



The Effect of Timing of Instillation Therapy on Outcomes and Costs for Patients Receiving Negative Pressure Wound Therapy
Abstract
Introduction. Although NPWTi-d has been associated with improved patient outcomes compared with NPWT alone, questions remain regarding the timing of NPWTi-d initiation. Objective. This study examined the effect of the timing of NPWTi-d initiation on patient outcomes and costs. Methods. A retrospective analysis was conducted utilizing a national, all-payer hospital database and included patients who received NPWTi-d in 2019. A matched cohort of 514 patients who received either early (within 1 day of NPWT application) or late (within 2–7 days of NPWT application) NPWTi-d initiation was created using propensity scoring. Differences in clinical outcomes and costs were compared using Wilcoxon rank sum, chi-square, and t tests. Results. Early NPWTi-d initiation was associated with significantly shorter NPWT duration (7.0 vs. 11.4 days; P <.0001) and inpatient stay (13.4 vs. 16.3 days; P <.0001) compared with late NPWTi-d initiation. Early NPWTi-d initiation was also associated with fewer debridements, OR visits during hospitalization, days until final OR procedure, and wound-related readmissions. Patients with early NPWTi-d initiation had a $10 877 lower mean cost of index admission (P <.0001), which included lower NPWT costs. Conclusion. Study data suggest that in these patients with wounds, early NPWTi-d initiation helped improve patient outcomes and reduced care costs.
Abbreviations
CCI, Charlson Comorbidity Index; ED, emergency department; ICD-10, International Statistical Classification of Diseases, Tenth Revision; LOS, length of stay; NPWT, negative pressure wound therapy; NPWTi-d, NPWT with instillation and dwell time; OR, operating room; PHD, Premier Healthcare Database; RCT, randomized controlled trial.
Introduction
Wounds are a major source of patient morbidity, health care utilization, and costs in the United States.1 NPWT was introduced over 20 years ago as a way to help improve wound management of both chronic and acute wounds.1 NPWT is used to remove infectious materials and exudate from wounds and has demonstrated effectiveness in promoting wound healing by stabilizing the wound bed, promoting continuous wound drainage, drawing the wound edges together, and stimulating granulation tissue growth.2-4 Use of NPWT has been associated with improved patient outcomes including earlier wound closure, reduced OR visits, reduced hospital LOS, fewer dressing changes, and reduced risk of amputation.5-9
The introduction of topical wound solution delivery (instillation therapy) in combination with NPWT (ie, NPWTi-d) has provided further benefits to promote wound healing.1 NPWTi-d provides wound cleansing through the periodic instillation of topical wound solutions directly over the wound bed with a set interval of dwell time followed by removal using negative pressure while the dressing remains in place. NPWTi-d has the added benefit of helping disrupt the bioburden cycle of complex wounds through the repeated cycles of wound cleansing with instillation and removal via negative pressure. Use of NPWTi-d has been associated with statistically significant reductions in wound size and bacterial bioburden10-13 as well as significant improvement in granulation tissue compared with NPWT.10,14 NPWTi-d use has been cited as a contributor to a reduction in the number of surgeries needed for debridement.1,3,9,15,16 Several studies have found NPWTi-d to be associated with fewer OR visits, reduced time to final surgical procedure, shorter hospital LOS, and a higher percentage of closed wounds before discharge compared with NPWT alone.9,15,17
Initially used in wounds that did not respond to traditional NPWT or as a last-resort therapy, NPWTi-d has gained traction as an integral part of wound management.18 Consensus guidelines published in 2020 recommend the use of NPWTi-d as an adjunct therapy along with debridement and systemic antibiotics for a wide variety of acute, chronic, and/or infected wounds, including traumatic, surgical, dehisced, and diabetic wounds as well as venous leg ulcers, pressure ulcers, and full-thickness burns, among other wound types.18 Although the guidelines state that NPWTi-d should be used within the framework of a clearly defined treatment plan and timetable,18 there are no specific guidelines concerning when NPWTi-d should be initiated, and questions remain regarding the timing of this therapy.1
Kaplan et al5 found that early initiation of NPWT (on day 1 or day 2 of treatment) resulted in a significant reduction in LOS, treatment days, intensive care unit days, and treatment costs compared with late initiation. Given that NPWTi-d can assist with early removal of exudate and provide wound cleansing that may help reduce bioburden,18 initiating instillation therapy in a timely fashion should help promote wound healing.1 It is important that the right therapy be administered at the right time, because complications that necessitate additional treatment (eg, infections) may occur in stalled wounds, resulting in increased LOS and spiraling costs of care.19 While the timing of NPWTi-d may affect patient outcomes, there is a gap in the literature concerning when to initiate NPWTi-d. The objective of this study was to examine the effect of timing of NPWTi-d initiation on patient outcomes and costs.
Materials and Methods
Study design
This study was a retrospective, matched cohort analysis using data from PHD (Premier, Inc.), the largest hospital administrative database in the United States. This database contains deidentified clinical and cost data from over 10 million inpatient admissions a year, representing approximately 25% of annual US inpatient admissions; it also contains data from outpatient visits to EDs, ambulatory surgery centers, and alternate sites of care.20 The study used deidentified data and was exempt from institutional review board review.
Study population
The study population included patients with an inpatient visit in 2019 who were treated with NPWTi-d (V.A.C. Veraflo Therapy, 3M) as indicated by hospital billing data. Patients who received NPWTi-d as their initial negative pressure treatment or within 1 day of NPWT application were categorized as having received early NPWTi-d initiation. Patients who received NPWTi-d within 2 to 7 days of initial NPWT application were categorized as having received late NPWTi-d initiation. For patients with multiple wounds in 2019, only the first documented wound in 2019 was included in the analysis.
Measures
Patient demographics as well as payor and admission type were obtained from the database. CCI scores were calculated for each patient based on comorbidities documented in the PHD in the 6 months prior to the index admission. Wound types were determined based on Current Procedural Terminology or ICD-10 diagnosis and procedure codes. Wound disruption or infection was determined using ICD-10 diagnosis codes. Clinical outcomes included inpatient LOS, duration of NPWT, number of debridements, number of OR visits, days between index admission and the last OR procedure performed during the index hospitalization, and all-cause and wound-related ED visits and readmissions within 30 days and 60 days. Cost outcomes included total cost of index admission, total NPWT cost during hospitalization, and readmission costs, wound costs, and overall health care costs at 30 days and 60 days. The date of the last OR procedure was based on the last day the patient had an OR department charge. ED visits, readmissions, and costs were considered wound-related if the admitting or primary diagnosis or primary procedure was wound-related or a patient had a Healthcare Common Procedure Coding System charge for NPWT or NPWTi-d during the visit. Overall health care costs were limited to inpatient and outpatient hospital visits at facilities that contributed data to the PHD. NPWT costs included vacuum pumps, canisters, cassettes, and dressings as well as other professional fees for NPWT or NPWTi-d and were obtained from billing data.
Statistical analysis
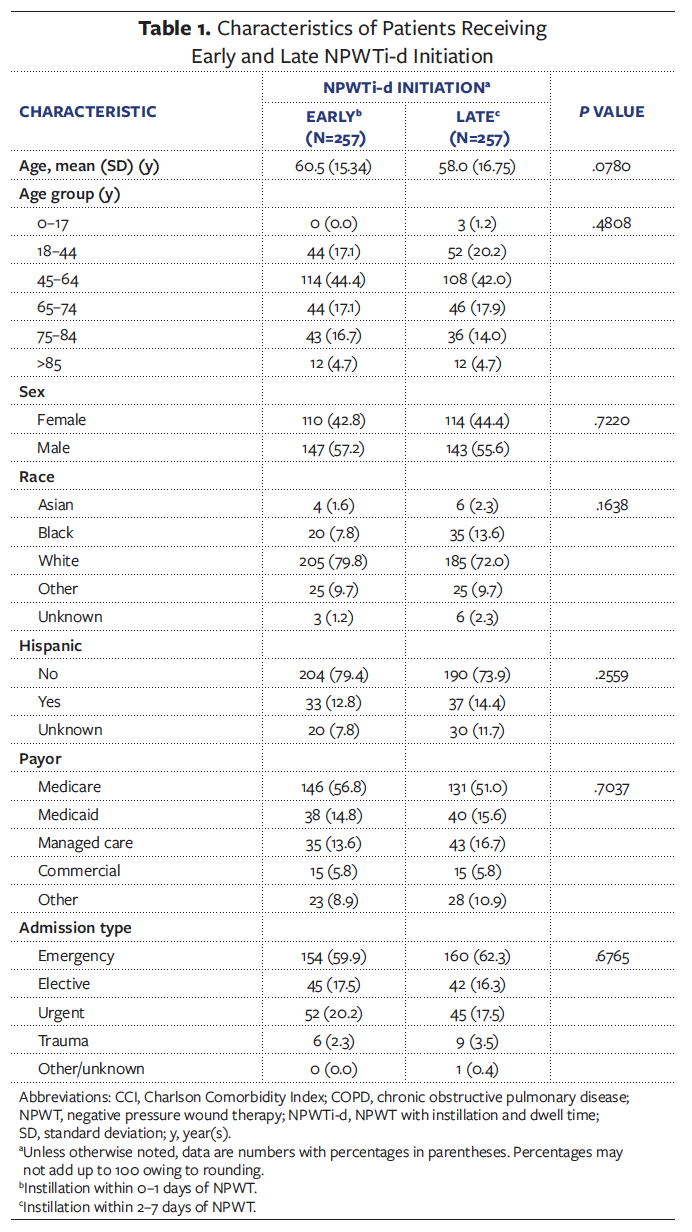
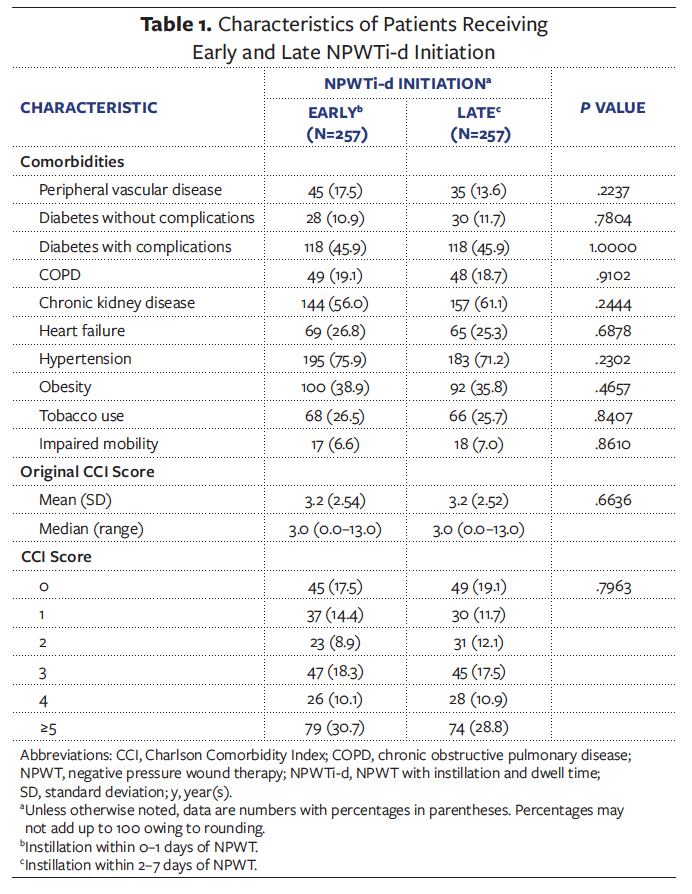
A matched cohort of 514 patients (257 per group) was created using propensity scoring. Propensity scores for each patient were modeled using logistic regression with a binary indicator to designate early versus late NPWTi-d initiation as the dependent variable and a vector of the following independent variables: age, sex, race, ethnicity, payor type, admission type (elective or not elective), CCI score, and comorbid conditions (Table 1), as well as wound type, presence of wound disruption or infection, and day of NPWT initiation. Patients who received early NPWTi-d initiation were matched to patients who received late NPWTi-d initiation using the nearest neighbor matching technique with an exact match on wound type. There were no statistically significant differences between groups for the independent variables that were included in the model following matching, which indicates that the groups were balanced in terms of observed covariates. Differences in outcomes between groups were compared using t tests and Wilcoxon rank sum tests for continuous variables and chi-square tests for categorical variables. Patients with an index LOS greater than 90 days and/or outliers with inpatient costs above the 99th percentile were excluded from the final analysis.
Results
There were no significant differences in patient demographics between the matched groups (Table 1). Mean age was 60.5 years for patients who received early initiation and 58.0 years for those who received late initiation. In both groups, more than half of the patients were on Medicare and over 60% of patients had emergency admissions. Many patients had comorbidities, with the most common including hypertension, chronic kidney disease, diabetes with complications, and obesity. The mean CCI score was 3.2 for both groups.
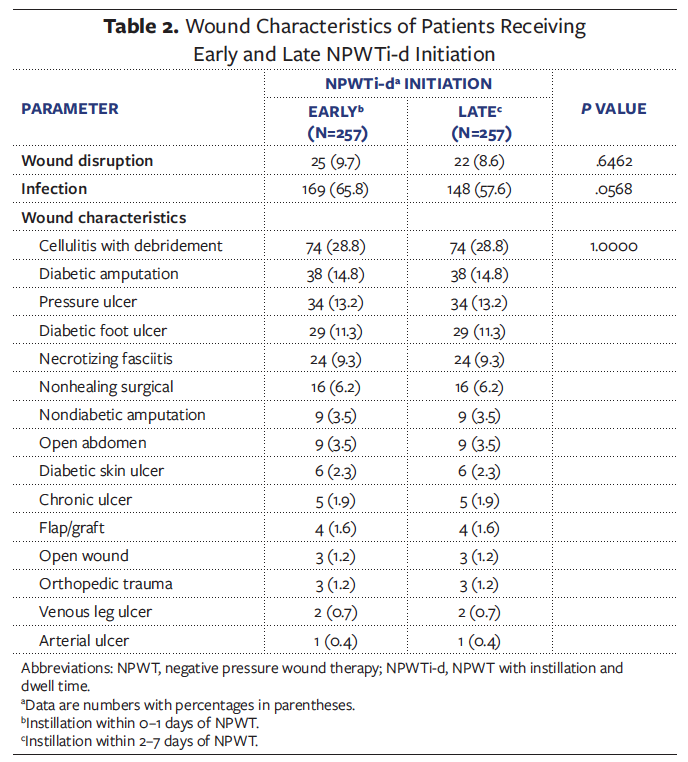
The most common wounds for both groups were cellulitis with debridement (28.8%), diabetic amputation (14.8%), pressure ulcer (13.2%), and diabetic foot ulcer (11.3%) (Table 2). Wound disruptions were present in 9.7% of patients who received early NPWTi-d initiation and 8.6% of patients who received late NPWTi-d initiation, and infection was present in 65.8% and 57.6% of these patient groups, respectively.
Clinical outcomes for the 2 groups are shown in Table 3. Initiation of NPWT wound therapy occurred around day 4 of the hospital stay for patients in both groups; however, patients who received early initiation of NPWTi-d therapy spent 4.4 fewer days on NPWT (7.0 days vs. 11.4 days; P <.0001). Overall hospital LOS was significantly shorter for patients who received early NPWTi-d initiation (13.4 days vs. 16.3 days; P <.0001).
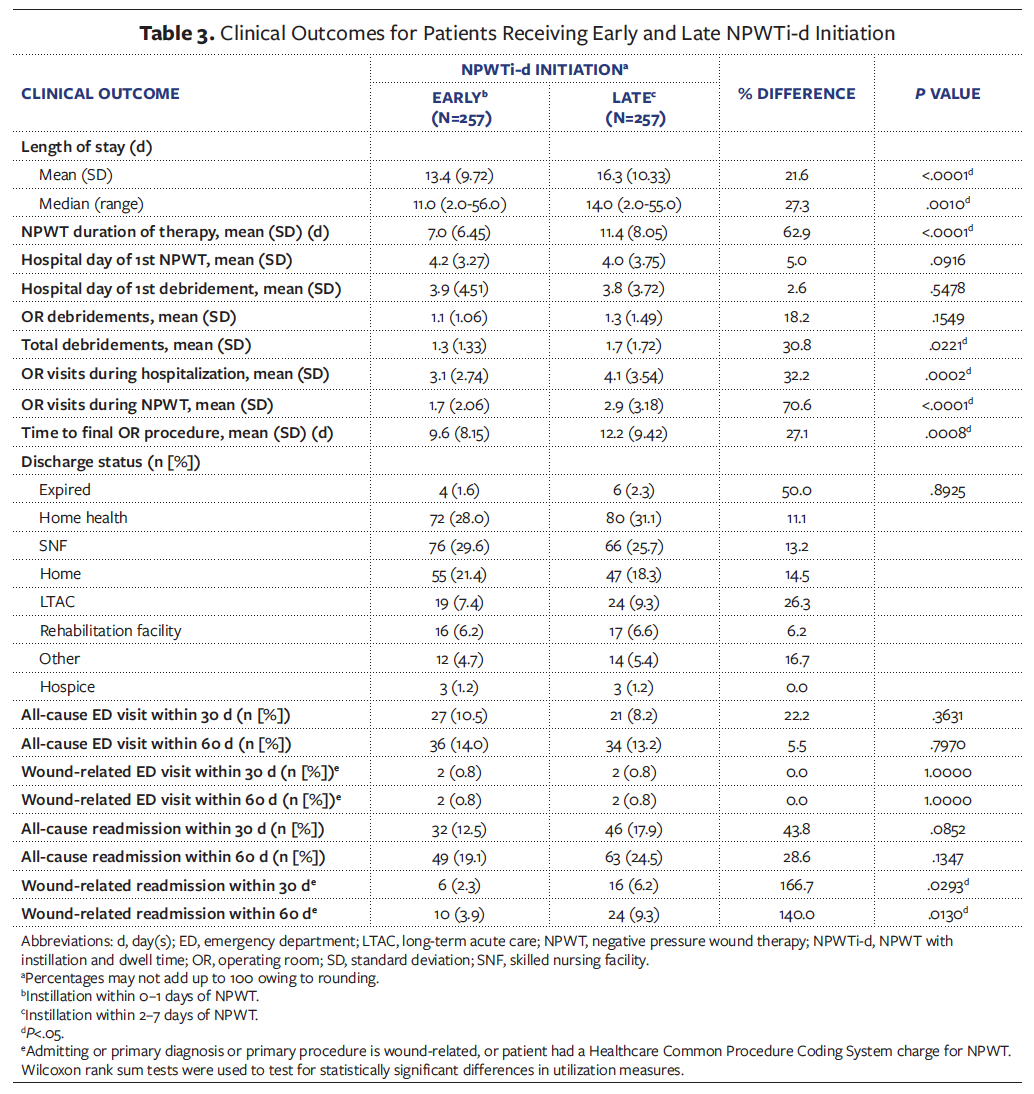
There were no significant differences between groups in terms of hospital day of first debridement or number of OR debridements. Patients who received early initiation of NPWTi-d underwent significantly fewer total debridements (1.3 vs. 1.7; P =.0221) and had fewer trips to the OR during hospitalization (3.1 vs. 4.1; P =.0002) and while receiving NPWT (1.7 vs. 2.9; P <.0001). The number of days until the final OR procedure was also significantly shorter for patients who received early NPWTi-d initiation (9.6 vs. 12.2; P =.0008).
There were no significant differences between groups in discharge status, and most patients were discharged to home, home health care, or a skilled nursing facility. Rates of all-cause and wound-related ED visits and readmissions were similar between groups; however, patients who received initiation of NPWTi-d had fewer wound-related readmissions at 30 days (6 vs. 16; P =.0293) and 60 days (10 vs. 24; P =.0130).
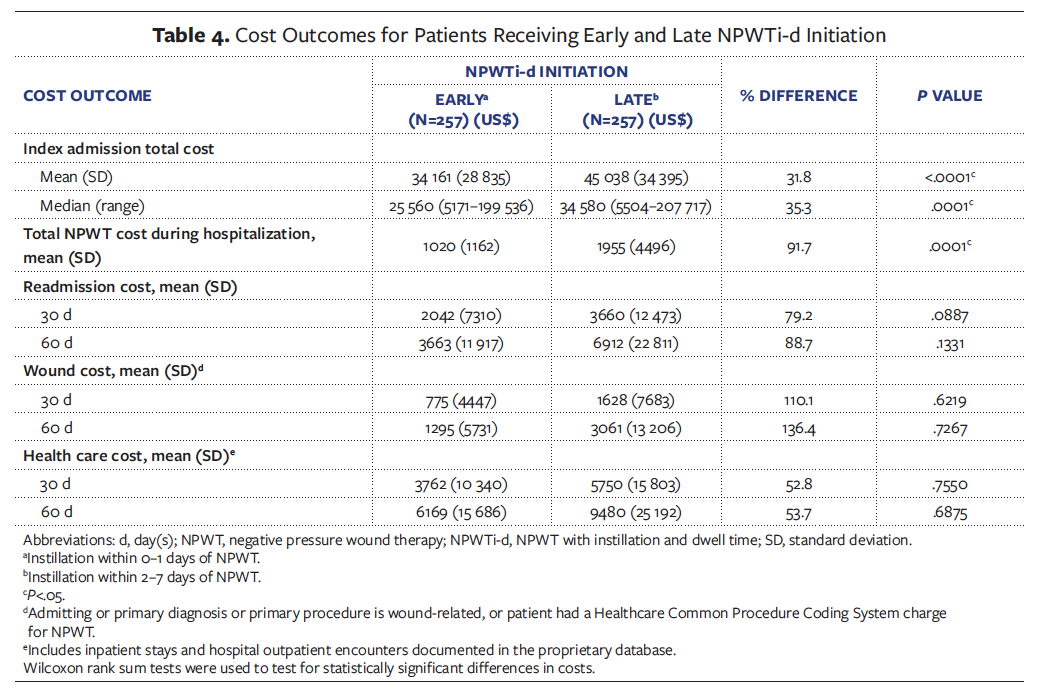
Cost outcomes for both groups are shown in Table 4. The mean total cost of index admission was $10 877 less for patients who received early initiation of NPWTi-d ($34 161 vs. $45 038; P <.0001). This cost difference included lower mean total NPWT cost ($1020 vs. $1955; P =.0001) for patients who received early NPWTi-d initiation. There were no significant differences between groups in 30-day or 60-day readmission costs, wound costs, or health care costs.
Discussion
NPWTi-d is an advancement from NPWT, because the addition of topical wound solution to the wound bed can facilitate wound cleansing and more efficient removal of exudates and infectious material.14,21 Although NPWTi-d was once primarily used as a last resort therapy, there is growing evidence indicating that it can be an integral component of care for complex wounds and can be considered among first-line treatments. NPWTi-d may be useful for patients who are poor surgical candidates, those who cannot tolerate bedside debridement, and those who are in need of wound cleansing as part of a multidisciplinary approach to wound care.22
In the current study, initiating NPWTi-d as the first type of NPWT or within 1 day of NPWT was associated with significant improvements in patient outcomes and reductions in cost. Patients who received early initiation of NPWTi-d spent fewer days on NPWT and had a shorter hospital LOS compared with patients who received late initiation of NPWTi-d, resulting in an average reduction in care costs of over $10 000. Early initiation of NPWTi-d was also associated with a significant reduction in total debridements (P =.0221), trips to the OR during hospitalization (P =.0002), trips to the OR while receiving NPWT (P <.0001), number of days to the final OR procedure (P =.0008), and wound-related readmissions (within 30 days [P =.0130], within 60 days [P =.0293]).
No other studies have compared outcomes between patients receiving NPWTi-d as an initial therapy versus those receiving NPWTi-d after several days of NPWT without instillation. One study examined use of NPWTi-d alone versus NPWTi-d followed by NPWT without instillation.3 In that small case series, Anchalia et al3 found NPWTi-d to be more effective than traditional NPWT in fast clearance of bioburden of wounds and preparing wounds for split-thickness grafting. However, study findings indicated that 2 to 3 treatments with NPWTi-d were sufficient to reduce bioburden, after which NPWT without instillation could be used as a step-down therapy to continue to prepare the wound bed for skin grafting.
Several studies have indicated that patients who receive NPWTi-d have significantly better outcomes than patients who receive other common wound therapies. In a recent meta-analysis including 13 studies with 720 patients, Gabriel et al23 found that the wounds of patients who received NPWTi-d were more likely to close, were ready for closure faster, and had a greater percent reduction in bacterial count compared with wounds of patients who received comparative therapies, including NPWT without instillation. Patients who received NPWTi-d also had fewer days of therapy and underwent fewer surgical debridements. No differences in LOS were observed between groups in the meta-analysis, as observed in the current study, but several of the included individual studies noted significant reduction in LOS for patients who received NPWTi-d compared with patients who received NPWT without instillation.9,15
Management of complex surgical wounds is a challenging and growing problem, with more patients being hospitalized with infected wounds and the average age and number of comorbidities of patients also increasing.4,18 Wound infections are among the most expensive complications following surgery and are a source of bacteria that drive nosocomial infection rates in hospitals.24 In the current study, early initiation of NPWTi-d was associated with a more than $10 000 reduction in costs for the index admission, including almost $1000 in reduced costs for NPWT. No large comparative studies have been conducted to assess the overall value of NPWTi-d versus other wound management strategies. However, using inputs from the meta-analysis conducted by Gabriel et al,23 an economic model was developed to determine the potential cost savings of NPWTi-d versus control therapies.21 The total potential per patient savings for patients who received NPWTi-d versus control therapies was estimated to be $33 388 in the United States, €8467 in Germany, and £5626 in the United Kingdom. These cost savings were the result of shorter inpatient LOS, shorter duration of NPWT, and fewer OR visits for surgical debridements.21
Although increasing numbers of small studies have demonstrated improved clinical outcomes and reduced costs for patients receiving NPWTi-d, large institutional or multi-institutional prospective RCTs are lacking.21-23 The current study is not an RCT, but it contributes to the existing knowledge base by examining the effect of the timing of instillation therapy across wound types using a hospital database representing 25% of all hospital admissions in the United States.20 The findings of the current study suggest that starting with NPWTi-d as opposed to adding instillation after several days of NPWT significantly improved patient outcomes in terms of total debridement, OR trips, OR trips during NPWT, days until final OR procedure, and readmission within 30 days and 60 days to help reduce costs of care. The benefits of early NPWTi-d initiation observed in this study are similar to those associated with NPWTi-d use over control therapies in other studies, including NPWT without instillation.
Limitations
This study has several limitations. Study data were obtained through the provision of routine patient care rather than as part of a targeted research study and were extracted from a hospital administrative database. Data points regarding use and timing of NPWTi-d and NPWT were extracted from billing data, which may contain inaccuracies. The database did not contain wound-specific data, including size and other characteristics, which prevented examination of the effect of NPWTi-d timing on wound healing. Instead, the effect of NPWTi-d on outcomes such as duration of NPWT, LOS, number of debridements, number of trips to the OR, and other health care utilization measures was examined. The lack of wound-specific data in the database also limited the ability to fully assess whether there were clinical indications that may have prompted a delay in NPWTi-d initiation for some patients, such as severe necrotizing infections requiring more aggressive debridements. Decisions concerning the timing of NPWTi-d initiation may vary by surgeon and may be based on patient-specific situations that may not be documented in structured data fields. Underlying differences in patient characteristics or undocumented wound characteristics may have influenced the timing of NPWTi-d and contributed to the observed differences in outcomes between study groups, including increases in OR visits and costs for patients who received late NPWTi-d initiation. The inability to adjust for unobserved covariates is an inherent limitation of retrospective studies; however, an attempt was made to control for differences between therapy groups using propensity score matching on observed covariates, including wound type and the presence of infection or wound disruption.
Conclusion
The findings from this study suggest that in patients with wounds, starting with NPWTi-d instead of NPWT without instillation is a successful strategy for helping to improve clinical outcomes and reduce costs of care. However, more evidence, particularly in the form of large-scale randomized trials, is needed to determine the optimal use of NPWTi-d as well as to maximize the clinical benefits and cost-effectiveness of the therapy.
References
1. Gupta S, Gabriel A, Lantis J, Téot L. Clinical recommendations and practical guide for negative pressure wound therapy with instillation. Int Wound J. 2016;13(2):159-174.
2. Diehm YF, Loew J, Will PA, et al. Negative pressure wound therapy with instillation and dwell time (NPWTi-d) with V. A. C. VeraFlo in traumatic, surgical, and chronic wounds--a helpful tool for decontamination and to prepare successful reconstruction. Int Wound J. 2020;17(6):1740-1749.
3. Anchalia M, Upadhyay S, Dahiya M. Negative pressure wound therapy with instillation and dwell time and standard negative pressure wound therapy in complex wounds: are they complementary or competitive? Wounds. 2020;32(12):E84-e91.
4. Kim PJ, Silverman R, Attinger CE, Griffin L. Comparison of negative pressure wound therapy with and without instillation of saline in the management of infected wounds. Cureus. 2020;12(7):e9047.
5. Kaplan M, Daly D, Stemkowski S. Early intervention of negative pressure wound therapy using Vacuum-Assisted Closure in trauma patients: impact on hospital length of stay and cost. Adv Skin Wound Care. 2009;22(3):128-132.
6. Apelqvist J, Armstrong DG, Lavery LA, Boulton AJ. Resource utilization and economic costs of care based on a randomized trial of vacuum-assisted closure therapy in the treatment of diabetic foot wounds. Am J Surg. 2008;195(6):
782-788.
7. Dowsett C, Davis L, Henderson V, Searle R. The economic benefits of negative pressure wound therapy in community-based wound care in the NHS. Int Wound J. 2012;9(5):544-552.
8. Driver VR, Blume PA. Evaluation of wound care and health-care use costs in patients with diabetic foot ulcers treated with negative pressure wound therapy versus advanced moist wound therapy. J Am Podiatr Med Assoc. 2014;104(2)
:147-153.
9. Gabriel A, Kahn K, Karmy-Jones R. Use of negative pressure wound therapy with automated, volumetric instillation for the treatment of extremity and trunk wounds: clinical outcomes and potential cost-effectiveness. Eplasty. 2014;14:e41.
10. Giri P, Krishnaraj B, Chandra Sistla S, et al. Does negative pressure wound therapy with saline instillation improve wound healing compared to conventional negative pressure wound therapy? - a randomized controlled trial in patients with extremity ulcers. Ann Med Surg (Lond). 2021;61:73-80.
11. Gabriel A, Shores J, Heinrich C, et al. Negative pressure wound therapy with instillation: a pilot study describing a new method for treating infected wounds. Int Wound J. 2008;5(3):399-413.
12. Kim PJ, Lavery LA, Galiano RD, et al. The impact of negative-pressure wound therapy with instillation on wounds requiring operative debridement: pilot randomised, controlled trial. Int Wound J. 2020;17(5):1194-1208.
13. Yang C, Goss SG, Alcantara S, Schultz G, Lantis II JC. Effect of negative pressure wound therapy with instillation on bioburden in chronically infected wounds. Wounds. 2017;29(8):240-246.
14. Lessing C, Slack P, Hong KZ, Kilpadi D, McNulty A. Negative pressure wound therapy with controlled saline instillation (NPWTi): dressing properties and granulation response in vivo. Wounds. 2011;23(10):309-319.
15. Kim PJ, Attinger CE, Steinberg JS, et al. The impact of negative-pressure wound therapy with instillation compared with standard negative-pressure wound therapy: a retrospective, historical, cohort, controlled study. Plast Reconstr Surg. 2014;133(3):709-716.
16. Chowdhry SA, Wilhelmi BJ. Comparing negative pressure wound therapy with instillation and conventional dressings for sternal wound reconstructions. Plast Reconstr Surg Glob Open. 2019;7(1):e2087.
17. Yang CK, Alcantara S, Goss S, Lantis II JC. Cost analysis of negative-pressure wound therapy with instillation for wound bed preparation preceding split-thickness skin grafts for massive (>100 cm(2)) chronic venous leg ulcers. J Vasc Surg. 2015;61(4):995-999.
18. Kim PJ, Attinger CE, Constantine T, et al. Negative pressure wound therapy with instillation: international consensus guidelines update. Int Wound J. 2020;17(1):174-186.
19. Dowsett C. Breaking the cycle of hard-to-heal wounds: balancing cost and care. Wounds
International. 2015;6(2):17-21.
20. Premier Healthcare Database: Data that Informs and Performs. Premier Applied Sciences, Premier Inc.;2020.
21. Kim PJ, Lookess S, Bongards C, Griffin LP, Gabriel A. Economic model to estimate cost of negative pressure wound therapy with instillation vs control therapies for hospitalised patients in the United States, Germany, and United Kingdom. Int Wound J. 2022;19(4):888-894.
22. Arowojolu OA, Wirth GA. Sacral and ischial
pressure ulcer management with negative-
pressure wound therapy with instillation and dwell. Plast Reconstr Surg. 2021;147(1S-1):61S-67S.
23. Gabriel A, Camardo M, O'Rorke E, Gold R, Kim PJ. Effects of negative-pressure wound therapy with instillation versus standard of care in multiple wound types: systematic literature review and meta-analysis. Plast Reconstr Surg. 2021;147(1s-1):68s-76s.
24. Sen CK, Gordillo GM, Roy S, et al. Human skin wounds: a major and snowballing threat to public health and the economy. Wound Repair Regen. 2009;17(6):763-771.





