



Innovative Treatment Utilizing an Autologous Blood Clot for Diabetic Foot Ulcers
Abstract
Introduction. Diabetic foot ulcer is a complex wound that requires considerable effort to restart a stalled healing process. In this study, a TABCT product was used in a point-of-care setting to treat DFUs by reconstructing the ECM and adjusting intricate phenotypes and mechanisms of mediators to progress towards complete healing. The mechanism of action consists of reconstruction of the ECM, which protects the wound area from further destruction while it incorporates into the ulcer to promote granulation over exposed vital structures (ie, tendons, bone, and neurovascular structures). Objective. The authors evaluated the efficacy of the TABCT product in the management of DFUs. Materials and Methods. Study participants were wound care patients in hospitals and clinics across the United States and Israel as part of a registry study (ClinicalTrials.gov: NCT04699305). Twenty-nine patients age 18 years or older with chronic DFUs were included. A blood clot was created using the patient’s own peripheral blood in a point-of-care setting. An 18-mL blood sample was drawn from the patient and incorporated with calcium gluconate and kaolin to form a clot. Efficacy and superiority levels in PAR at week 4 and week 12 over the SOC treatment were established using the Agresti-Coull confidence interval. Results. Treatment of DFUs using the TABCT product resulted in 22 patients (75.86%) achieving 50% PAR at week 4 and showed superiority when compared with SOC data in previously published studies. Complete closure was achieved in 28 wounds (95%) at week 12. Conclusion. In the current study, TABCT exhibited superiority over SOC treatment and provided granulation over vital structures with a reduction in overall wound size in a timely manner via incorporation and stimulation of the body’s own healing capabilities.
Abbreviations
CI, confidence interval; DFU, diabetic foot ulcer; ECM, extracellular matrix; NPWT, negative pressure wound therapy; PAR, percent area reduction; PDGF, platelet-derived growth factor; SOC, standard of care; TABCT, topical autologous blood clot therapy.
Introduction
Diabetic foot ulcer is among the most common complications of uncontrolled diabetes and is associated with an increased risk of mortality.1 The annual incidence of DFUs worldwide ranges between 9.1 million and 26.1 million.1 It is estimated that approximately 15% to 25% of patients with diabetes will develop a DFU in their lifetime, resulting in increased incidence of hospitalizations and amputations.1,2 In the United States, the total annual medical cost for the management of DFUs ranges between $9 billion and $13 billion.3
Diabetes alters the wound environment and negatively affects the ECM. Hyperglycemia causes an increase in advanced glycation end products, resulting in decreased ECM elasticity, which causes disruption of ECM-cell interactions and signaling.4,5 Irregularity of the ECM occurs as a result of decreased collagen and elastin production; decreased levels of thrombospondin-1, angiopoietin-like 4, hyaluronan, and glycosaminoglycans; and increased levels of tissue fibronectin, thrombospondin-2, osteopontin, connective tissue growth factor, versican expression, and tenascin-C.4 The alternating levels of these molecules are responsible for the irregular composition of the ECM and structure, which leads to further interruptions in ECM-cell interactions and compromised cell functions that prohibit proper cell migration, proliferation, and contraction. These adverse events induce a prolonged inflammatory phase, stalled healing process, and compromised neurovascular function, resulting in a chronic DFU.6
Effects of chronicity on ulcers
In the setting of chronic DFU, cellular events become dysfunctional, and crucial mediators are unable to activate and provide signaling for wound remodeling. Continued disruption of the ECM reduces signaling, adhesion, and activation of macrophages, growth factors, and various mediators, resulting in wound stagnation. Macrophages are essential not only in fostering a wound environment free of debris and bioburden, but in the initiation and progression of the healing cascade towards reepithelialization. Macrophages are involved in host defense, initiation and resolution of inflammation, growth factor production, phagocytosis, cellular proliferation, and tissue restoration in wounds.7
Under normal circumstances, owing to inflammation at the ulcerative site, macrophages are recruited to the area, where they engage in the polarization of various phenotypes that are mediated by cytokines, oxidants, lipids, and growth factors released by the same macrophages.7 Once recruited, macrophages ingest neutrophils, thus initiating their phenotypic conversion into anti-inflammatory macrophages via mediators released by neutrophils. The conversion of macrophages from pro-inflammatory (M1 classically activated) to anti-inflammatory (M2 alternatively activated) is a major differentiating factor between an ulcer that heals vs one that becomes chronic. The M1 macrophages release interleukin 12 and promote strong proinflammatory Th1 immune responses early in the healing process with the main intention of host defense. The M2 macrophages release interleukin 10 to downregulate inflammation and promote repair of soft tissue.7 Under chronic conditions, macrophages secreting interleukin 1 beta with an inflammatory phenotype are present in diabetic ulcers, which is part of a proinflammatory feedback loop that blocks the activation of M2 macrophages, preventing advancement towards tissue repair. Targeting the pathway of phenotypic modulations of macrophages is beneficial in generating new therapies. Development of a TABCT product (ActiGraft; RedDress Medical) assists in producing an environment in which phenotypic conversion from M1 to M2 macrophages can occur while repairing soft tissue deficits.
Treatment modality of TABCT
Chronic DFU is often managed using SOC options such as initial offloading, debridement of necrotic and infected soft tissue, antibiotics, and wound care dressings. Wound care dressings must provide a moist wound environment in which proper wound healing may occur. Further developments have been made towards creating autologous therapeutic modalities that can provide a moist and bioburden-free wound environment, reconstruction of the ECM to provide an organized means of signaling and activating mediators that are capable of restoring the wound healing mechanisms, and regeneration and epithelialization of soft tissue. This study evaluates the efficacy of a TABCT product to treat hard-to-heal DFUs in a real-world setting.
The TABCT product can be used in either an outpatient or inpatient setting for safe and rapid preparation and administration of a whole blood clot matrix. The blood clot is derived from the patient’s own peripheral blood and biologically delivers necessary growth factors and induces macrophages, cytokines, and mediators to promote the body’s natural healing process for treatment of the wound. Each application of the blood clot provides a protective covering, allowing the formation of a scaffold and integration into the ulcer to devise an optimal environment for healing. The newly formed scaffold acts as a biocompatible wound/environment barrier to prevent further contamination of the wound while preventing interruption of advancement through the wound healing process.16 While providing protection, the fibrin clot allows for remodeling and reconstruction of the ECM in an organized manner to assist with proper cell adhesion and signaling for recruitment of necessary factors and mediators to promote healing.
Materials and Methods
Patients
Study participants included wound care patients in hospitals and clinics across the United States and Israel as part of a registry study (ClinicalTrials.gov: NCT04699305). The inclusion criteria consisted of patients being age 18 years or older and with an eligible wound type (diabetic chronic wounds, hard-to-heal wounds, and those with delayed healing). Patients or their legally authorized representatives provided written informed consent before the patient was enrolled in the study.
Application and procedure for TABCT
Blood (18 mL) was withdrawn from the patient into acid citrate dextrose adenine vacuum tubes. The blood was then gently mixed with a calcium coagulant and kaolin in a coagulation mold to create a blood clot, which takes approximately 8 minutes. Reapplication was performed weekly.
Statistical analysis
Demographic and patient history data were described with the mean and standard deviation for normally distributed continuous data and the median and IQR for nonnormally distributed continuous data. Categorical data were described using frequencies and graphs. Assumptions of normality were evaluated using box plots, histograms, and a Shapiro-Wilks normality test.
Effectiveness
To quantify the extent to which the autologous blood clot is associated with wound healing, a Wilcoxon signed-rank test was conducted, and an effect size (r) was calculated. Assumptions of independence and symmetric distribution of differences were confirmed. To establish the 95% CI of the autologous fibrin clot effects, an Agresti-Coull confidence interval was constructed. Wound healing was operationalized as a 50% reduction in total wound area (PAR) by 4 weeks of treatment. Achievement of 50% PAR at 4 weeks is a strong predictor of 12-week wound healing, as identified by others.8,9 Wounds that have not attained 50% PAR by 4 weeks are not expected to heal by 12 weeks; this early marker serves as a reliable end point for research purposes.
Superiority
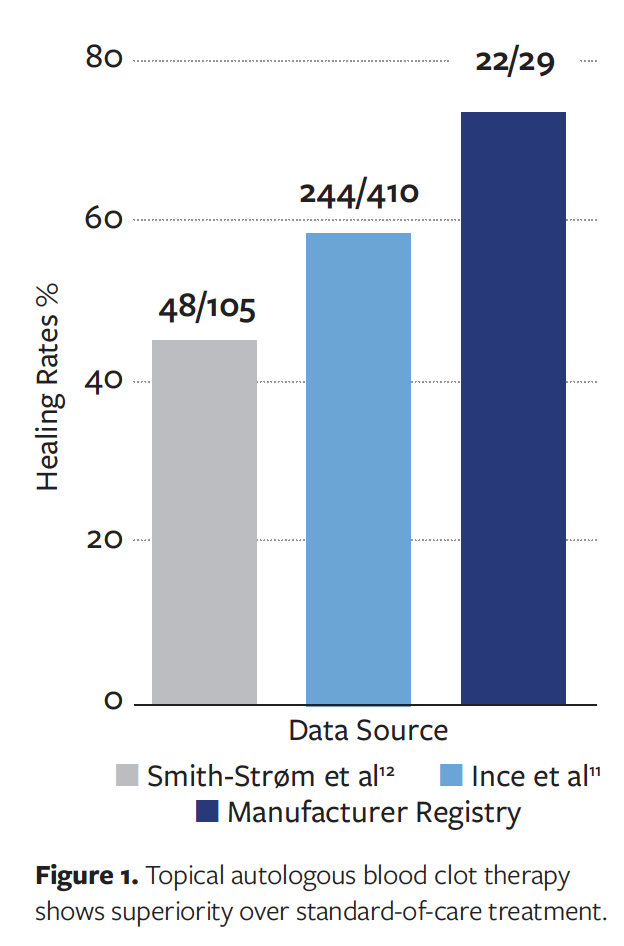
To determine whether the TABCT product was superior to the existing SOC, the success rates were compared with known values of healing identified in epidemiological studies using a 1-sided binomial probability test. The SOC is based on the following 4 principles: pressure relief, debridement, infection management via antibiotics and wound care dressings (ie, foam, collagen, alginate, and hydrogel), and, when indicated, revascularization.10 The TABCT product was compared with success rates identified in 2 observational studies.11,12 Comparison success rates were extracted from several manuscripts in the scientific literature. In an evaluation of 410 DFUs (of which, over 90% measured < 3 cm2 in size and had a median ulcer duration of 15 days), Ince et al11 identified a complete healing rate at 12 weeks of 59.3%. This study provides a benchmark rate of healing based on existing SOC. These researchers also identified significant (P =.047) associations between the duration of the ulcer at treatment initiation and the total time required for healing, as well as between ulcer size at referral and whether healing can be attained. Patients in the current study had chronic nonhealing DFUs, which take longer to heal and are less likely to achieve healing. In an observational study of 105 patients treated at 2 outpatient centers in Norway, Smith-Strøm et al12 identified a 45.7% overall healing rate. In their study, patients with ulcers that had persisted for 52 days or more before the patients were referred to a specialist experienced a 58% reduction in healing rates compared with patients who were referred earlier;verity at the start of treatment was found to be inversely associated with healing rates. Assumptions required for the binomial probability test were evaluated and confirmed, and success was operationally defined as achieving a PAR of 50% or more at the 4-week visit. Collectively, healing rates in epidemiological studies and clinical trials range from 45.7% to 59.3% using a SOC approach.11,12
Results
Sample characteristics and efficacy
of TABCT in achieving wound healing
A total of 39 patients were evaluated, and 29 had sufficient data for inclusion. There were 20 male (68.96%) and 7 female (24.14%) patients; sex was unknown for 2 patients. All patients had multiple comorbidities (type 2 diabetes, neuropathy, hypertension, hyperlipidemia, and peripheral arterial disease). Mean wound size at baseline was 9.36 cm2 ± 12.02 (range, 0.5–38.5 cm2). By week 4, the mean PAR was 75.48% ± 27.99 (range, 22%–100%). Per the Wilcoxon signed-rank test, the difference between this PAR and the 50% benchmark was statistically significant (z = 4.72; P <.001; r = 0.88). The Agresti-Coull CI for this effect ranges from 0.5762 to 0.8805 (range, 57.62%–88.05%). By week 4, there was a total of 9 patients (31.03%) who achieved complete healing and 22 patients (75.86%) who experienced 50% PAR. These results indicate that the use of TABCT is substantially associated with complete wound healing, per a PAR of at least 50% at 4 weeks. At week 12, a total of 28 wounds (95%) achieved complete wound closure.
Superiority of TABCT vs SOC
treatment
The TABCT product was compared with SOC for achieving 50% PAR at 4 weeks. A total of 22 patients (75.86%) were treated with the TABCT product and achieved 50% PAR at week 4. Comparison of this finding with the overall healing rate of 45.7% reported by Smith-Strøm et al12 showed the hematologic product to be superior to SOC treatment (P =.001). This was also the case when the finding in this study was compared with the higher rate of healing identified in the Ince et al11 benchmark findings of 59.3% (P =.046). In both comparisons, the fibrin blood clot was identified as the statistically significant superior treatment, because it achieved a greater proportion of at least 50% PAR at 4 weeks than the current SOC models identified in the current study (Figure 1). Additionally, patients evaluated in the observational studies experienced smaller wounds and wounds of shorter duration. Because the current study population is derived from a registry study, it represents patients with larger, harder-to-heal wounds, ie, patients identified in epidemiological studies as being the least likely to achieve healing.
Case 1
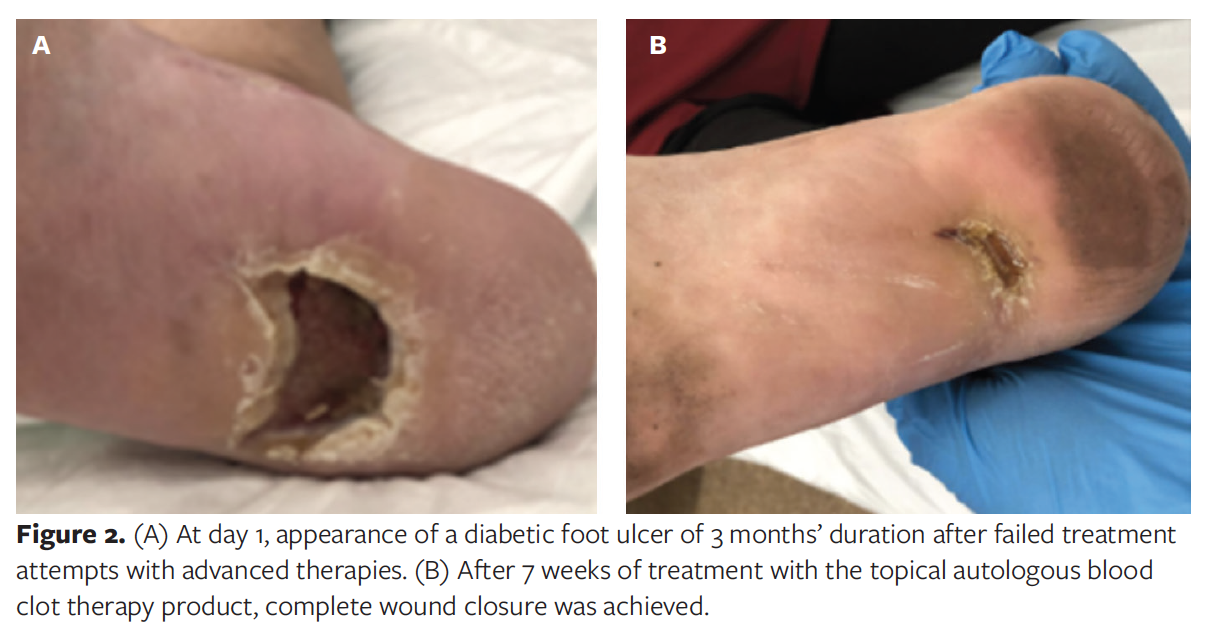
A 50-year-old female with type 2 diabetes presented with a large DFU of the right heel. Over the course of 3 months, the DFU was treated with excisional surgical debridement of nonviable soft tissue, NPWT set at −125 mm Hg, advanced wound care dressings, and a nonadherent antimicrobial hydroalginate dressing in an attempt to achieve wound healing. However, no reduction in ulcer size occurred. Because of a previous abscess and repeat infection at the ulcer site, the patient received antibiotics to control the infection. Following failure of all previous treatments, the TABCT product was applied. The fibrin blood clot was applied once weekly for 7 weeks, and it demonstrated a consistent decrease in ulcer size and depth. Complete healing was achieved at week 7, with complete epithelialization of the ulcer area with no signs of infection (Figure 2).
Case 2
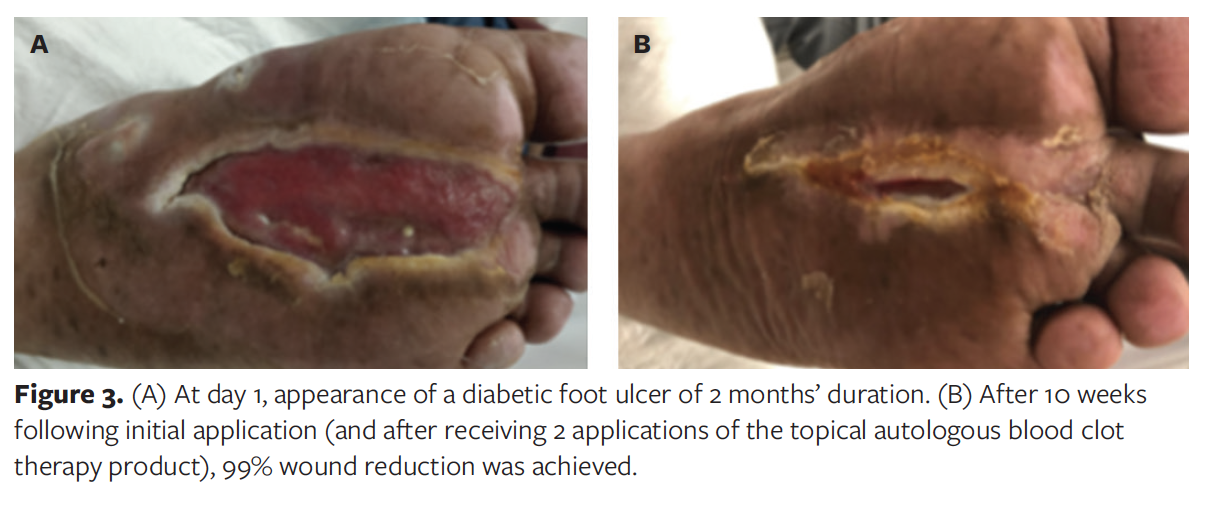
A 60-year-old male with type 2 diabetes presented with a plantar DFU of the left foot as well as chronic osteomyelitis of the first ray of the affected foot. The patient was treated with intravenous antibiotics for approximately 6 weeks. For 2 months, the ulcer was managed with conservative treatment consisting of NPWT at −125 mm Hg and advanced wound care dressings, without improvement. The TABCT product was applied once weekly in a point-of-care setting for 2 consecutive weeks. The patient returned to the clinic 10 weeks after the first application; by which time, the ulcer had reduced in size by 99% (Figure 3).
Case 3
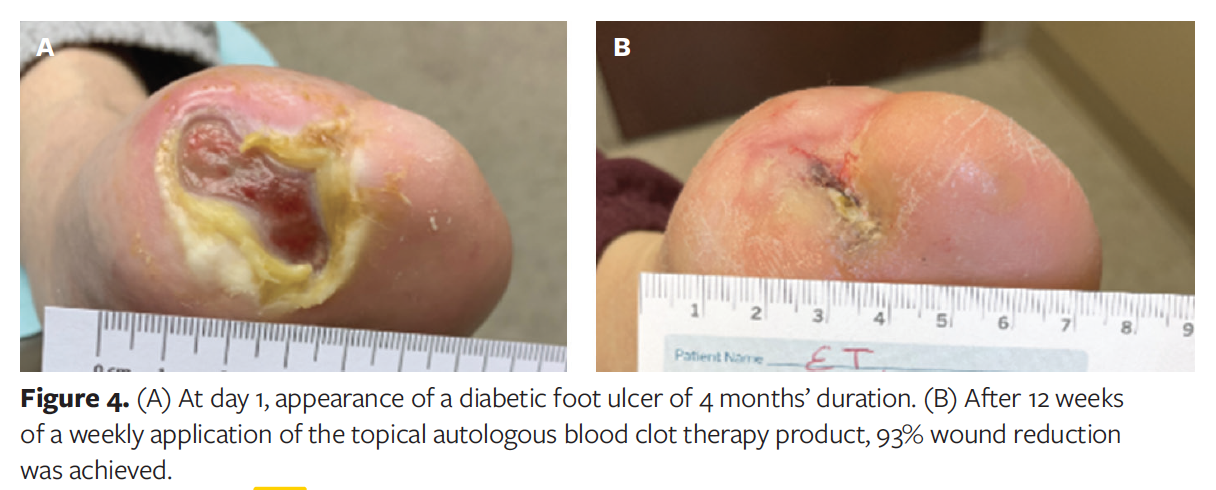
A 62-year-old female with a past medical history of type 2 diabetes, peripheral neuropathy, and a previous transmetatarsal amputation presented with a Wagner grade 3 DFU of the right foot. The ulcer showed no change after 4 months of repeat surgical debridement and use of amnion products. The TABCT product was applied once weekly for 12 weeks. One week after the first application, a decrease in ulcer drainage was observed. A decrease in ulcer size was noted weekly thereafter, along with a minimal amount of drainage present at the ulcer site. By week 12, the ulcer had reduced in size by 93% (Figure 4).
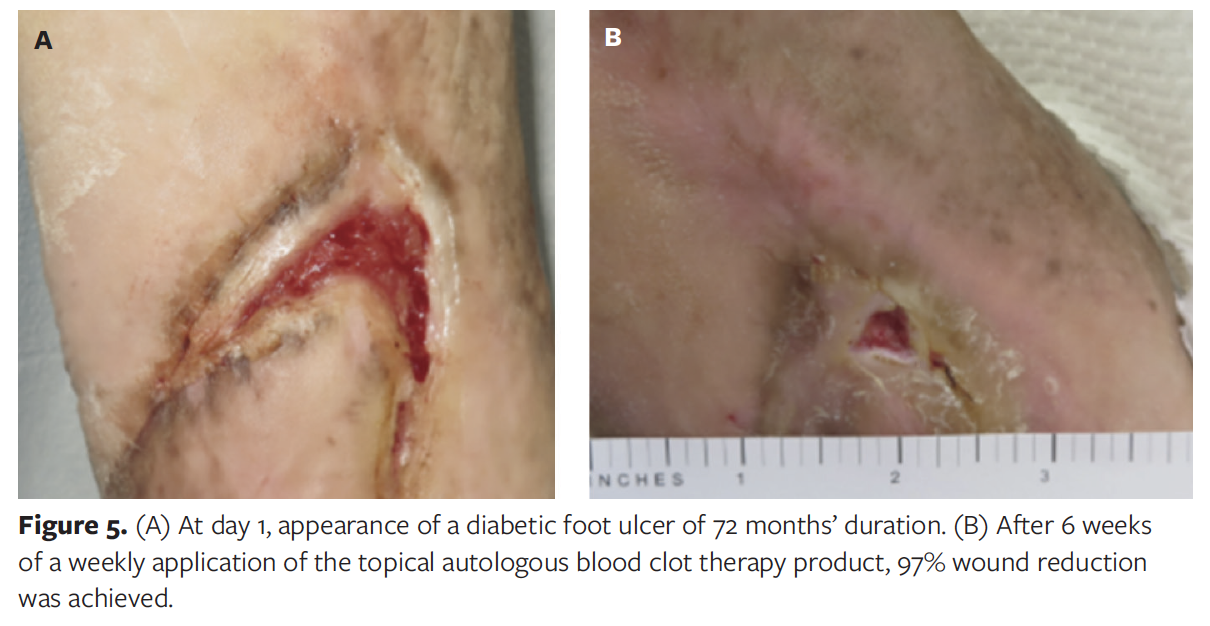
Case 4
A 58-year-old female with type 2 diabetes and peripheral neuropathy presented with a Wagner grade 1 plantar DFU of the right foot of 72 months’ duration. Despite previous management of the ulcer using saline, honey, cadexomer iodine, alginate, topical antibiotics, surgical debridement, and xeroform, no improvement occurred. The TABCT product was applied once weekly for 6 weeks, and the first and second applications resulted in 40% and 70% ulcer reduction, respectively. By week 6, the ulcer had reduced in size by 97% (Figure 5).
Case 5
A 58-year-old male with type 2 diabetes presented with a DFU of the right lateral ankle of 3 months’ duration. Previous management of the ulcer was not successful and included surgical drainage, NPWT set at −125 mm Hg, and a synthetic acellular dermal regeneration template. The ulcer size on day 1 of TABCT application was 29.4 cm2. The TABCT product was applied once weekly for 12 weeks, and a linear decrease in wound size occurred during the treatment period. By week 12, the ulcer had reduced in size by 98% (measuring 0.5 cm2) (Figure 6).

Discussion
The growing incidence of diabetes worldwide contributes to the increasing prevalence of DFUs, which constitute a huge burden on the health care system.13 Ulcer deterioration and limb amputation significantly reduce patients’ quality of life and increase morbidity and mortality.14 Achieving wound closure and wound reduction in the treatment of DFUs poses great challenges. The complexity of these ulcers is strongly correlated with stalling in the inflammatory phase of the wound healing process. Using a treatment option that facilitates progression of the wound from a stagnant stage in the inflammatory phase into the proliferative and remodeling phases remains the main goal of wound healing. In the management of DFUs, time is a variable that can drastically change the status of the ulcer. The longer the ulcer is stagnant without any improvement, the worse the outcomes, often resulting in tissue necrosis and even limb loss. Approximately 15% to 25% of patients with diabetes develop a foot ulcer, and of these, an estimated 12% require lower extremity amputation.15 To preserve the limb, it is necessary to effectively initiate the wound healing process while creating an environment that promotes reepithelialization.
Once applied, the TABCT product stimulates and activates the migration of growth factors to the injured area to assist in facilitating and expediting progression of the wound from the inflammatory phase to the proliferative phase. Using the patient’s autologous cells in the management of the wound or ulcer allows for stimulation and activation of the components that are present in the blood and platelet concentrate containing various types of cytokines and growth factors.16 The fibrin blood clot creates a scaffold that simulates a biologic delivery system that functions to control the release of growth factors and cytokines over several days.17 This scaffold allows for infiltration of cells and mediators such as neutrophils and monocytes, which initiate the differentiation of the monocytes into M1 macrophages. The clot acts as a protective scaffold, assisting in the reconstruction of the ECM as a means of providing an organized manner of healing that mimics the natural wound healing process. By re-creating the ECM, phenotypic modulation of macrophages occurs, stimulating anti-inflammatory M2 macrophages to promote cell attachment and spreading associated with the later phases of wound healing.18
The ECM is an important modulator of wound repair because of its effect on cell behavior, such as adhesion, migration, proliferation, or survival. The ECM also has an indirect effect by altering secretion, activation, and activity of extracellular protease, or by modulating growth factor activity or bioavailability.19 With proper remodeling of the ECM, granulation of the wound bed and coalescence of wound edges occur, which signify progression through the wound healing process.
The TABCT product contains and attracts different growth factors such as PDGF, fibroblast growth factor, epidermal growth factor, vascular endothelial growth factor, insulin-like growth factor, and transforming growth factor. These are necessary healing factors to the wound site that enhance and accelerate the wound healing process from the inflammatory phase to the proliferative phase. This process aids in the proliferation and migration of different cell types, endothelial cell stimulation, angiogenesis, and chemotaxis of fibroblasts and inflammatory cells; it aids in the continued production and/or remodeling of the ECM. These growth factors are imperative in formulating granulation tissue over exposed vital structures while providing angiogenesis, transferring nutrients and oxygen to the wound bed to promote tissue regeneration.20
During wound healing, monocytes adhere to the ECM to differentiate into M2 macrophages. Their attachment and differentiation lead to the upregulation of PDGF secretion, which plays a role in the proliferative phase of the wound healing process. Growth factors have the capability to regulate the ECM during wound healing by stimulating cells to increase the production of ECM components to create a stronger scaffold for adhesion and regulation of chemokines and mediators.21,22 The ECM, growth factors, and newly attracted chemokines and mediators continue to work together to provide granulation over the exposed vital structures to achieve wound closure.
The TABCT product was applied to DFUs of a mean size of 9.36 cm2 at baseline and was found to achieve complete wound closure and 50% PAR at 4 weeks in 31% and 76% of patients, respectively, in chronic and complex hard-to-heal DFUs. Complete ulcer reduction was noted in 95% of DFUs, which indicated the TABCT product was effective in the management of hard-to-heal DFUs. Based on the estimated success rates with SOC reported by Ince et al11 and Smith-Strøm et al12 (ie, successful treatment defined as achieving a PAR of 50% or more at week 4), treatment with the TABCT product exhibited superiority compared with the SOC approach. The fibrin clot creates a protective scaffold, contributing to the reconstruction of the ECM and allowing for the enhancement of adequate wound healing and remodeling of the skin deficit.
Limitations
This study identifies and quantifies the sizable effects of treatment with the TABCT product using real-world effectiveness data. However, the registry only included patients treated with the TABCT product; comparison group data were not available. One benefit of a registry study is that it includes patients who are not typically included in clinical trials. These patients often have larger wounds, hard-to-treat wounds, or wounds with a long history. Thus, registry studies are likely to produce estimates of effectiveness that are lower than estimates of efficacy identified in controlled trials. A comparison of treatments with TABCT in patients with large, poorly healing wounds would likely produce a larger effect size.
Conclusions
The TABCT product creates an environment that enhances the healing of complex and chronic wounds in an efficient and timely manner. With consistent application of the TABCT product to the injured area, reconstruction of the ECM occurs, thus modulating the current state of the wound with assistance from mediators such as macrophages. This in turn aids in the organized recruitment of growth factors, mediators, and cytokines necessary to promote wound healing and granulation over any exposed vital structures.
How Do I Cite This?
Williams M, Davidson D, Wahab N, Hawkins J, Wachuku CD, Snyder R. Innovative treatment utilizing an autologous blood clot for diabetic foot ulcers. Wounds. 2022;34(7):195–200. doi:10.25270/wnds/21089
Acknowledgments
Authors: Marie Williams, DPM1; David Davidson, DPM2; Naz Wahab, MD3; Jessie Hawkins, PhD4; Chinenye D. Wachuku, DPM5; and Robert Snyder, DPM6
Affiliations: 1Aventura Hospital and Medical Center, Aventura, FL; 2Buffalo General Medical Center, Williamsville, NY; 3Wound Care Experts, Las Vegas, NV; 4Franklin Health Research Center, Franklin, TN; 5Hoboken University Medical Center, Hoboken, NJ; 6Barry University School of Podiatric Medicine, Miami, FL
Disclosure: Dr. Snyder serves as a consultant for RedDress Medical.
ORCID: Jessie Hawkins, 0000-0002-0302-7327; Chinenye D. Wachuku, 0000-0002-8087-655X
Correspondence: Robert Snyder, DPM, 16800 NW 2nd Avenue Suite 202, North Miami Beach, FL 33169; drwound@aol.com
References
1. Oliver TI, Mutluoglu M. Diabetic foot ulcer. In: StatPearls [Internet]. StatPearls Publishing; 2022.
2. Volmer-Thole M, Lobmann R. Neuropathy and diabetic foot syndrome. Int J Mol Sci. 2016;17(6):917. doi:10.3390/ijms17060917
3. Barshes NR, Saedi S, Wrobel J, Kougias P, Kundakcioglu OE, Armstrong DG. A model to estimate cost-savings in diabetic foot ulcer prevention efforts. J Diabetes Complications. 2017;31(4):700-707. doi:10.1016/j.jdiacomp.2016.12.017
4. Huang Y, Kyriakides TR. The role of extracellular matrix in the pathophysiology of diabetic wounds. Matrix Biol Plus. 2020;6-7:100037. doi:10.1016/j.mbplus.2020.100037
5. Qing C. The molecular biology in wound healing & non-healing wound. Chin J Traumatol. 2017;20(4):189-193. doi:10.1016/j.cjtee.2017.06.001
6. Davis FM, Kimball A, Boniakowski A, Gallagher K. Dysfunctional wound healing in diabetic foot ulcers: new crossroads. Curr Diab Rep. 2018;18(1). doi:10.1007/s11892-018-0970-z
7. Snyder RJ, Lantis J, Kirsner RS, Shah V, Molyneaux M, Carter MJ. Macrophages: a review of their role in wound healing and their therapeutic use. Wound Repair Regen. 2016;24(4):613-629. doi:10.1111/wrr.12444
8. Snyder RJ, Cardinal M, Dauphinée DM, Stavosky J. A post-hoc analysis of reduction in diabetic foot ulcer size at 4 weeks as a predictor of healing by 12 weeks. Ostomy Wound Manage. 2010;56(3):44-50.
9. Del Core MA, Ahn J, Lewis RB III, Raspovic KM, Lalli TA, Wukich DK. The evaluation and treatment of diabetic foot ulcers and diabetic foot infections. Foot Ankle Orthopaedics. 2018;3(3). doi:10.1177/2473011418788864
10. Aldana PC, Khachemoune A. Diabetic foot ulcers: appraising standard of care and reviewing new trends in management. Am J Clin Dermatol. 2020;21(2):255–264. doi:10.1007/s40257-019-00495-x
11. Ince P, Game FL, Jeffcoate WJ. Rate of healing of neuropathic ulcers of the foot in diabetes and its relationship to ulcer duration and ulcer area. Diabetes Care. 2007;30(3):660-663. doi:10.2337/dc06-2043
12. Smith-Strøm H, Iversen MM, Igland J, et al. Severity and duration of diabetic foot ulcer (DFU) before seeking care as predictors of healing time: a retrospective cohort study. PLoS One. 2017;12(5):e0177176. doi:10.1371/journal.pone.0177176
13. International Diabetes Federation. The global burden. IDF Diabetes Atlas. 5th ed. 2012:38-39.
14. Noor S, Zubair M, Ahmad J. Diabetic foot ulcer--a review on pathophysiology, classification and microbial etiology. Diabetes Metab Syndr. 2015;9(3):192-199. doi:10.1016/j.dsx.2015.04.007
15. Greer N, Foman N, Dorrian J, et al. Advanced wound care therapies for non-healing diabetic, venous, and arterial ulcers: a systematic review [Internet]. Evidence-based Synthesis Program. Department of Veterans Affairs (US); 2012.
16. Snyder RJ, Schultz G, Wachuku C, Rashid AM, Ead JKK. Proposed mechanism of action of topically applied autologous blood clot tissue: a quintessential cellular and tissue based therapy. J Am Podiatr Med Assoc. 2020;20–140. doi:10.7547/20-140
17. Maquart FX, Monboisse JC. Extracellular matrix and wound healing. Pathol Biol (Paris). 2014;62(2):91–95. doi:10.1016/j.patbio.2014.02.007
18. Krzyszczyk P, Schloss R, Palmer A, Berthiaume F. The role of macrophages in acute and chronic wound healing and interventions to promote pro-wound healing phenotypes. Front Physiol. 2018;9:419. doi:10.3389/fphys.2018.00419
19. Chen Z, Fu S, Wu Z, et al. Relationship between plasma angiogenic growth factors and diabetic foot ulcers. Clin Chim Acta. 2018;482:95–100. doi:10.1016/j.cca.2018.03.035
20. Schultz GS, Wysocki A. Interactions between extracellular matrix and growth factors in wound healing. Wound Repair Regen. 2009;17(2):153–162. doi:10.1111/j.1524-475X.2009.00466.x
21. Zubair M, Ahmad J. Role of growth factors and cytokines in diabetic foot ulcer healing: a detailed review. Rev Endocr Metab Disord. 2019;20(2):207–217. doi:10.1007/s11154-019-09492-1
22. Chang M. Restructuring of the extracellular matrix in diabetic wounds and healing: a perspective. Pharmacol Res. 2016;107:243-248. doi:10.1016/j.phrs.2016.03.008






