



Erosive Pustular Dermatosis of the Scalp: Clinicopathological Correlation Leading to a Definition of Diagnostic Criteria
Abstract
Introduction. Erosive pustular dermatosis of the scalp (EPDS) is frequently misdiagnosed as epithelial tumor or trauma. To the authors’ knowledge, no international guidelines or consistent recommendations for treatment of EPDS exist, and histological findings often are labeled as nonspecific. Objective. This study aimed to identify clinical and histological characteristics unique to EPDS to aid diagnosis. Materials and Methods. The biopsies of 21 patients (age range, 73–90 years) with EPDS and who were diagnosed and treated at the Department of Dermatology at University of Leipzig Medical Center and the Asklepios Medical Center, Weißenfels, Germany, were reevaluated by dermatopathologists. Results were correlated with the clinical findings and course. Results. Erosive pustular dermatosis of the scalp was observed in elderly patients with androgenetic alopecia and field cancerization of the capillitium; most patients had multiple comorbidities. Therapy used to treat actinic keratosis lesions (eg, imiquimod, ingenol mebutate), photodynamic therapy, cryotherapy, trauma, and surgery all were found to have predisposed for or led to EPDS. Erosive pustular dermatosis of the scalp presented clinically as exophytic crusts and pus overlying shiny granulation tissue. Histopathological findings demonstrated an ulcerated epidermis and dermal infiltrates dominated by lymphocytes together with a multitude of plasma cells. Plasma cells were found in all 21 biopsies and represented a common criterion for the correct diagnosis. The erosive lesions healed well within weeks after therapy with topical steroids. Conclusions. Chronic, poorly healing lesions with crusts and pus over shiny granulation tissue on the scalp are suggestive of EPDS, which should be confirmed by biopsy. Histological clues to a diagnosis of EPDS include dermal infiltrates of plasma cells and lymphocytes. The topical application of high-potency steroids showed great effectiveness in the present study.
How Do I Cite This?
Reschke R, Grunewald S, Paasch U, Averbeck M, Simon JC, Wetzig T. Erosive pustular dermatosis of the scalp: clinicopathological correlation leading to a definition of diagnostic criteria. Wounds. 2021;33(6):143–146. doi:10.25270/wnds/2021.040721.01
Introduction
Erosive pustular dermatosis of the scalp (EPDS) usually affects the scalp of older men. Different stimuli are known to cause these inflammatory lesions, such as trauma,1 previous surgery,2 imiquimod,3 ingenol mebutate,4 and photodynamic therapy (PDT).5 The etiology of the disease remains unclear. The histological characteristics of EPDS have not been consistently defined. A mixed inflammatory infiltrate of macrophages, neutrophil and eosinophil granulocytes, and plasma cells has been reported. The findings are often interpreted as nonspecific.6
Materials and Methods
Patient selection
Data were retrospectively collected from patients (age range, 73–90 years) who were treated for EPDS at the University of Leipzig Medical Center and Asklepios Medical Center, Weißenfels, Germany. Initially, patients were admitted for suspected squamous cell cancers of the scalp. All lesions were biopsied for histopathological evaluation.
Clinical and histopathological analyses
Each patient’s clinical course and background were obtained from medical records. All tissue biopsies were taken from the center of the lesions, then screening was conducted for tumors and characteristic cellular patterns in hematoxylin-eosin staining.
Diagnostic criteria
Clinical criteria consisted of the following: chronic, poorly healing lesions on the scalp (purulent crusts overlying shiny granulation tissue); elderly patients; external injury to the skin most frequently damaged by actinic keratoses (eg, PDT, cryotherapy, imiquimod, surgery); skin in marginal areas easily detachable by forceps; and excellent response to topical steroids. The histopathological criterion was prominent dermal infiltrates of plasma cells and lymphocytes in a perivascular pattern or spread over the entire dermis.
Results
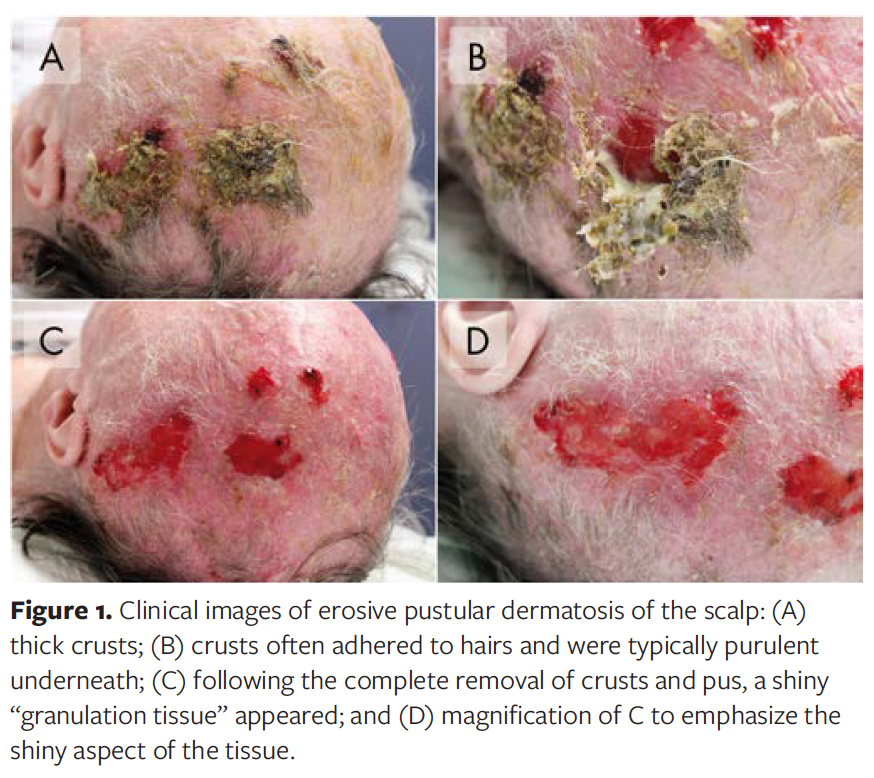
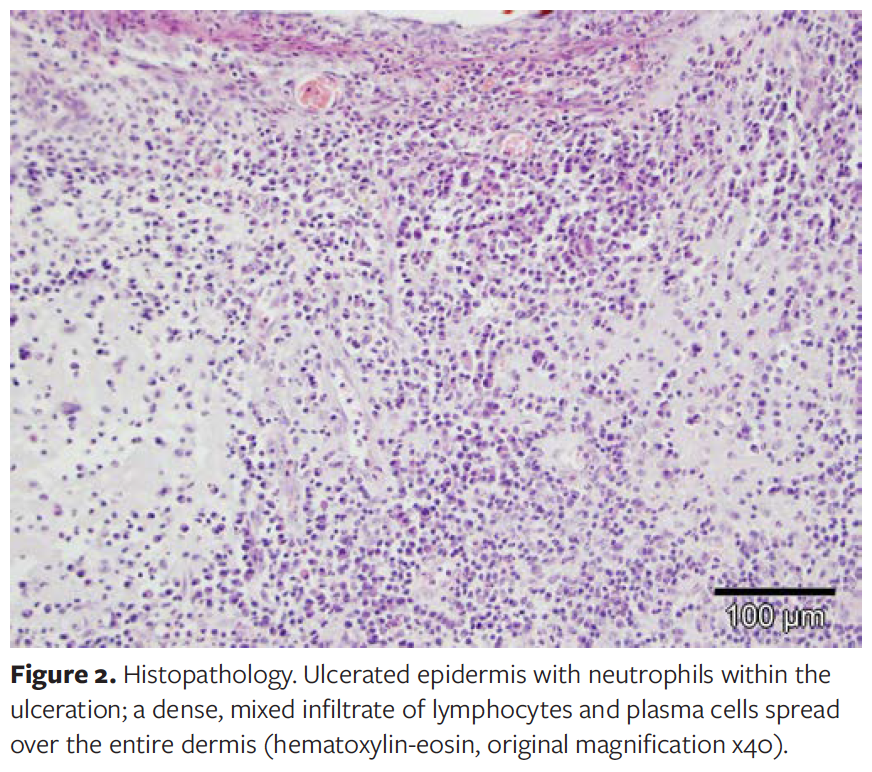
The analyzed cohort consisted of 21 patients (18 men, 86%; 3 women, 14%) with EPDS. Typically, patients displayed thick crusts. After removing the crusts, pus and a shiny, glass-like layer of hypertrophic granulation tissue surfaced (Figure 1). Dermatopathological evaluation revealed a dermal infiltrate of lymphocytes and plasma cells in all 21 patients. These lymphoplasmacytic infiltrates were predominantly located in a perivascular pattern in the superficial and mid-dermis. In severe cases of EPDS, plasma cells formed dense infiltrates in the entire dermis (Figure 2) and appeared polyclonal. Neutrophils were detectable around the ulceration in 8 of 21 patients (38%). Name-giving pustules were not observed in any case, most likely owing to the removal of purulent crusts before the biopsy. In the punch biopsies residual hair follicles were rarely observed, and those that existed were located mainly in the marginal areas. The latter finding corresponds to the clinical observation of hair loss caused by EPDS.
Triggers for EPDS in the patients in this study were cryotherapy, PDT, 5-fluorouracil, diclofenac gel, surgery, donor sites of split-thickness skin grafts, and trivial injuries of the scalp. In all cases, the skin had been damaged by actinic keratoses and skin atrophy. Fifteen of 21 patients (71%) developed EPDS in areas of the scalp affected by androgenetic alopecia. The condition existed between 3 and 24 months prior to the first consultation with a health care professional. Previous therapeutic attempts with disinfection and modern wound dressings were unsuccessful. Some patients had positive microbiological smears, showing colonization with Staphylococcus aureus or with Pseudomonas or Candida species. Although local antibiotic and antimycotic therapies achieved the eradication of bacteria and Candida species, the lesions did not heal. Seven patients also had diabetes mellitus. However, the vascular supply to the skin was intact in all patients. None of the patients were immunosuppressed. Erythrocyte sedimentation rate (ESR) was elevated in all 5 patients investigated. Elevated ESR seemed to correlate with disease severity as well as with the density of plasma cell infiltrates in the biopsies. These factors must be controlled in larger patient cohorts, however. In contrast, C-reactive protein was within normal range or only mildly elevated. Differential diagnoses that are associated with an elevated ESR, such as lymphoma, plasmocytoma, leukemia, other malignancies, severe anemia, hemolytic syndrome, nephrotic syndrome, de Quervain disease, polymyalgia rheumatica, giant cell arteritis, systemic lupus erythematosus, and severe systemic infections, were excluded in these patients.
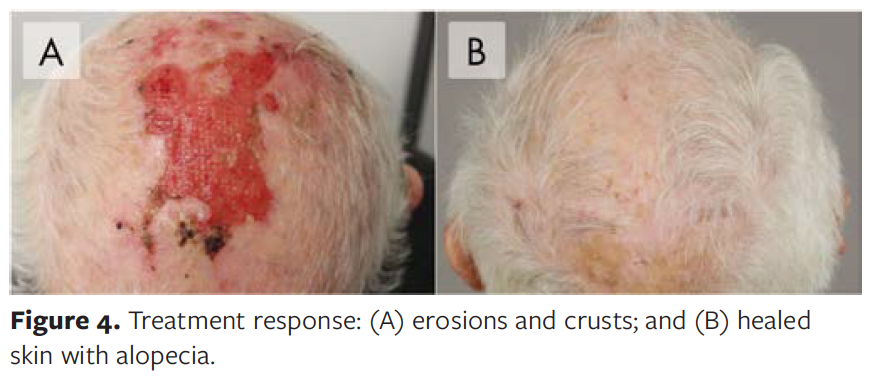
All patients were treated with topical glucocorticoids (class III or IV), topical disinfection, and, if necessary, a topical antibiotic. This treatment resulted in complete healing within a few weeks (mean, 2.5 weeks) (Figure 3, Figure 4) as well as normalization of the ESR in all patients. One patient experienced recurrence; however, the patient responded well to additional treatment with topical steroids.
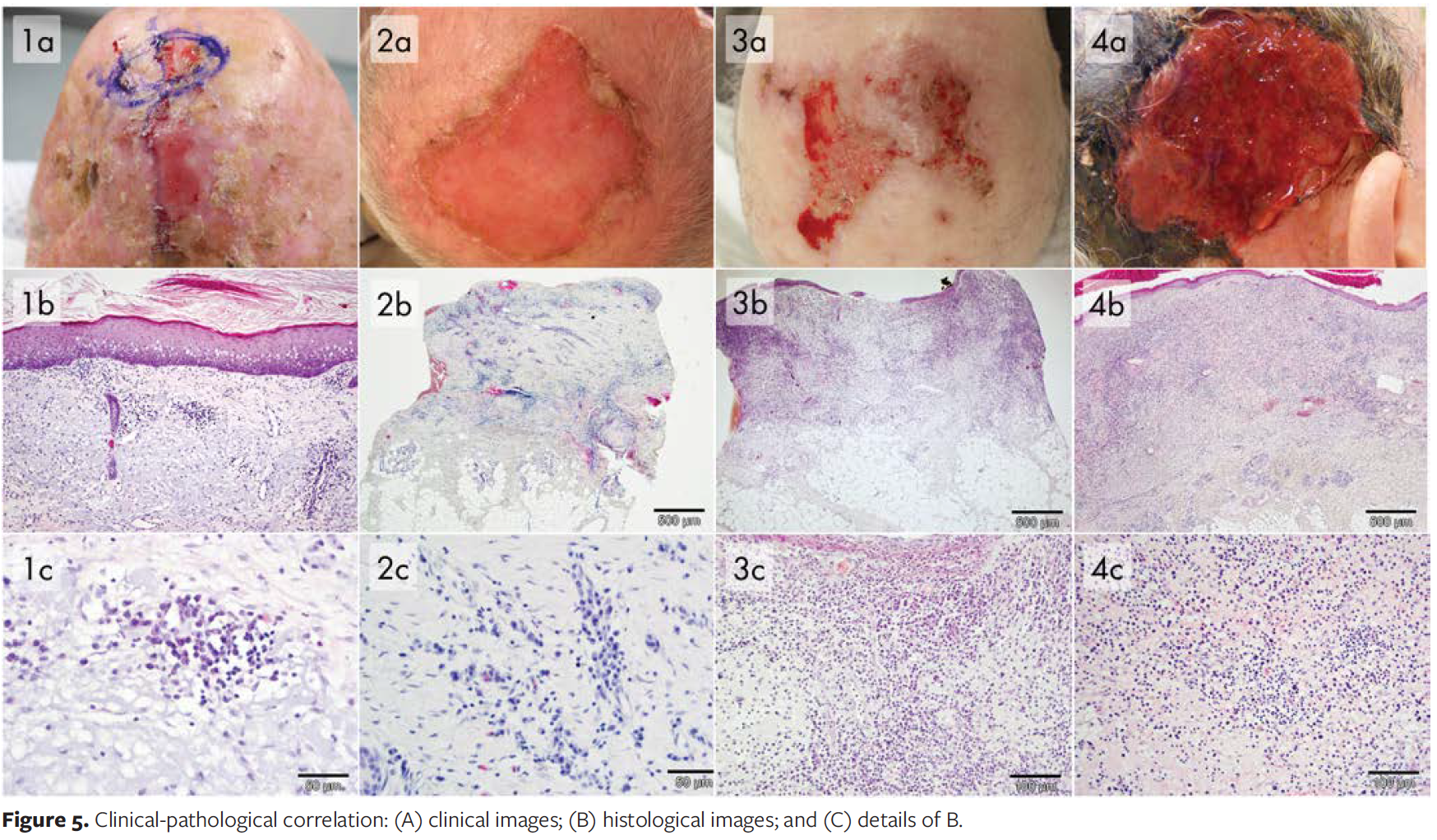
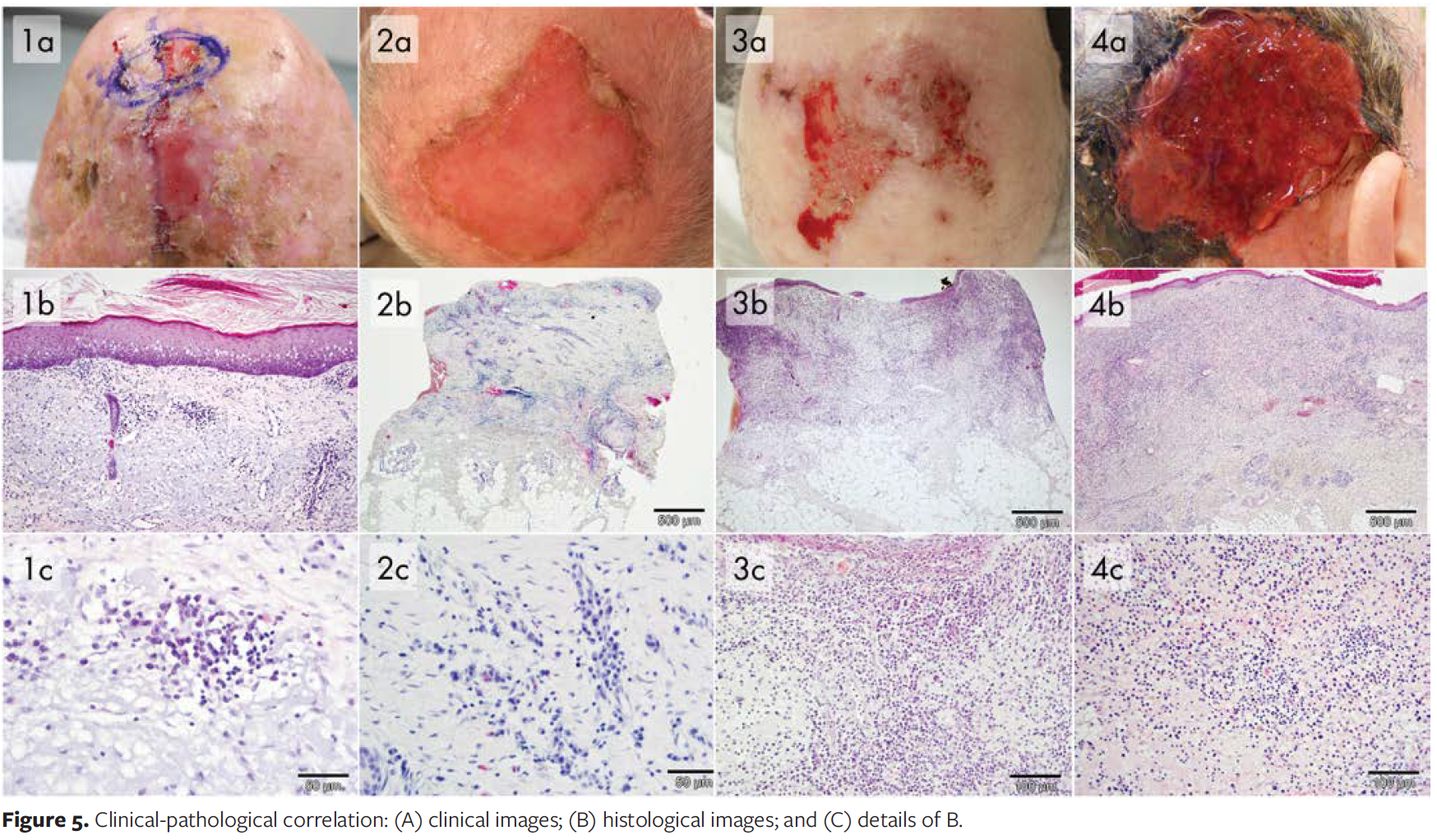
Secondary alopecia was a typical effect of EPDS, notably owing to the inflammatory destruction of hair follicles (Figure 5). However, most patients in this study initially presented with androgenetic alopecia.
Discussion
Erosive pustular dermatosis of the scalp can clinically imitate other diseases, such as cutaneous squamous cell carcinoma, basal cell carcinoma, Brunsting-Perry cicatricial pemphigoid, bacterial or mycotic infections, and folliculitis decalvans. After the exclusion of epithelial tumor growth, EPDS is thought to be a nonspecific wound healing disorder,6 and clear diagnostic criteria for EPDS are lacking. For this reason, in-depth clinicopathological correlations were performed in this study to review the criteria defining this disease.
Erosive pustular dermatosis of the scalp usually develops on previously damaged skin of the scalp in elderly persons. Most often, patients have previously undergone treatment for actinic keratosis or field cancerization using methods that have a proinflammatory effect or that traumatize the epidermis and superficial dermis, such as PDT or surgery. Elderly patients tend to frequently scratch preexisting lesions on their scalp, which could in turn further aggravate inflammatory processes.7 In some cases, the resulting EPDS remains itchy.8 These inflammatory or traumatic insults trigger the accumulation of inflammatory cells, such as lymphocytes and plasma cells, which further contribute to this wound healing disorder. The literature indicates that both women and men are affected.8-10 In the present study, there were more male patients than female patients, most likely owing to the higher frequency of androgenetic alopecia and subsequently actinic keratosis in this sun-exposed area. One side effect of EPDS is secondary alopecia owing to the destruction of hair follicles by chronic inflammation. The authors of this study hypothesize that missing or destructed hair follicles delay the re-epithelialization process. This has already been shown in experimental models, in which half of the keratinocytes involved in wound healing are derived from adnexal structures.11
Hence, the healing process is slowed because it must be initiated from the marginal areas of the lesion. The epidermis is easily detachable in the marginal area, which could result in increased size of the lesion. However, the detachable epidermis could be used as an additional clinical sign of EPDS.
In patients with normal C-reactive protein values, the increased ESR might reflect the autoinflammatory nature of the disease. Larger trials are necessary to determine whether ESR monitoring might be useful as a parameter for disease activity and the treatment response. In addition to the existing literature concerning histopathologic evaluation of EPDS, the authors of the present study postulate that the occurrence of plasma cells in the dermis is the most characteristic histological criterion of EPDS (Figure 2, Figure 5). In patients with EPDS, tissue biopsies of the scalp show the occurrence of plasma cells to be significantly more extensive than in patients who do not exhibit EPDS. Other authors also describe dermal plasma cells but characterize neutrophils as the predominant histopathological feature.12 Similarities with other neutrophilic dermatoses, such as pustular pyoderma gangrenosum, have been proposed. The authors of the present study observed neutrophils mostly located around ulcerations. Thus, neutrophils can be interpreted as part of the acute inflammation.13 Plasma cells and lymphocytes prevail in the chronic status of EPDS, however. Clinically, EPDS is easy to distinguish from other dermatoses with prominent plasma cells, such as lues, Lyme disease, or erythema elevatum diutinum. Infiltrates of lymphocytes and plasma cells can also occur in actinic keratoses. However, lymphoplasmacytic infiltrates of EPDS are much more pronounced and affect deeper dermal layers. There is reason to believe that the peritumoral inflammation remains and even intensifies after healing of the precancerous lesion being triggered by external stimuli (eg, surgery, cryotherapy). The exact and early diagnosis of EPDS prevents futile treatments with expensive wound care products. Instead, patients are sufficiently treated with topical steroids. Other topical therapies, such as 5% dapsone gel or tacrolimus, have shown positive effects in smaller case series.10,14 Erosive pustular dermatosis of the scalp relapse occurs but responds well to repeated treatment with topical steroids.
Limitations
The size of this study was small. The ESR was measured in only 5 patients. Larger studies are necessary to confirm our findings. In future studies, biopsies of lymphoplasmacytic dermatosis of the scalp could be compared to actinic keratosis or dermatosis with dense plasma cell infiltrate.
Conclusions
Erosive pustular dermatosis of the scalp can be clinically described as consisting of purulent crusts and underlying granulation tissue on actinically damaged skin following topical therapies (eg, PDT, cryotherapy, imiquimod, surgery). Histopathologically, EPDS is always characterized by dermal infiltrates of plasma cells and lymphocytes. The name erosive pustular dermatosis of the scalp is misleading; lymphoplasmacytic dermatitis of the scalp may be a more accurate term for the condition. In the authors' opinion, the histological finding of dermal plasma cells is the most characteristic diagnostic criterion for EPDS and can ensure a correct diagnosis. With proper diagnosis, EPDS can be successfully treated with topical steroids.
Acknowledgments
Authors: Robin Reschke, MD1; Sonja Grunewald, MD1; Uwe Paasch, MD1; Marco Averbeck, MD1; Jan C. Simon, MD1; and Tino Wetzig, MD2
Affiliations: 1Department of Dermatology, University of Leipzig Medical Center, Germany; 2Department of Dermatology, Dermatosurgery and Allergology, Asklepios Medical Center, Weißenfels, Germany
Contributions: Robin Reschke, MD, and Sonja Grunewald, MD, contributed equally to this study.
Correspondence: Robin Reschke, University of Leipzig Medical Center, Philipp-Rosenthal Str. 23, 04103 Leipzig, Germany; robin.reschke@medizin.uni-leipzig.de
Disclosure: The authors disclose no additional conflicts of interest.
References
1. Grattan CE, Peachey RD, Boon A. Evidence for a role of local trauma in the pathogenesis of erosive pustular dermatosis of the scalp. Clin Exp Dermatol. 1988;13(1):7–10. doi:10.1111/j.1365-2230.1988.tb00639.x
2. Roche-Kubler B, Monnin C, Aubin F, Dupond AS. Erosive pustular dermatosis of the scalp and thigh associated with skin graft recipient and donor sites. Eur J Dermatol. 2015;25(3):269–271. doi:10.1684/ejd.2015.2528.
3. Vaccaro M, Barbuzza O, Guarneri B. Erosive pustular dermatosis of the scalp following treatment with topical imiquimod for actinic keratosis. Arch Dermatol. 2009;145(11):1340–1341. doi:10.1001/archdermatol.2009.278
4. Rongioletti F, Chinazzo C, Javor S. Erosive pustular dermatosis of the scalp induced by ingenol mebutate. J Eur Acad Dermatol Venereol. 2016;30(11):e110–e111. doi:10.1111/jdv.13350
5. Guarneri C, Vaccaro M. Erosive pustular dermatosis of the scalp following topical methylaminolaevulinate photodynamic therapy. J Am Acad Dermatol. 2009;60(3):521–522. doi:10.1016/j.jaad.2008.09.006
6. Kowalzick L, Marcus EL, Gradistanac B, et al. Persistierende wundheilungsstörungen nach lokaltherapie von feldkanzerisierung des capillitiums mit Imiquimod oder Diclofenac. Aktuelle Dermatologie. 2015;41(01/02):50–53. doi:10.1055/s-0034-1390877
7. Chung BY, Um JY, Kim JC, Kang SY, Park CW, Kim HO. Pathophysiology and treatment of pruritus in elderly. Int J Mol Sci. 2020;22(1):174. doi:10.3390/ijms22010174
8. LaCour M, Allen T, Wilkerson M, Nguyen AV, Gibson BR. A case of erosive pustular dermatosis of the scalp in a pediatric patient. JAAD Case Rep. 2019;5(2):118–120. doi:10.1016/j.jdcr.2018.11.001
9. Wilk M, Zelger BG, Hauser U, Höpfl R, Zelger B. Erosive pustular dermatosis of the scalp: reappraisal of an underrecognized entity. J Dtsch Dermatol Ges. 2018;16(1):15–19. doi:10.1111/ddg.13387
1o. Broussard KC, Berger TG, Rosenblum M, Murase JE. Erosive pustular dermatosis of the scalp: a review with a focus on dapsone therapy. J Am Acad Dermatol. 2012;66(4):680–686. doi:10.1016/j.jaad.2011.10.011
11. Patton D, Lynch PJ, Fung MA, Fazel N. Chronic atrophic erosive dermatosis of the scalp and extremities: a recharacterization of erosive pustular dermatosis. J Am Acad Dermatol. 2007;57(3):421–427. doi:10.1016/j.jaad.2007.04.026
12. Langton AK, Herrick SE, Headon DJ. An extended epidermal response heals cutaneous wounds in the absence of a hair follicle stem cell contribution. J Invest Dermatol. 2008;128(5):1311–1318. doi:10.1038/sj.jid.5701178
13. Tomasini C, Michelerio A. Erosive pustular dermatosis of the scalp: a neutrophilic folliculitis within the spectrum of neutrophilic dermatoses: a clinicopathologic study of 30 cases. J Am Acad Dermatol. 2019;81(2):527–533. doi:10.1016/j.jaad.2018.10.029
14. Starace M, Loi C, Bruni F, et al. Erosive pustular dermatosis of the scalp: clinical, trichoscopic, and histopathologic features of 20 cases. Am Acad Dermatol. 2017;76(6):1109–1114.e2. doi:10.1016/j.jaad.2016.12.016







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}