DWH) leads to various health problems and increases the cost of health care for patients. Objective. To identify the determinants associated with DWH in postoperative patients. Materials and Methods. This prospective study included 225 postoperative patients admitted to 3 tertiary care hospitals in south India. Data were collected by interviewing each patient. DWH was defined as absence of wound retraction 10 days postoperative. Results. Nonhealing of the surgical wound was noted in 96 patients (42.7%). In the multivariable analysis, the presence of comorbidities like obesity and hypertension, an American Society of Anesthesiologists score of II or III, not using ceftriaxone with sulbactam prophylactically before surgery, an increased fasting blood sugar status in the postoperative period, and resistance to fluoroquinolones and aminoglycosides in the culture and sensitivity reports were associated with DWH in the patients studied. Conclusion. Detailed preoperative evaluation of patients, controlling comorbidities, using appropriate antibiotics, and postoperative control of blood sugars in patients with diabetes, as well as culture and sensitivity testing, are needed to minimize the occurrence of DWH.
Introduction
Delayed wound healing (DWH) is a critical problem during the postoperative period.1 DWH leads to physical and mental health problems among postoperative patients. Additionally, it prolongs the hospital stay, leading to an increase in the cost of health care.
Several modifiable factors—such as the use of substances of abuse, malnutrition, stress, and comorbidities such as obesity and diabetes mellitus—have been implicated in DWH.1 Appropriately identifying high-risk patients and providing them with good pre- and postoperative care can help reduce the occurrence of DWH, thereby accelerating the recovery process. Prevention of various modifiable risk factors also avoids other postoperative complications that can prolong hospital stays.
The current study was performed to identify preoperative, surgical, and postoperative determinants associated with DWH among postoperative patients at different types of tertiary health care facilities in southern India.
Materials and Methods
This prospective study included postoperative patients admitted to 2 government hospitals and 1 private hospital affiliated with Kasturba Medical College in Mangalore, India. Institutional Ethics Committee approval was obtained on May 17, 2023 (approval number IEC KMC MLR 05/2023/231). Permission from the medical superintendents of the 3 hospitals was obtained before the start of the study. All postoperative patients who were admitted to the hospital for more than 10 days were included in this study via the convenience sampling method. Patients who were admitted with nonsurgical wounds; those who were outpatients for procedures such as venous port placement, lymph node biopsy, or fine-needle aspiration cytology; and those who did not consent to participate were excluded from this study.
Written informed consent was obtained from each participant in the local language, Kannada, after they were provided details regarding the nature and purpose of the study.
The sample size of this study was calculated via the formula Zα2pq/d2, where “Zα” value was taken as 1.96 at 95% confidence intervals, “p” was the estimated proportion of postoperative patients with DWH, “q” was the estimated proportion of the postoperative patients with normal wound healing (which was “1-p”), and “d” was the desired margin of error. With the assumption that 20% of postoperative patients develop DWH based on the findings of another south Indian study2 substituted as “p” and 6% absolute precision substituted as “d”, the sample size was calculated as 171. In anticipation of a nonresponse rate of 20%, the final sample size was rounded to 205 participants.
Data were collected by interviewing each patient in the postoperative period via a semistructured interview schedule. This schedule was prepared after an extensive literature review.
The schedule was content validated with the help of subject experts. It was then translated into Kannada and back-translated to English for language validation.
Wounds heal through the phases of hemostasis, inflammation, proliferation, and tissue remodeling.3-6 DWH was defined as failure of the wound to reach the proliferation stage as identified by absence of wound retraction 10 days postoperative.
Participants’ socioeconomic status was assessed via the modified Kuppuswamy socioeconomic scale of 2022.7 The preoperative height and weight of the participants were recorded from the case sheets. Body mass index (BMI) was categorized according to the Asia-Pacific BMI classification.8
Data collection tool
The data collection tool has 4 sections. Section A contains information regarding participants’ sociodemographic details, such as age, sex, marital status, education, occupation, type of family, education and occupation of the head of the household, total monthly family income, and place of residence. Section B asks about participants’ lifestyle habits, such as the use of alcohol and chewing tobacco, and smoking in the last month (current history of substance abuse); the type of diet consumed (eg, vegetarian or mixed); and comorbidities. Section C contains details regarding the American Society of Anesthesiologists (ASA) score; type of surgical procedure; site and length of the surgical incision; type of anesthesia given to the patient, whether general, regional, or spinal; preoperative practices, such as the type of antibiotics used before surgery, and requirement for blood transfusion; and postoperative practices, such as the requirement for blood transfusion after surgery, placement of a urinary catheter, and status of the wound 10 days after surgery. This information was recorded from the patient’s medical case record. The investigators then assigned ASA classification status as follows: class I for normal healthy patients, class II for patients with mild systemic disease, class III for patients with severe systemic disease that was not incapacitating, class IV for patients with severe systemic disease that was a constant threat to life, class V for patients who were moribund and not expected to survive without the operation, and class VI for patients who were declared brain dead.9 In section D of the data collection tool, the culture and sensitivity reports of the samples taken from the surgical wound as well as the hemoglobin and fasting blood sugar (FBS) values before and after surgery were recorded by the investigators from the case sheets.
Data analysis
Data entry and analysis were performed using SPSS Statistics for Windows version 25.0 (IBM Corporation). The descriptive statistics are presented as mean (SD) and percentages. Determinants associated with DWH were analyzed via unpaired t tests, chi-square tests, and Fisher exact tests via univariate analysis and binary logistic regression analysis. A P value of less than .05 was considered statistically significant.
Results
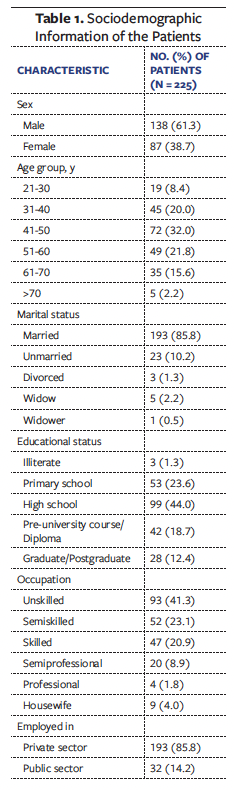
Among the 225 patients, 192 (85.3%) were admitted to the 2 government hospitals, and the remaining 33 (14.7%) were admitted to the private hospital. The mean (SD) age of the patients was 47.9 (12.4) years (range, 21 years-81 years). The most common education level achieved was high school (n = 99 [44.0%]), and the most common occupation was unskilled worker (n = 93 [41.3%]) (Table 1).
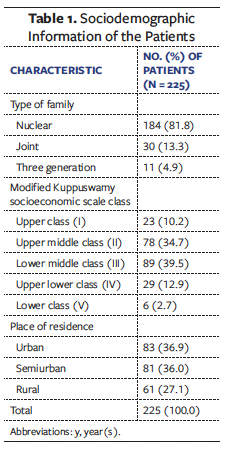
Type II diabetes mellitus was by far the most common comorbidity (n = 112 [49.8%]). Overweight or obesity was present in 161 patients (71.6%) (Table 2).
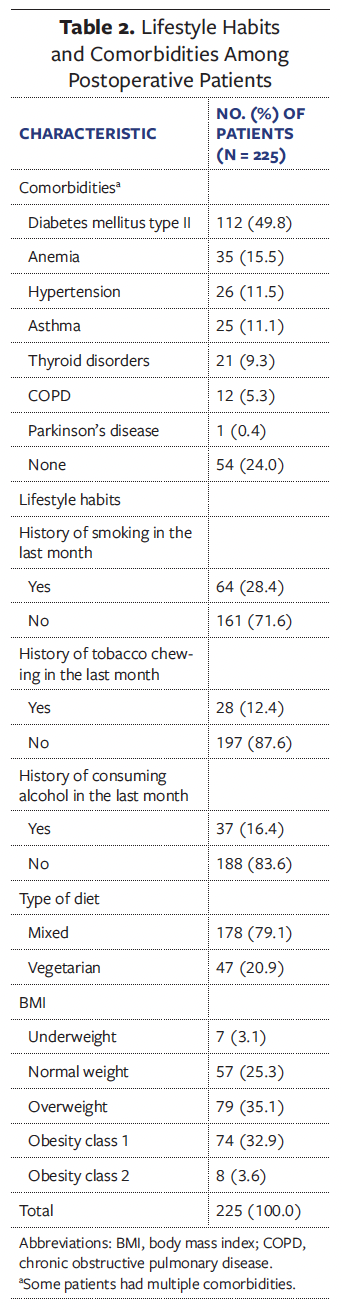
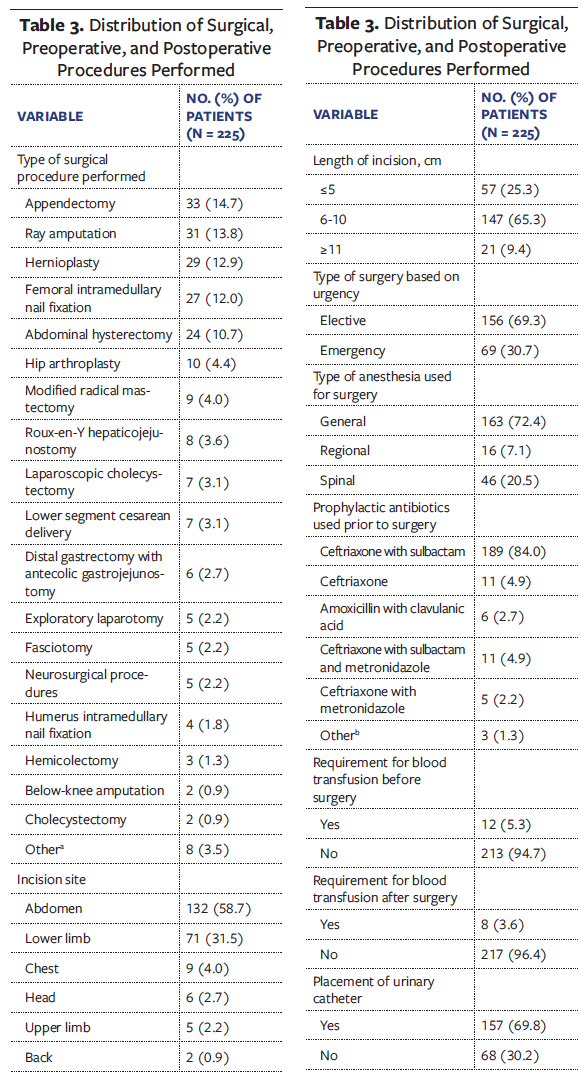
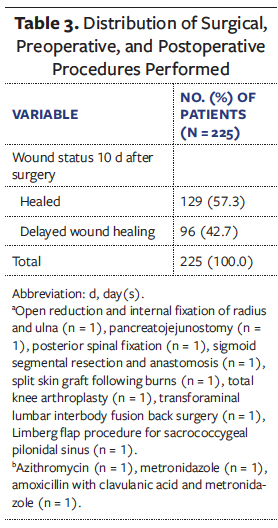
Among the patients, 91 (40.4%), 126 (56.0%), and 8 (3.6%) were of ASA class I, II and III, respectively. The most common surgical procedure performed was appendectomy (n = 33 [14.7%]). Among the 7 patients who underwent lower segment cesarean delivery, 3 had a history of gestational diabetes mellitus during the antenatal period. The most common site of incision was the abdomen (n = 132 [58.7%]), followed by the lower limb (n = 71 [31.5%]). Preoperatively, ceftriaxone with sulbactam antibiotic was given to most patients (n = 189 [84.0%]). Postoperatively, nonhealing of the surgical wound 10 days after surgery was noted in 96 patients (42.7%) (Table 3).
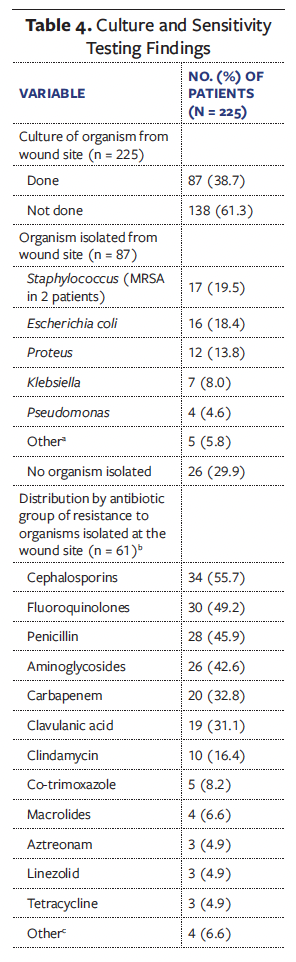
Eighty-seven patients (38.7%) underwent culture and sensitivity testing. The most common organism identified was Staphylococcus (n = 17 [19.5%]). In 26 samples, no organisms were identified. Among the remaining 61 samples, the most common antibiotics the organisms were found to be resistant to were cephalosporins (n = 34 [55.7%]) (Table 4).
The various sociodemographic variables and comorbidities associated with DWH status among the patients in the univariate analysis at P values less than or equal to .15 are shown in Table 5. These variables were age group, sex, and educational status of the patients, whether they were employed in the private or public sector, their socioeconomic status as per the modified Kuppuswamy socioeconomic scale, type of hospital (whether government or private) where the patient was seeking treatment, BMI, presence of diabetes mellitus type II and hypertension, and their ASA score.
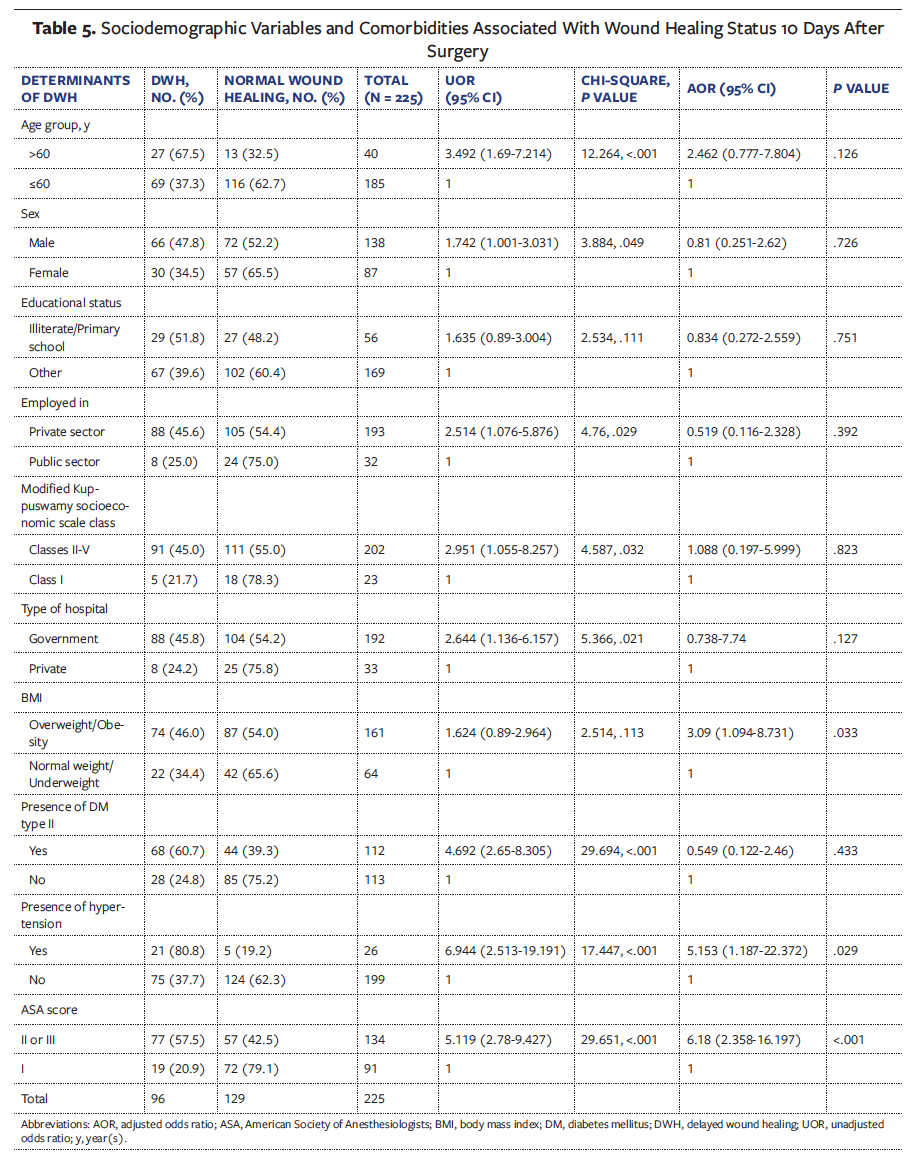
The mean (SD) age of the 96 patients with DWH was 50.3 (13.6) years, and that of the 129 patients with normal healing was 46.2 (11.2 years) (t = 2.421, P = .016). The male-to-female ratio among the patients who presented with DWH was 2.2:1.
There was no association between DWH and marital status (P = .16), occupation (P = .16), type of family (P = .863), place of residence (P = .628), presence of anemia (P = .17), presence of asthma (P = .225), presence of chronic obstructive pulmonary disease (P = .259), current history of smoking (P = .161), current history of alcohol consumption (P = .938), current history of tobacco chewing (P = .427), or type of diet (P = .311).
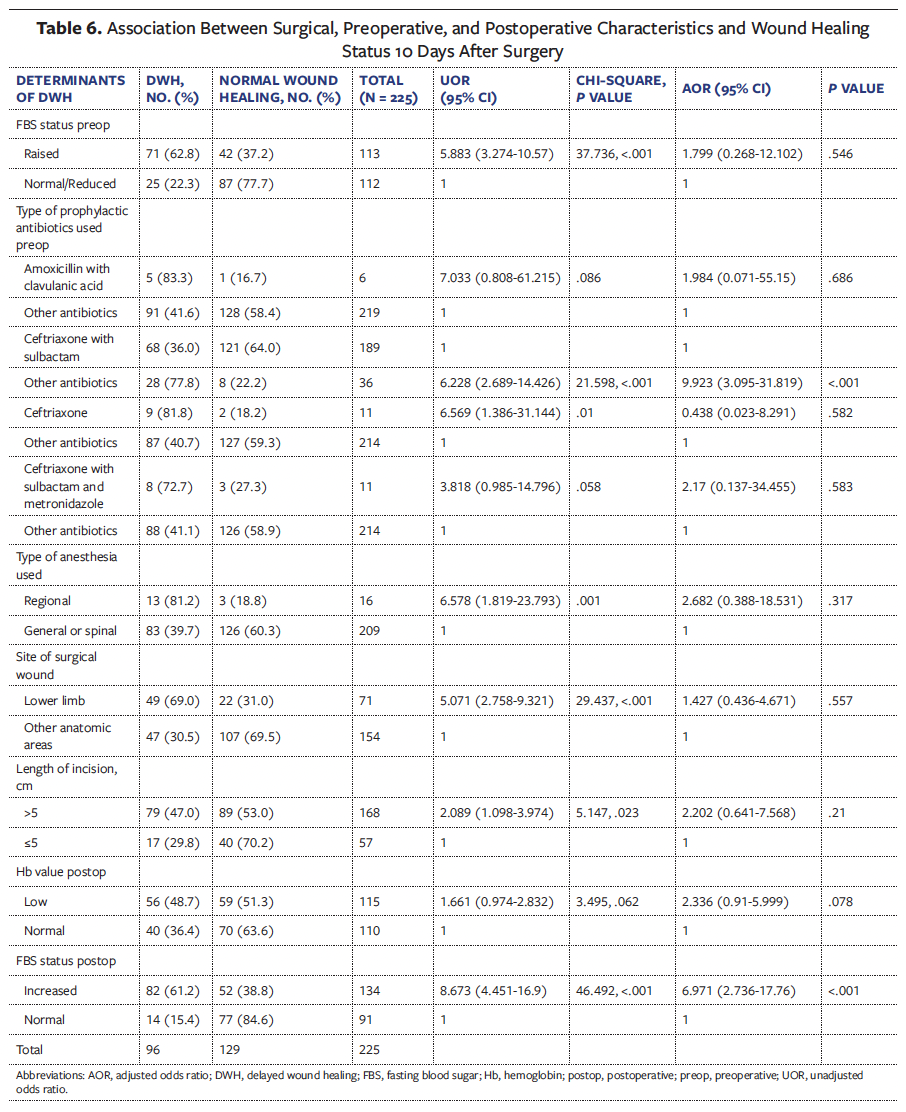
The various surgical, preoperative, and postoperative characteristics associated with wound healing status 10 days after surgery among patients in the univariate analysis at P values less than or equal to .15 are shown in Table 6. There was no association between DWH and the use of metronidazole given prophylactically before surgery (P > .99); azithromycin given prophylactically before surgery (P = .427); amoxicillin, clavulanic acid, and metronidazole given prophylactically before surgery (P = .427); ceftriaxone with metronidazole given prophylactically before surgery (P = .166); the requirement of blood transfusion before surgery (P = .259); a low hemoglobin level before surgery (P = .267); the requirement of blood transfusion after surgery (P = .291); or the presence of a urinary catheter (P = .337).
The associations among organisms isolated from the surgical wound, the resistance status to various antibiotics, and the healing status of the wound 10 days after surgery among the patients in the univariate analysis at P values less than or equal to .15 are shown in Table 7. There was no association between DWH status and the presence of Klebsiella (P = .1968), Acinetobacter (P > .99), Escherichia coli (E coli) (P = .1779), or Pseudomonas (P > .99). Similarly, there was no association between DWH status and sulbactam resistance (P > .99), vancomycin resistance (P > .99), aztreonam resistance (P > .99), macrolide resistance (P = .576), linezolid resistance (P > .99), co-trimoxazole resistance (P = .579), tetracycline resistance (P > .99), or nitrofurantoin resistance (P > .99).
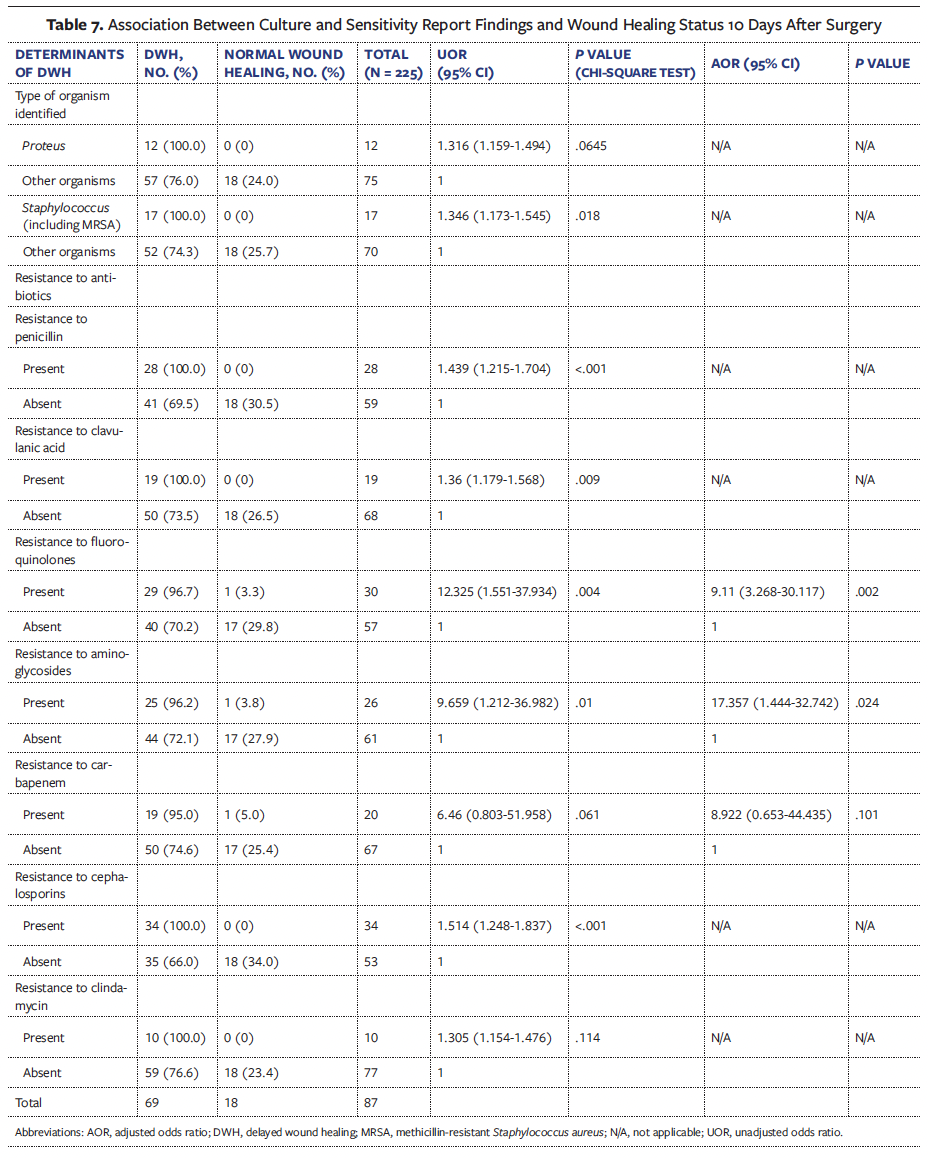
All 29 variables associated with DWH at a P value less than or equal to .15 in the univariate analysis were introduced into the binary logistic regression analysis model. The P values of 6 variables, namely, the presence of Proteus or Staphylococcus, and resistance to penicillin or cephalosporins, or to clindamycin or clavulanic acid, were close to 1. Therefore, these variables were eliminated from the model. The Nagelkerke R2 value of the model was 0.71, and the Hosmer-Lemeshow test P value was .193, indicating that the model was a good fit. In the multivariable analysis, the presence of the comorbidities overweight or obesity, and hypertension; an ASA score of II or III; not using ceftriaxone with sulbactam prophylactically before surgery; an increased FBS status in the postoperative period; and resistance to fluoroquinolones and aminoglycosides in the culture and sensitivity reports were associated with DWH (Tables 5, 6, and 7).
Discussion
In the present study, 42.7% of patients experienced DWH. Other studies have reported postoperative DWH rates of 3%,10 3.2%,11 12.2%,1 and 20%.2 In 2 other Indian studies done among patients who underwent abdominal laparotomy, one in Bangalore4 and the other at Burla,5 both studies reported 40% of such patients had DWH.
The mean age of patients who presented with DWH in the current study was 50.3 years, compared with 62.2 years in a study performed in Burla, India.5
Among patients with DWH, the proportion of males was more than twice that of females in the present study and was 3 times greater than that of females in previous studies.4,5,11 This finding may be due to the favorable regulatory effect of estrogen in the wound healing process among females.12
According to the univariate analysis in the current study, DWH was considerably more common among patients in government hospitals than among those in private hospitals. Although there was not a significant association between hospital type and DWH in the multivariate analysis, this difference could be because of the longer waiting time for surgery among patients admitted to government hospitals.13 Prolonged hospital stay increases the vulnerability of patients to nosocomial infections.
The preoperative determinants of DWH in the multivariable analysis in the present study were the presence of comorbidities such as overweight or obesity, and hypertension; an ASA score of II or III; and not using ceftriaxone with sulbactam prophylactically before surgery. Previous studies reported the following as preoperative factors associated with DWH: male biological sex4; comorbidities such as increased BMI,2,14,15 anemia,2,14 hypertension,2,14 and diabetes mellitus2,14; acute abdomen following traumatic causes as indications for first surgery11; and emergency laparotomy.4
Individuals with obesity are prone to DWH due to hypoperfusion effects as a consequence of poor vascularization in the subcutaneous adipose tissue.15,16 Inadequate oxygenation in the tissue surrounding a wound reduces collagen synthesis and leads to a poor inflammatory response, which impairs the cellular repair process.15,17 Reduced infiltration of immune cells due to hypoperfusion also increases the risk of infection in the wound, resulting in DWH.18 Therefore, it is essential to formulate a reasonable weight loss plan for patients scheduled for elective surgery during the preoperative period to minimize DWH in the postoperative period. Hypertension causes tissue edema and decreases the oxygen supply to wounds; thus, patients with hypertension are prone to DWH.19 ASA scores II and III indicate the presence of systemic diseases. Thus, optimizing the patient’s health condition prior to elective surgery is important to prevent DWH.
In the current study, the use of ceftriaxone with sulbactam prophylactically before surgery was associated with faster wound healing. This finding indicates that the use of appropriate antibiotics before surgery is essential to avoid DWH.
Surgical factors such as type of anesthesia, site of surgical wound, and incision size were not associated with DWH in the current study. However, in a study performed in Raipur, India, the length of the surgical incision was associated with DWH.15
Postoperative factors such as increased FBS and resistance of microorganisms to fluoroquinolones and aminoglycosides in culture and sensitivity reports were associated with DWH among the patients in this study. In other studies, excessive intraoperative blood loss,14 delayed ambulation,14 inadequate post-operative wound care,14 and development of postoperative sepsis11 were identified as risk factors for DWH.
Higher blood glucose levels also affect leukocyte function during the inflammatory stage of wound healing. Diabetes mellitus causes long-term microvascular damage, which results in tissue hypoxia and a reduced supply of nutrients. Hypoxia further affects the processes of reepithelialization and collagen deposition required for wound healing.3 Uncontrolled blood glucose also causes dysfunction of endothelial cells and disrupts the proliferation of keratinocytes and fibroblasts, which are essential for reepithelialization.20
The most common organism identified in surgical wounds in the present study was Staphylococcus, as observed in other studies.2,21-23 The proportions of various microorganisms present in surgical wounds reported in previous studies are as follows, Staphylococcus in 11.4%,23 13.4%,10 36%,21 45%,22 41.7%,2 and 50%23; E coli in 7.7%,23 10.3%,10 12%,21 13%,22 and 40.3%25; Klebsiella in 5.1%,10 7.5%,24 10%,21 10.9%,25 and 24%22; Pseudomonas in 5%,22 8%,21 8.2%,10 and 26.9%23; Acinetobacter in 10%21,22; and Proteus in 3%.22 In the current study, the presence of Staphylococcus in the univariate analysis and resistance to certain antibiotics in the multivariable analysis were associated with DWH. Thus, performing culture and sensitivity tests using appropriate antibiotics will help prevent DWH.
Limitations
This study was performed at 3 hospitals in a single urban area; thus, the findings may not be generalizable to postoperative patients in other geographical regions. Data regarding specific nutrients, such as vitamins A, C, E, and K; zinc; polyphenols; omega-3 fatty acids; amino acids; and quality protein consumed in a day were not collected from the patients and so were not analyzed in relation to DWH status. Similarly, data regarding albumin, prealbumin, and other inflammatory markers were not available in the medical records of the majority of patients and were not noted by the investigators. The investigators also did not assess whether a proinflammatory diet of highly processed foods had any effect on DWH.
Conclusion
Greater than 40% of the patients in the current study had DWH. The researchers identified several pre- and postoperative factors associated with DWH. Patients with mild or severe systemic diseases, resulting in ASA scores of II or III, need appropriate disease management in the preoperative period for improved wound healing and well-being. Lifestyle changes such as diet control and increased physical activity are needed to reduce overweight and obesity, as well as blood pressure. The protocol of using ceftriaxone with sulbactam prophylactically before surgery needs to be followed in hospitals for better wound healing results. Antibiotic stewardship should be adopted in these settings to promote the appropriate use of antibiotics and minimize the risk of antibiotic resistance. Detailed preoperative evaluation of patients, control of various comorbidities, the use of appropriate antibiotics, and postoperative control of blood sugars in patients with diabetes, as well as culture and sensitivity testing, are needed to minimize the occurrence of DWH. The involvement of a multidisciplinary team of professionals comprising surgeons, anesthesiologists, infectious diseases physicians, nurses, and microbiologists is needed to address DWH.
Author & Publication Information
Authors: Nitin Joseph, MBBS, MD, PGDFM1; Madhuri Vishnoi, MBBS2; Paarth Garg, MBBS, MD3; and Atmananda Hedge, MBBS, MS, MRCS Ed4
Affiliations: 1Department of Community Medicine, Kasturba Medical College Mangalore, Manipal Academy of Higher Education, Manipal, India; 2Kasturba Medical College Mangalore, Manipal Academy of Higher Education, Manipal, India; 3Autonomous State Medical College, Firozabad, India; 4Department of Orthopedics, Kasturba Medical College Mangalore, Manipal Academy of Higher Education, Manipal, India
Acknowledgments: The authors thank all the medical superintendents of the 3 participating hospitals for granting permission to perform this research study.
Ethical Approval: The Institutional Ethics Committee of Kasturba Medical College of Mangalore approved this study on May 17, 2023 (approval number IEC KMC MLR 05/2023/231). Written informed consent was obtained from each participant.
Funding: This study was funded in whole by the Indian Council of Medical Research, New Delhi, India, under Short Term Studentship Research Grants (grant number 2023-12703).
Disclosure: The authors disclose no financial or other conflicts of interest.
Correspondence: Nitin Joseph, Department of Community Medicine, Kasturba Medical College, Light House Hill Road, Mangalore 575001, Karnataka State, India, nitin.josep@manipal.edu
Manuscript Accepted: July 1, 2025
References
1. Zehnpfennig L, Ritter M, Montagna G, et al. The impact of delayed wound healing on patient-reported outcomes after breast cancer surgery. J Plast Reconstr Aesthet Surg. 2022;75(11):4125-4132. doi:10.1016/j.bjps.2022.06.106
2. Panda S, Uppala M. Study on wound healing following major abdominal gynaecological surgeries in a tertiary care hospital. Int J Reprod Contracept Obstet Gynecol. 2023;12(5):1297-1302. doi:10.18203/2320-1770.ijrcog20231213
3. Wernick B, Nahirniak P, Stawicki SP. Impaired Wound Healing. [Updated Aug 28, 2023]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482254/
4. Guru R, Panigrahy B, Habada SK, et al. Factors affecting post-laparotomy wound healing. Eur J Cardiovasc Med. 2023;13(3):378-381. doi:10.5083/ejcm/2023
5. Panigrahi S, Sethy S, Bhoi K, Saurav S, Panigrahi
M. Factors affecting wound healing after laparotomy at a tertiary care hospital, Odisha, India: a prospective interventional study. International Journal of Anatomy, Radiology and Surgery. 2023;12(3):SO01-SO03. doi:10.7860/IJARS/2023/59903.2885
6. Singh S, Young A, McNaught CE. The physiology of wound healing. Surgery (Oxford). 2017;35(9):473-477. doi:10.1016/j.mpsur.2017.06.004
7. Sood P, Bindra S. Modified Kuppuswamy socioeconomic scale: 2022 update of India. International Journal of Community Medicine and Public Health. 2022;9(10):3841-3844. doi:10.18203/2394-6040.ijcmph20222581
8. Okawa Y, Mitsuhashi T, Tsuda T. The Asia-Pacific body mass index classification and new-onset chronic kidney disease in non-diabetic Japanese adults: a community-based longitudinal study from 1998 to 2023. Biomedicines. 2025;13(2):373. doi:10.3390/biomedicines13020373
9. American Society of Anesthesiologists. Statement on ASA Physical Status Classification System. Updated December 13, 2020. Accessed March 1, 2025. https://www.asahq.org/standards-and-practice-parameters/statement-on-asa-physical-
status-classification-system
10. Metgud MC, Kataria A, Nadipally SR, Patil K. Incidence of wound dehiscence following obstetric and gynecological surgeries at a tertiary care hospital: a retrospective study. Journal of SAFOG. 2020;12(2):73-78. doi:10.5005/jp-journals-10006-1763
11. Teklemariam BT, Biyana CF, Asfaw SA. Determinants of postoperative abdominal wound dehiscence among patients operated in a tertiary hospital. Ethiop J Health Sci. 2022;32(4):739-746. doi:10.4314/ejhs.v32i4.10
12. Li Z, Ma R, Tan J, et al. Hormonal interventions in skin wounds - a mini review. Mol Med. 2024;30(1):217. doi:10.1186/s10020-024-00978-6
13. Obermair A. What are the pros and cons of having treatment in the public vs private hospital system? Updated June 6, 2024. Accessed April 19, 2025. https://www.obermair.info/latest-news/blog/what-are-the-pros-and-cons-of-having-treatment-in-the-public-vs-private-hospital-system/
14. Ranjan A, Surabhi, Singh R, Sinha S. Risk factor assessment for wound dehiscence following caesarean section: a study from a tertiary care center in Bihar. IJPQA. 2025;16(1):284-291.
15. Nagaria T, Kujur A, Thakur N. Incision length: an emerging risk factors for surgical-site infection following cesarean section. Int J Reprod Contracept Obstet Gynecol. 2017;6(5):1829-1833. doi:10.18203/2320-1770.ijrcog20171566
16. Villela NR, Kramer-Aguiar LG, Bottino DA, Wiernsperger N, Bouskela E. Metabolic disturbances linked to obesity: the role of impaired tissue perfusion. Arq Bras Endocrinol Metabol. 2009;53(2):238-245. doi:10.1590/s0004-27302009000200015
17. Hong WX, Hu MS, Esquivel M, et al. The role of hypoxia-inducible factor in wound healing. Adv Wound Care (New Rochelle). 2014;3(5):390-399. doi:10.1089/wound.2013.0520
18. Spampinato SF, Caruso GI, De Pasquale R, Sortino MA, Merlo S. The treatment of impaired wound healing in diabetes: looking among old drugs. Pharmaceuticals (Basel). 2020;13(4):60. doi:10.3390/ph13040060
19. Ozgok Kangal MK, Regan JP. Wound Healing. [Updated May 1, 2023]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024.
20. Burgess JL, Wyant WA, Abdo Abujamra B, Kirsner RS, Jozic I. Diabetic wound-healing science. Medicina (Kaunas). 2021;57(10):1072. doi:10.3390/medicina57101072
21. Mathur P, Mittal S, Trikha V, et al. Surveillance for surgical site infections in orthopedic trauma surgeries at an Indian hospital. Indian J Med Microbiol. 2022;40(2):268-273. doi:10.1016/j.ijmmb.2021.12.016
22. Gupta S, Manchanda V, Sachdev P, Saini RK, Joy M. Study of incidence and risk factors of surgical site infections in lower segment caesarean section cases of tertiary care hospital of north India. Indian J Med Microbiol. 2021;39(1):1-5. doi:10.1016/j.ijmmb.2020.11.005
23. Meng J, Zhu Y, Li Y, et al. Incidence and risk factors for surgical site infection following elective foot and ankle surgery: a retrospective study. J Orthop Surg Res. 2020;15(1):449. doi:10.1186/s13018-020-01972-4
24. Hou TY, Gan HQ, Zhou JF, et al. Incidence of and risk factors for surgical site infection after colorectal surgery: a multiple-center prospective study of 3,663 consecutive patients in China. Int J Infect Dis. 2020;96:676-681. doi:10.1016/j.ijid.2020.05.124
25. Taherpour N, Mehrabi Y, Seifi A, Eshrait B, Nazari SSH. Epidemiologic characteristics of orthopedic surgical site infections and under-reporting estimation of registries using capture-recapture analysis. BMC Infect Dis. 2021;21(1):3. doi:10.1186/s12879-020-05687-z






