Pulsed Electromagnetic Field Stimulation Therapy for Charcot Foot Ulcer: A Randomized Controlled Trial
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Wounds or HMP Global, their employees, and affiliates.
Abstract
Background. Charcot foot is a debilitating complication of peripheral neuropathy and is primarily associated with diabetes, leading to structural damage, ulceration, and osteomyelitis. Pulsed electromagnetic field (PEMF) therapy is a promising treatment modality for wound healing and bone metabolism. Objective. To evaluate the efficacy of PEMF therapy in promoting bone growth and ulcer healing in patients with Charcot foot ulcers. Materials and Methods. This prospective, single-blinded, controlled trial included 34 patients with stage 2 or 3 chronic Charcot foot with ulceration who were randomized into 2 groups. Group A (study group) received PEMF therapy in addition to transcutaneous electrical nerve stimulation (conventional TENS), medical treatment, and standard wound care, while group B (control group) received conventional TENS and the same medical treatment and standard wound care as those in group A, 3 times per week for 3 months. Primary outcomes were assessed with plain radiographs and wound surface area tracing pre-intervention, 6 weeks post-intervention, and 12 weeks post-intervention. Results. No significant differences were evident at baseline analysis. After 6 weeks, both groups showed significant change in Charcot foot signs as well as a reduction in wound surface area (P < .05). In the study group, 23.5% of participants showed complete resolution of Charcot signs (normal appearance), 5.9% progressed to stage 2 (bone sclerosis), and 70.6% remained at stage 1. Regarding wound healing, the study group showed greater reduction in wound surface area, with a median (IQR) of 8.5 cm2 (9.4 cm2-12.2 cm2) compared with 11.5 cm2 (9.4 cm2-15.5 cm2) in the control group. By 12 weeks, 94.1% of the study group showed complete radiological resolution of Charcot signs vs 5.9% in the control group (P < .001). Median wound surface area was significantly reduced in the study group to 0.0 cm² (0.0 cm²-1.0 cm²) compared with 6.6 cm2 (5.7 cm²-7.9 cm²) in the control group (P < .05), indicating superior healing outcomes with PEMF therapy. Conclusion. PEMF therapy is an efficacious adjunctive treatment for Charcot foot ulcers, facilitating both wound healing and bone regeneration.
Introduction
Charcot foot, a debilitating complication of neuropathy, has an estimated prevalence of approximately 0.8% to 8% in the general diabetic population.1 It is primarily associated with diabetes mellitus, but it may also occur in patients with conditions such as neurosyphilis, syringomyelia, leprosy, and congenital neuropathies.1
The pathogenesis of Charcot foot involves repetitive microtrauma in a foot with impaired sensation, combined with neurovascular changes leading to increased bone resorption and joint destruction. The diagnosis is often delayed, resulting in severe complications, including fractures, dislocations, and in some cases, amputation. Early diagnosis and appropriate treatment are critical for preventing these complications.2
Charcot foot typically progresses through distinct stages of disease, including inflammation, fragmentation, coalescence, and consolidation. During the active inflammatory phase, the foot is characterized by redness, warmth, and swelling, often without pain due to the underlying neuropathy. As the disease progresses, bone and joint destruction leads to deformities, such as the classic rocker-bottom foot, which is associated with a high risk of ulceration and further complications.3
The management of Charcot foot often includes off-loading and immobilization to prevent further damage to the affected foot, but complications such as ulcers remain a significant challenge.4 Charcot foot ulcers, which may develop due to structural deformities and diminished protective sensation, are notoriously difficult to heal and often lead to infection, osteomyelitis, and amputation. Key clinical challenges include joint deformity, compromised local blood flow, increased risk of infection, and issues with patient adherence, each of which complicates management and outcomes.5 The role of physical therapy in managing Charcot foot ulcers is gaining attention, with various modalities—including high-power laser therapy, electrical stimulation, and pulsed electromagnetic field (PEMF) therapy—being explored as adjunctive treatments to enhance wound healing.
PEMF therapy has shown promise in promoting soft tissue repair and bone healing. It operates by emitting low-frequency, low-intensity electromagnetic fields that interact with local tissues, potentially accelerating cellular processes involved in wound healing and bone metabolism. Studies suggest that PEMF may influence cellular transduction pathways and enhance the healing of chronic, nonhealing wounds by re-stimulating the arrested wound healing process.6 PEMF has also been shown to regulate bone formation and metabolism by affecting the function of cells and extracellular matrix in bone tissue.7 This offers a potential therapeutic avenue for patients with Charcot foot, for which both soft tissue healing and bone integrity are crucial.7 However, to optimize outcomes, it is essential to consider the multifactorial nature of Charcot neuropathy (CN), in which deformity alters biomechanical loading and healing potential, impaired blood flow affects tissue viability and healing, infections can exacerbate joint destruction, and poor adherence, especially with off-loading regimens, can hinder recovery.8 Electrical stimulation could represent a new therapy for patients with diabetic peripheral neuropathy. Six studies confirmed that electrical stimulation provided improvement of sensory neuropathy and symptoms of painful neuropathy in persons with diabetes.9 Electrical stimulation has been found to offer relief from peripheral neuropathy pain by stimulating cutaneous afferent fibers.9
The aim of the current study was to evaluate the efficacy of PEMF therapy in promoting bone growth and ulcer healing in patients with Charcot foot ulcers.
Materials and Methods
This single-blinded, randomized, controlled trial enrolled 34 patients with stage 2 or 3 chronic Charcot foot with ulceration into the study. Participants, aged 50 to 70 years, were recruited from Kasr Al Ainy Hospital, Cairo University. All subjects were carefully screened to exclude any conditions that could interfere with the healing process, such as malignancy, autoimmune disorders, rheumatologic diseases, hypotension, and ischemic conditions.
Ethical consideration
The study received approval from the hospital’s Institutional Review Board (IRB) (IRB approval number P.T.REC/012/005154). Additionally, the trial was registered under the clinical registry number NCT06527131. After participants were adequately briefed on the study’s goals, their written informed consent was obtained. Subjects were free to withdraw from the study at any time; participation was entirely voluntary. In accordance with the Declaration of Helsinki, all steps of data collecting, entry, and analysis were conducted in a highly confidential and private manner.
The patients were randomized into 2 groups: study group A, which involved the study intervention, had 17 patients, and the control group B had 17 patients as well. The randomization process was conducted by a blinded, independent research assistant using a computer-generated randomization system. To maintain allocation concealment, the group assignments were placed in opaque, sealed envelopes that were sequentially numbered and opened only after patient consent and baseline assessments were completed.
All participants demonstrated full adherence to the PEMF treatment protocol. No patients missed more than 10% of the scheduled sessions. In fact, 100% of patients attended all their assigned appointments, and no dropouts were recorded during the intervention period. Therefore, the adherence rate for PEMF therapy was 100%.
Outcome measures
Patients were assessed before treatment, after 6 weeks of treatment, and after 12 weeks of treatment using diagnostic plain radiographic evaluation for radiological features of Charcot foot and bone regeneration, including the presence and severity of fractures, bone fragmentation, sclerosis, and other bone deformities commonly associated with Charcot osteoarthropathy. Additionally, wound surface area was measured using the tracing method, which involves placing a transparency film over a wound, tracing the wound perimeter, and then placing the tracing over graph paper to count the squares and determine the surface area. This is a more accurate and reliable method than standard multiplication of length by width to calculate wound surface area.10
The combination of radiological evaluation and wound surface area tracing provided a comprehensive assessment of both internal bone structure and external wound healing, ensuring a thorough evaluation of treatment efficacy across all study participants.
Interventions
After the participants were divided into 2 groups, study group A received PEMF therapy using the CryoMag Professional device (Level). Each patient was comfortably positioned in a supine posture, and the PEMF applicator was precisely adjusted to target the site of the Charcot foot ulcer. The therapy parameters were set to a frequency of 20 Hz, with an intensity of 50 gauss. Each session lasted for 120 minutes. In addition, ice was applied locally at a temperature of approximately 12°C, with a controlled pressure of 25 mm Hg to manage inflammation and provide adjunctive relief. Both groups received transcutaneous electrical nerve stimulation, as well as the same medical treatment and standard wound care, which included regular debridement, dressing changes, and off-loading. Additionally, infection control was conducted 3 times per week for a duration of 3 months for both groups. This comprehensive care ensured that all participants received appropriate wound management in conjunction with their assigned therapeutic intervention.
Statistical analysis
All statistical analyses were performed using open-source Jamovi software (version 2.3.28). An unpaired t test was used to compare age between the 2 groups, and a chi-square test was performed to compare sex distribution. The Shapiro-Wilk test was used to assess the normality of the data. For within-group comparisons of pre- and post-treatment outcomes, a paired t test was conducted. A P value less than .05 was set as the level of significance for all statistical tests.
Results
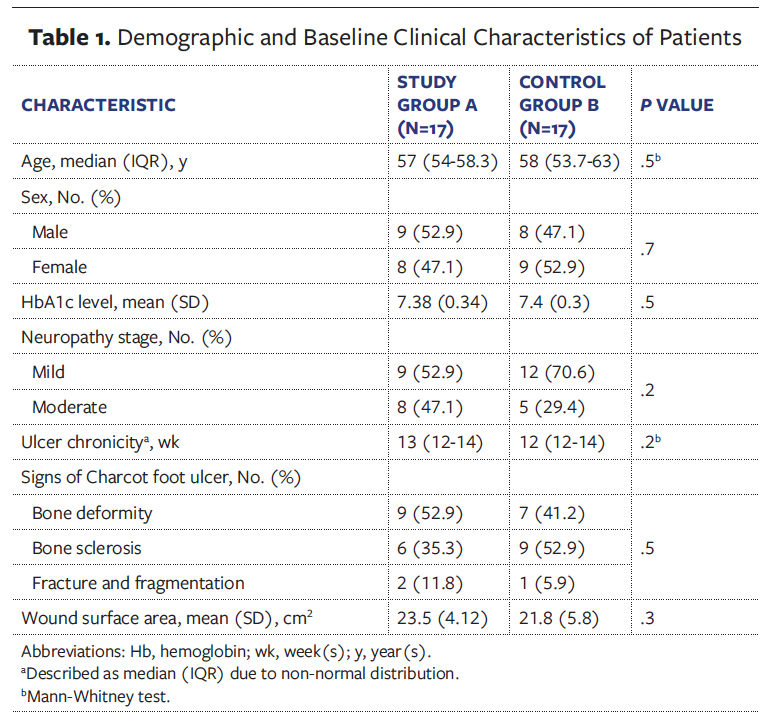
The study participants had a median age of 57 years. Males and females were represented equally. Before treatment, there was no statistically significant difference between the 2 groups concerning age, ulcer chronicity, and glycemic control, and the mean (standard deviation) wound surface area was 23.5 (4.12) cm² in the study group and 21.8 (5.8) cm² in the control group (Table 1). Sex distribution, neuropathy severity, and signs of Charcot foot ulcer were also comparable between the groups, with no statistically significant difference, confirming that both groups had comparable baseline metabolic control, which is important for wound healing.
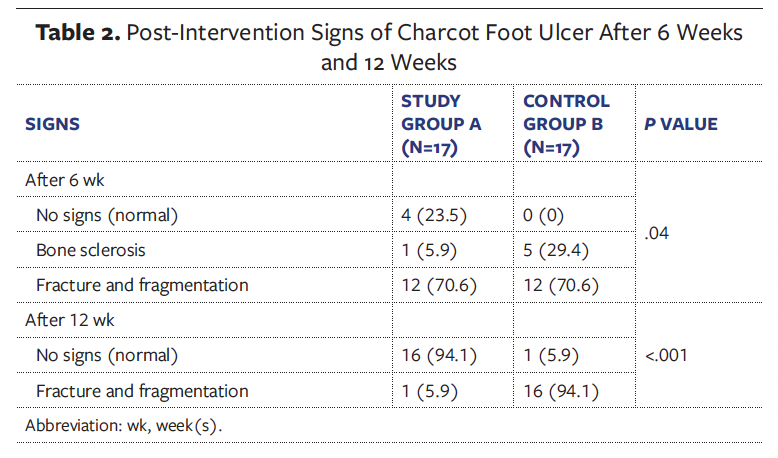
After 6 weeks of treatment, there was a statistically significant change in Charcot foot signs as well as a reduction in wound surface area in both groups (P < .05) (Table 2). At that time, 23.5% of participants in study group A (n = 4) showed no signs of Charcot foot (normal), 5.9% (n = 1) progressed to bone sclerosis (stage 2), and 70.6% (n = 12) showed fracture and fragmentation (stage 1). In comparison, no participants in control group B showed resolution of Charcot foot signs (0%), while 29.4% (n = 5) presented with bone sclerosis (stage 2), and 70.6% (n = 12) presented with fracture and fragmentation (stage 1).
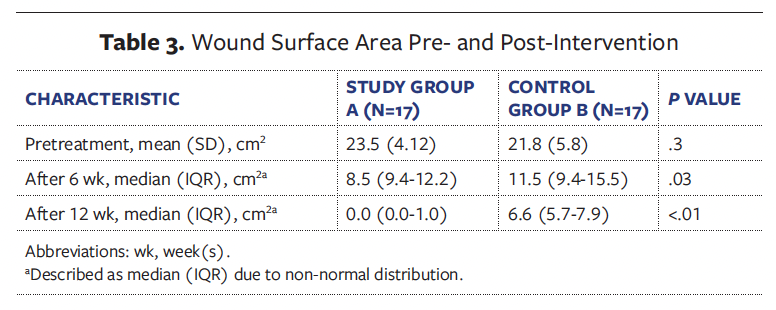
Regarding wound surface area, after 6 weeks the study group demonstrated greater improvement, with a median (IQR) of 8.5 cm2 (9.4 cm2-12.2 cm2) compared with 11.5 cm2 (9.4 cm2-15.5 cm2) in the control group (Table 3).
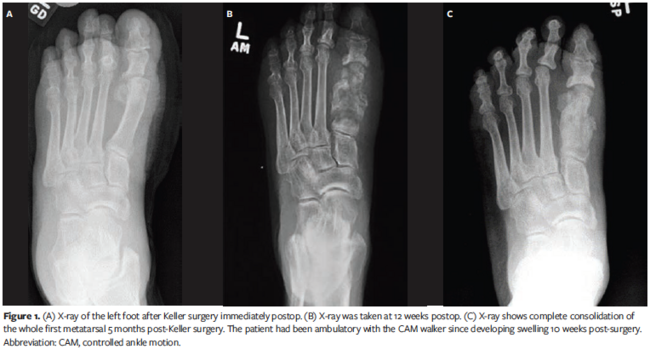
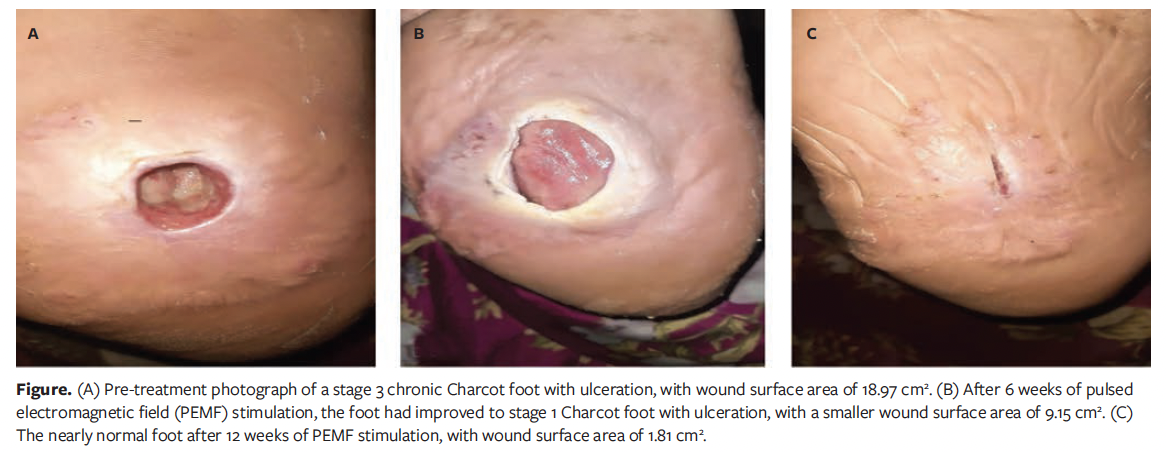
By 12 weeks, the treatment effect became even more pronounced, with 94.1% of study group A showing complete resolution of Charcot foot signs (normal) compared with 5.9% in the control group, a significant difference (P < .001) (Table 2). In addition, study group A showed a dramatic improvement in wound surface area, with a median (IQR) area of 0.0 cm² (0.0 cm²-1.0 cm²), indicating near-complete healing in most participants (Table 3) (Figure).
In contrast, the control group had a median wound surface area of 6.6 cm² (5.7 cm²-7.9 cm²). The P values less than .05 for 6- and 12-week results reflect significant difference between the groups, with study group A demonstrating superior wound healing outcomes compared with the control group.
Discussion
Charcot joint or neurogenic arthropathy in patients with diabetes leads to severe complications such as joint dislocation and deformity. Early diagnosis and appropriate management are important to prevent severe damage and amputation.2 Several classification systems are used to classify Charcot arthropathy.
The Eichenholtz classification for Charcot arthropathy divides Charcot foot into 3 stages according to clinical and radiographic criteria.11 Stage 1, or the fragmentation stage, involves bony destruction resulting in ligamentous laxity and subluxation, with radiographic evidence of bone destruction, debris formation, and/or dislocation. In stage 2 (coalescence), periarticular debris is absorbed and larger bone fragments form calluses, with radiographic evidence of absorption of debris and sclerosis formation. In stage 3, the reconstruction stage, there is radiographic evidence of consolidation and remodeling of fracture fragments.
The present study was conducted on 34 patients with stage 2 or 3 chronic Charcot foot with ulceration to evaluate the efficacy of PEMF therapy in promoting bone growth and ulcer healing. Through the induction of various cellular and physiological responses, PEMF stimulation primarily works by enhancing cellular metabolism, promoting angiogenesis, and modulating inflammatory responses.12 At the cellular level, PEMF stimulation increases the production of growth factors and cytokines, which are crucial for tissue repair and regeneration. It also stimulates the proliferation and differentiation of osteoblasts and chondrocytes, contributing to improved bone and cartilage healing.12 The application of PEMF therapy in CN shows promising effects on bone regeneration and modulation of inflammatory mediators. Nonetheless, the clinical context of CN requires a broader consideration of other influencing factors. Deformity, palpable loose bodies, and prominent osteophytes are consequences of substantial joint and bone destruction, followed by bony proliferations. The typical end-stage appearance of a Charcot foot is the rocker-bottom deformity.13 PEMF enhances the stimulation of osteoblast proliferation and differentiation for bone formation. It may aid in early-stage bone remodeling, but in advanced deformity, surgical correction may still be necessary. Thus, the role of PEMF should be evaluated within the stage of deformity progression.14
Regarding blood flow, vascular compromise in patients with diabetes (particularly those with peripheral arterial disease) limits oxygen and nutrient delivery to affected joints. The potential of PEMF to enhance microvascular perfusion could be beneficial; however, its efficacy may vary based on baseline vascular status, and further stratified studies are needed.15
As for infection, infection complicates CN management due to overlapping osteomyelitis and soft tissue involvement. While PEMF is not directly antimicrobial, it must be used with caution in infected sites, and appropriate infection control should be established before initiating therapy.16
Patient adherence is a determining factor for CN treatment. Effective management of CN depends heavily on patient adherence to off-loading, immobilization, and professional foot care. PEMF therapy requires consistent application over time, and its success is contingent on patient adherence.17
The current study demonstrated that PEMF therapy significantly improved both clinical signs and wound healing in patients with Charcot foot ulcers compared with the control group; both groups received transcutaneous electrical nerve stimulation and standard medical treatment. There were no significant differences between the groups in terms of baseline characteristics, including age, sex, hemoglobin A1c level, neuropathy stage, or ulcer chronicity, ensuring that the observed effects could be attributed to the intervention.
Six weeks after intervention, study group A showed a significant reduction in bone sclerosis and an increase in number of patients with no signs of Charcot foot compared with the control group (23.5% vs 0%; P = .04). Furthermore, the wound surface area in the study group was significantly smaller than in the control group (P = .03), suggesting that PEMF therapy accelerates wound healing. By 12 weeks, the differences became more pronounced, with 94.1% of the study group showing no signs of Charcot foot, compared with 5.9% of the control group showing no signs of Charcot foot (P < .001).
Additionally, after 12 weeks study group A achieved near-complete wound healing (median wound surface area, 0.0 cm²), while the control group still had significant residual wounds (median wound surface area, 6.6 cm²) (P < .01). The findings of the current study align with several previous investigations that have demonstrated the efficacy of PEMF therapy in treating Charcot foot and other chronic wounds.
These findings are in agreement with those of Ziegler et al,18 who studied elderly patients undergoing high tibial osteotomy and reported faster osseous consolidation with PEMF therapy, particularly in patients aged 50 years or older. These findings suggest that PEMF is a valuable adjunct therapy for bone healing, especially in populations with impaired healing capacity, such as the elderly or those with diabetes.18
Additionally, PEMFs have been shown to significantly reduce the time to bone consolidation in patients with Charcot arthropathy, with an average healing time of 11 weeks in the PEMF- treated group compared to 23.8 weeks in the control group.19 This finding is in agreement with a study published in 2017 that concluded that PEMF therapy significantly improved wound healing in patients with diabetic foot ulcers, which share numerous similarities with Charcot foot ulcers in terms of delayed healing due to neuropathy, poor circulation, and chronic inflammation.20 Building on these results, the findings of the current study reinforce the emergence of PEMF stimulation as a promising therapeutic approach for managing Charcot foot ulcers.
Limitations
The study results are limited to the selected sample with the parameters used. The relatively short follow-up duration also limited this study. Further studies should be conducted to gather more convincing evidence on the long-term effects of PEMF on Charcot foot ulcer.
Conclusion
Charcot foot is a debilitating complication of neuropathy. Delayed diagnosis can result in severe complications, including deformity and ulcers. This study supports the efficacy of PEMF as a non-invasive adjunct for managing Charcot neuropathy and associated foot ulceration. Over a 12-week period, the intervention group demonstrated significantly superior outcomes compared to the control group, achieving remarkable improvements in both structural bone integrity (with a majority returning to a normal classification) and accelerated wound healing (with near-complete ulcer closure).
Author & Publication Information
Authors: Norhan Mohamed Eltayeb, BS1; Marwa Mahdy Abdelhamid, PhD1; Hossam Zaghloul Yousuf, MD2; and Nessrein Afifi Abd-Elrashid, PhD1
Affiliations: 1Faculty of Physical Therapy, Cairo University, Cairo, Giza, Egypt; 2Vascular Surgery Department, Kasr Al Ainy Faculty of Medicine, Cairo University; Cairo, Egypt
Author Contributions: Study design: N.A. Acquisition of data: N.E. Analysis and interpretation of data: N.A., N.E., H.Y. Drafting of the manuscript: M.A., N.E., H.Y. Revision of the manuscript: N.A., M.A., H.Y. Read and approved the final manuscript: all authors.
Disclosure: The authors disclose no financial or other conflicts of interest.
Ethical Approval: The trial received approval from the Institutional Review Board (IRB approval number: P.T.REC/012/005154) and was registered under the clinical registry number NCT06527131. Written informed consent was obtained from all participants.
Correspondence: Norhan Mohamed Eltayeb, BS; Faculty of Physical Therapy, Cairo University, 7 Ahmed El Zayat Street, Bein El Sarayat, Dokki, Giza 12611, Egypt; 1400534@st.pt.cu.edu.eg
Manuscript Accepted: June 24, 2025
References
1. Gouveri E, Papanas N. Charcot osteoarthropathy in diabetes: a brief review with an emphasis on clinical practice. World J Diabetes. 2011;2(5):59-65. doi:10.4239/wjd.v2.i5.59)
2. Jeong JJ. Diagnosis and treatment of Charcot arthropathy in diabetic patients. Journal of Korean Medical Association. 2021;64(8):543-550. doi:10.5124/jkma.2021.64.8.543
3. Rosskopf AB, Loupatatzis C, Pfirrmann CWA, Böni T, Berli MC. The Charcot foot: a pictorial review. Insights Imaging. 2019;10(1):77. doi:10.1186/s13244-019-0768-9
4. Madan SS, Pai DR. Charcot neuroarthropathy of the foot and ankle. Orthop Surg. 2013;5(2):86-93. doi:10.1111/os.12032
5. Konarzewska A, Korzon-Burakowska A,
Rzepecka-Wejs L, Sudoł-Szopińska I, Szurowska E, Studniarek M. Diabetic foot syndrome: Charcot arthropathy or osteomyelitis? Part I: clinical picture and radiography. J Ultrason. 2018;18(72):42-49. doi:10.15557/JoU.2018.0007
6. Seeliger C, Falldorf K, Sachtleben J, van
Griensven M. Low-frequency pulsed electromagnetic fields significantly improve time of closure and proliferation of human tendon fibroblasts. Eur J Med Res. 2014;19(1):37. doi:10.1186/2047-783X-19-37
7. Yuan J, Xin F, Jiang W. Underlying signaling pathways and therapeutic applications of pulsed electromagnetic fields in bone repair. Cell Physiol Biochem. 2018;46(4):1581-1594. doi:10.1159/000489206
8. Stancu B, Ilyés T, Farcas M, Coman HF, Chiș BA, Andercou OA. Diabetic foot complications: a retrospective cohort study. Int J Environ Res Public Health. 2022;20(1):187. doi:10.3390/ijerph20010187
9. Thakral G, Kim PJ, LaFontaine J, Menzies R,
Najafi B, Lavery LA. Electrical stimulation
as an adjunctive treatment of painful and
sensory diabetic neuropathy. J Diabetes Sci
Technol. 2013;7(5):1202-1209. doi:10.1177/193229681300700510
10. Alonso MC, Mohammed HT, Fraser RD, Ramirez Garcia Luna JL, Mannion D. Comparison of wound surface area measurements obtained using clinically validated artificial intelligence-
based technology versus manual methods and the effect of measurement method on debridement code reimbursement cost. Wounds. 2023;35(10):E330-E338. doi:10.25270/wnds/23031
11. Rosenbaum AJ, DiPreta JA. Classifications in
brief: Eichenholtz classification of Charcot
arthropathy. Clin Orthop Relat Res. 2014;473(3):1168-1171. doi:10.1007/s11999-014-4059-y
12. Caliogna L, Bina V, Brancato AM, et al. The role of PEMFs on bone healing: an in vitro study. Int J Mol Sci. 2022;23(22):14298. doi:10.3390/ijms232214298
13. Ergen FB, Sanverdi SE, Oznur A. Charcot foot in diabetes and an update on imaging. Diabetic Foot Ankle. 2013:4. doi:10.3402/dfa.v4i0.21884
14. Galli C, Pedrazzi G, Guizzardi S. The cellular effects of pulsed electromagnetic fields on osteoblasts: a review. Bioelectromagnetics. 2019;40(4):211-233. doi:10.1002/bem.22187
15. Stewart GM, Wheatley-Guy CM, Johnson BD, Shen WK, Kim CH. Impact of pulsed electromagnetic field therapy on vascular function and blood pressure in hypertensive individuals. J Clin Hypertens (Greenwich). 2020;22(6):1083-1089. doi:10.1111/jch.13877
16. Hussain MSE, Anwar HW, Elnakib MM, Mosaad AE. Evaluation of the effect of pulsed electromagnetic field therapy in the treatment of chronic wounds. Microbes and Infectious Diseases. 2023;4(3):928-942. doi:10.21608/mid.2023.203163.1497
17. Jansen RB, Svendsen OL. A review of bone metabolism and developments in medical treatment of the diabetic Charcot foot. J Diabetes Complications. 2018;32(7):708-712. doi:10.1016/j.jdiacomp.2018.04.010
18. Ziegler P, Nussler AK, Wilbrand B, et al. Pulsed electromagnetic field therapy improves osseous consolidation after high tibial osteotomy in elderly patients-a randomized, placebo-controlled, double-blind trial. J Clin Med. 2019;8(11):2008. doi:10.3390/jcm8112008
19. Petrisor B, Lau JTC. Electrical bone stimulation: an overview and its use in high risk and Charcot foot and ankle reconstructions. Foot Ankle Clin. 2005;10(4):609-620. doi:10.1016/j.fcl.2005.06.003
20. Abd El Rasheed NA, Mahmoud NF, Hamada AH, Khatib AHE. Pulsed electromagnetic fields versus laser therapy on enhancing recovery of diabetic foot ulcer- a single blind randomized controlled trial. Biomedical Research. 2017;28(19):8509-8514.