



A Real-world Study of a Calcium Alginate Dressing for Various Wound Etiologies on Clinical Performance, Usability, and Safety
Abstract
Introduction. Complex wounds require a moist wound healing environment and exudate control. Alginate dressings are highly absorbable and available as sheets for superficial wounds and ropes for deeper wounds. Objective. This study evaluates the real-world performance of a conformable CAD containing mannuronic acid for various wound types. Materials and Methods. The usability and safety of the tested CAD were evaluated in adult patients with various wound types. Further endpoints were clinician satisfaction with dressing application and suitability for wound type and their opinion of the tested CAD compared with other dressings of this type. Results. The study included 83 patients with exuding wounds (42 male [51%]; 41 female [49%]) and a mean age of 74.54 years (SD ± 15.54 years). Thirteen clinicians (76%) (x = 1.24) rated the first CAD application as very easy, 4 (24%) as easy, and 1 (6%) as not easy. The time for dressing application was ranked as very good (x = 1.65) by 8 clinicians (47%), while 7 (41%) rated the time for application as good, and 2 (12%) gave a satisfactory rating. Conclusion. The CAD sheet and rope were safe to use and fit for purpose in wounds of various etiologies. In addition, the dressing was easy to handle and remove, formed a gel faster than other alginates, and outperformed other previous products.
Introduction
Complex secondary intention healing wounds are associated with significant health- related quality of life burden and high economic costs to society.1,2 Prevalence of complex wounds is projected to increase due to an aging population and increasing incidence of obesity, diabetes, and cardiovascular diseases.3 Secondary intention healing wounds can be managed with various dressings, depending on the etiology, wound condition, and patient-related factors. Maintaining a moist wound environment to optimize healing is a well-established evidence-based practice.4 This can be achieved by using first-line interactive/bioactive dressings, which provide a moist, conducive environment to promote wound healing.5 Alginates may be used for these wounds and can be either calcium or calcium sodium salts of alginic acid. When applied to a wound, the calcium in the alginate reacts with the sodium salts present in the wound exchanges, forming sodium alginate, which is a hydrophilic gel.6
Alginate is a naturally occurring biopolymer that is sourced from brown algae (Phaeophyceae), including Ascophyllum nodosum, Laminaria hyperborea, Laminaria japonica, Macrocystis pyrifera, and Laminaria digitate.7 Soluble sodium alginate gel forms due to active ion exchange of calcium ions for sodium ions at the wound surface, resulting in absorption of wound exudate.7 Alginate dressings are highly absorbable and are available as sheets for superficial wounds and ropes for packing deeper wounds.7-10 Alginates require a secondary dressing to keep the dressing in place and prevent it from drying out.11 Depending on the wound condition and the level of exudate, typically, alginates can be kept in place from 1 to 3 days, and they are changed when they have fully converted to a gel.11 A study was developed to evaluate a CAD in a real-world clinical setting when used for various wound types.
Materials and Methods
The international, multicenter, single-arm observational study applied a calcium alginate wound dressing for adult patients with various wound types to evaluate its clinical performance, usability, and safety of use. The tested dressing (Suprasorb A Pro; Lohmann & Rauscher, Germany) is a soft, conformable wound dressing containing a high proportion of mannuronic acid. When in contact with wound exudate, the dressing forms a gel, creating a moist wound environment, absorbing wound exudate, and promoting wound healing.11
The observational study was carried out in both a hospital and outpatient setting in 17 clinical centers in Germany (n = 7), Austria (n = 6), and Poland (n = 4) by a multidisciplinary team comprising 10 nurses (of whom one was a district nurse), 5 wound care specialists, and 2 physicians. The clinicians were asked to treat up to 8 wound patients, each using the CAD according to their local guidelines for a period of at least 3 dressing changes or more.
Primary endpoints
The study’s primary endpoints included ease of dressing application, the time required for dressing application, and the number of dressings used per patient. The clinical performance of the dressing was based on conformability upon application and when on the wound, autolytic debridement, absorbent and exudate management capacity of the dressing while maintaining a controlled moist wound healing environment, wound healing capacity, reduction of wound odor, and duration of treatment of each patient. Safety of dressing use was evaluated upon dressing removal (was the dressing removed in 1 piece, leaving no residue in the wound bed?) and maceration of wound edges.
Secondary endpoints
The secondary endpoints of the study included clinicians’ satisfaction with dressing use (was the goal set for the patient achieved?) and secondary dressing use. The etiology of the wound for which the dressing was used was factored into the analysis.
Tertiary endpoint
The study’s tertiary endpoint analyzed indications for the use of the dressing and clinicians’ opinions, comparing the tested CAD with other types of CADs they have used.
Data gathering and statistical analysis
The clinicians completed an electronic questionnaire at the end of each patient’s treatment and a general electronic questionnaire at the end of the study. Statistical analysis was performed using Microsoft Excel (Microsoft Corporation) and GraphPad Prism 9 (GraphPad Software, Inc).
For the final sample, 83 wounds were used for data analyses. Scaled variables were displayed as means ± SD. Categorical variables were displayed by frequency tables or cross-tabulations. A Likert scale ranging from 1 (very easy/good) to 6 (very complicated/inadequate) was used to score the variables.
In the case of decision-making questions, the thesis was considered proven if more than 70% agreed. For answers on the 6-point Likert scale, the thesis was considered correct if the rating was <2.
Ethical considerations
This international, multicenter, single- arm, observational study was conducted according to the guidelines of the Declaration of Helsinki. Since this was a study testing a CE (Conformite Europeenne)-registered product within the instructions for use and within everyday clinical practice without any additional patient risk while adhering to local rules and regulations, neither approval from the ethics committee nor from the federal authorities was required. Informed consent was obtained following local rules and regulations from all enrolled participants before starting the study.
Results
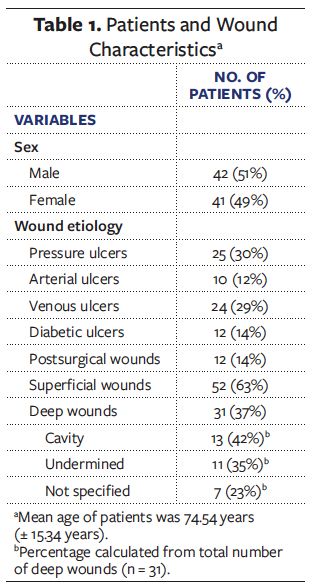
A total of 83 adult patients (42 male [51%]; 41 female [49%]) with a mean age of 74.54 years (SD ± 15.34 years) were included in the analysis. The patients suffered from highly exuding wounds of varying etiologies, comprising pressure ulcers (n = 25; 30%), arterial ulcers (n = 10; 12%), venous ulcers (n = 24; 29%), diabetic ulcers (n = 12; 14%), and postsurgical wounds (n = 12; 14%). The wounds were mostly superficial (n = 52; 63%); of the 31 deep wounds, 13 had cavities, 11 were open undermined wounds, and 7 were unspecified (Table 1).
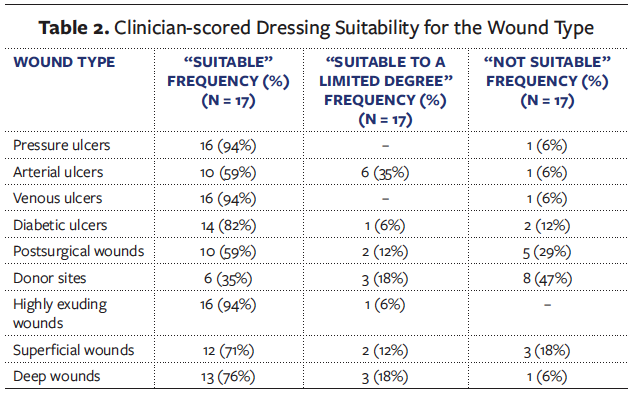
The attending clinicians (N=17) rated the tested CAD as suitable for use in most wound types. Of these, 16 (94%) rated the dressing as appropriate for pressure ulcers. Ten clinicians (59%) confirmed suitability for arterial ulcers, 16 (94%) for venous ulcers, and 14 (82%) for diabetic ulcers. Additionally, 10 (59%) confirmed the suitability for postoperative wounds and 6 (35%) for split skin donor sites. Sixteen clinicians (94%) considered the CAD suitable for heavily exuding wounds, 12 (71%) for superficial wounds, and 13 (76%) for deep wounds (Table 2).
In all but one of the 83 enrolled patients, the clinicians used various types of secondary dressings alone or in combination. These secondary dressings included super absorbent wound dressings (n = 44; 53%), foam dressings (n =38; 46%), elastic fixation bandages (n = 23; 28%), and short stretch bandages (n = 7; 8%). The use of more than 1 secondary dressing at the same time was possible, such as a superabsorbent dressing fixed with an elastic fixation bandage.
Handling of the dressing
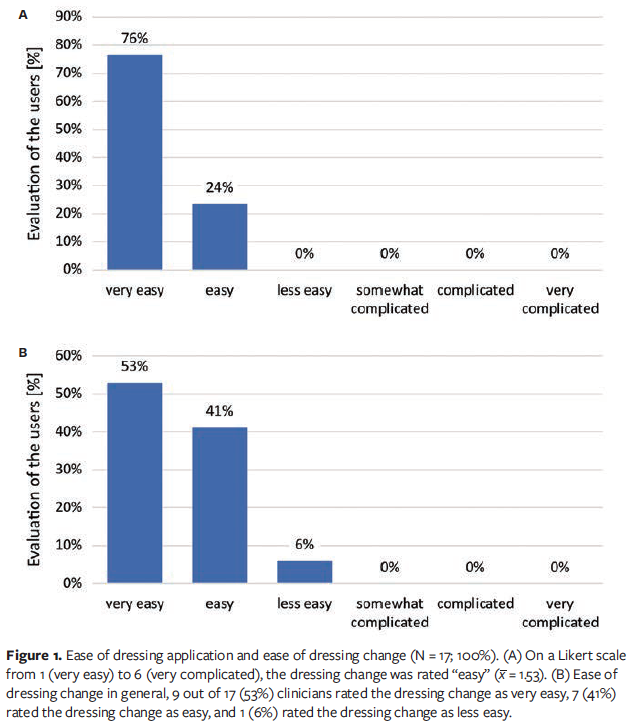
At the first dressing application, the clinicians (N = 17) used a Likert scale ranging from 1 (very easy) to 6 (very difficult) to score such factors as the ease of dressing application in general, the time required for the application, and the conformability of the dressing. Thirteen clinicians (76%) [𝑥̅ = 1.24] rated the first application as very easy, 4 (24%) rated the task as easy, and 1 (6%) rated the dressing change as less easy (Figures 1A and 1B). The time required for dressing application, in general, was rated as very good (𝑥̅ = 1.65) by 8 (47%) clinicians, while 7 (41%) rated the time required as good, and 2 clinicians (12%) scored this as satisfactory. Conformability of the dressing upon application was rated as very good by 4 clinicians (24%), whereas 12 (71%) rated the initial conformability as good (𝑥̅ = 1.82), and 1 clinician (6%) scored it as satisfactory. The CAD conformability to the wound bed in its gelled state was rated very good by 9 clinicians (53%), good by 7 (41%) (𝑥̅ = 1.59), and sufficient by 1 (6%).
Clinical efficacy
On average, the wounds were treated over a period of 35.06 days (SD ± 29.64 days), and the size of the wounds was reduced by 49.72% within the study period. The average dressing change interval was 3.52 days (SD ± 2.47 days).
When asked about setting multiple goals for their patients’ (N = 83) treatment using the alginate dressing, the clinicians reported that they aimed to achieve good exudate management in 62 patients (75%), anticipated autolytic debridement in 61 patients (73%), and wanted to support coagulation in 17 patients (20%). In 8 patients (10%), the clinicians had other goals comprising avoidance of infection, stabilizing the wound edges, and stimulation of granulation and epithelialization. At the end of the study, the clinicians reported having achieved the treatment goals in 74 (89%) of their patients.
In 20 patients, wound odor was present at the start of the study. In 13 of the 20 patients (65%), the wound odor had decreased at the end of the study, and in 7 cases (35%), the wound odor persisted.
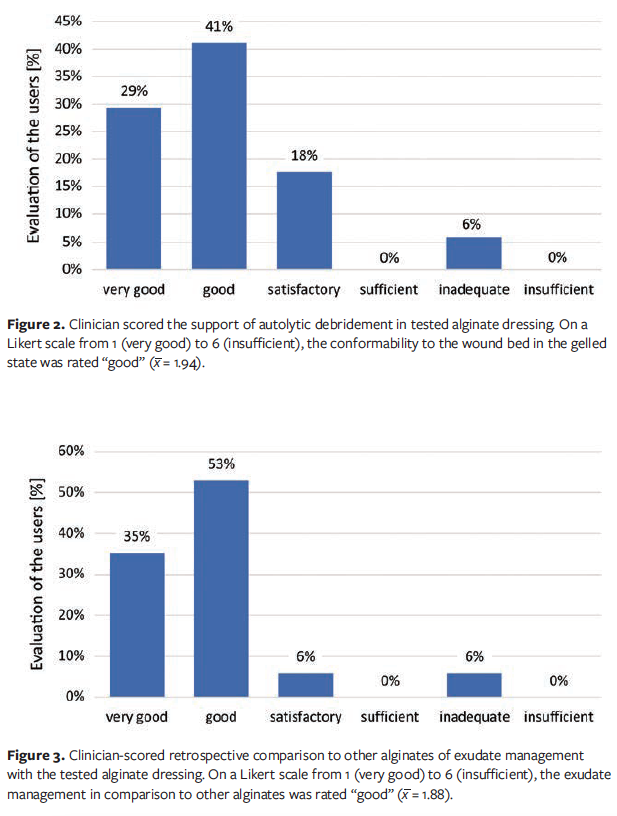
The clinicians (N = 17) scored various clinical features of the alginate dressing on a Likert scale from 1 (very good) to 6 (insufficient). For support of autolytic debridement in general, 5 clinicians (29%) rated the dressing’s performance as very good and 7 (41%) scored the performance as good (𝑥̅ = 1.94), while 3 clinicians (18%) gave a satisfactory rating, and 1 (6%) scored the autolytic debridement performance as inadequate (Figure 2).
Of the participating clinicians, 14 (82%) stated that the tested CAD was able to adequately absorb exudate. For 3 (18%) clinicians, this was only true to a limited degree. None stated that the tested CAD was not able to absorb exudate at all. Regarding absorption of dead tissue, 7 (41%) indicated that the tested CAD was able to do this adequately, while 8 (47%) stated that the wound dressing could only do this to a limited extent. Two clinicians (12%) stated that the CAD was unable to absorb dead tissue. (Evaluations noted in this paragraph were not based on a Likert scale.)
The clinicians were also asked for their opinions regarding how the tested CAD compared with other alginate dressings they had used. Exudate management of the test dressing was rated as very good by 6 clinicians (35%), while 9 (53%) gave a rating of good (𝑥̅ = 1.88); 1 clinician each (6%) gave ratings of satisfactory and inadequate (Figure 3). According to 15 (91%) out of 17 clinicians, the alginate dressing established a moist wound environment, while 2 (12%) gave an unsatisfactory rating for that capability.
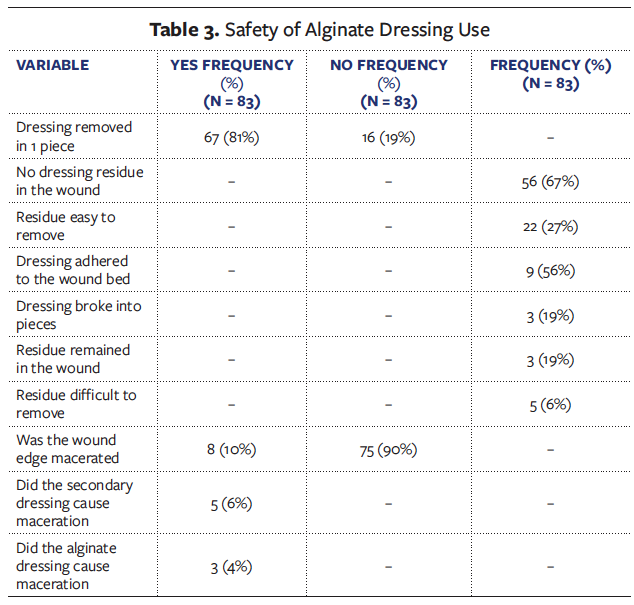
Safety aspects of dressing use
In 67 of 83 patients (81%), the dressing was removed from the wound in 1 piece. Of the 16 patients patients for whom this was not the case, the dressing stuck to the wound bed in 9 patients (56%), the dressing broke into several pieces in 3 patients (19%), and alginate fibers remained in the wound of 3 others (19%). In 56 of 83 patients (67%), the dressing was removed without leaving residue. In 22 patients (27%), any remaining residue was easy to remove, and in 5 patients (6%), the dressing left residue that was difficult to remove.
Maceration of the wound edges did not occur in 75 patients (90%) patients during the treatment with the tested CAD. However, in 5 patients (6%), maceration occurred due to the secondary dressing, and 3 patients (4%) had maceration due to the CAD (Table 3).
Sixteen (94%) of the clinicians indicated in a provided questionnaire that they would like to use the tested CAD in the future, while 1 (6%) indicated that they would not do so.
Discussion
Alginate dressings offer several advantages over other dressing types; in addition to being hemostatic, flexible, and highly absorbent, they form a gel with exudate, create a moist environment, can be easily removed, and can also be used as a wound filler.8,9 However, they are nonadhesive and therefore require a secondary dressing.10 Although alginate dressings rarely cause inflammatory or anaphylactic reactions, there have been reports of allergic reactions when there is not enough moisture within the wound cavity to form a removable gel.12
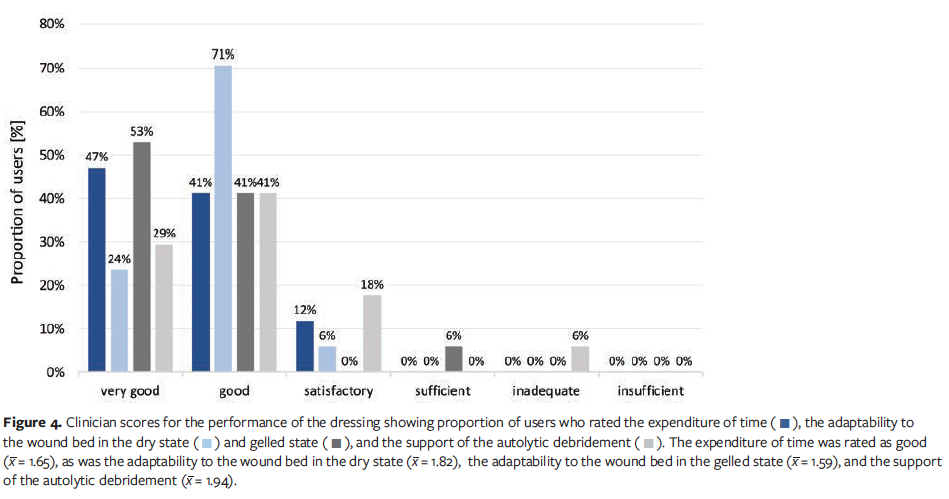
This current real-world study showed that clinicians rated the handling of the alginate dressing and its clinical performance for various wound types and etiologies as very easy/good or easy/good (Figure 4). In addition, at the end of the study, in 74 of 83 patients (89%), the clinicians reported that the CAD had met the treatment goals.
Alginate dressings are highly absorbent, biodegradable dressings used in moderately to highly exuding wounds. One of the benefits of using an alginate dressing is its efficacy in absorbing excess moisture from wounds.9,10,13 On bleeding wound sites, alginate dressings facilitate hemostasis due to the active release of calcium ions that aid the clotting mechanism.13 When used on a donor site, they can remain in place for up to 7 days.13 The clinicians involved in this study did not evaluate the CAD for use in donor sites; therefore, this application should be undertaken with caution.
The tested alginate dressing caused maceration in 3 of 83 patients (4%). In 22 patients (27%), the alginate dressing left residue upon dressing change; of these, 5 had residue that was difficult to remove. Although the fibers of the alginate dressing were reportedly easy to remove by rinsing the wound (n = 22; 27%), clinicians noted this performance as unfavorable. Nevertheless, these low frequencies of issues indicate that the product is safe to use.
When considering an alginate dressing, selecting the right dressing for the wound type is essential. Alginate rope dressings should be used with caution in narrow or very deep cavities because complete removal may be difficult.11 Clinicians should also avoid packing the material tightly into the cavity.11 Alginate dressings are not recommended in the management of anaerobic wound infections. If applying this type of dressing to an infected wound, clinicians should ensure that the secondary dressing is nonocclusive.11
With the exception of donor sites, various wound etiologies were scored as valid applications for the improved alginate dressing. Compared with earlier iterations, the newer CAD scored the same or better in the assessed parameters. Because of its superior performance, most of the surveyed clinicians reported a desire to switch to the improved alginate.
Limitations
There were several limitations of this study. For example, the study design did not include the evaluation of comparators. Instead, the tested CAD was evaluated in patients with various complex wound types in a real-world setting. Therefore, the present findings may not extend to other CADs with different formulations. In addition, the survey at the end of the study in which clinicians compared the CAD with their experiences using other dressings of this type was merely an observation of individual clinicians. Randomized controlled studies are needed to give a valid comparison of the performance of various alginate dressings. However, standardizing complex wounds has many challenges and does not necessarily provide the real-world clinical experience with wound dressings that this study did.
Conclusion
The sheet and rope CAD tested in this study met the requirements regarding handling, performance, and safety of use in wounds of various etiologies. In addition, the dressing was generally easy to handle and remove and, according to the clinicians, formed a gel faster than other alginates. Overall, the CAD clinically outperformed other alginate dressings the polled clinicians had used.
Acknowledgments
Authors: Renata Bienias, MSN; Marco Feulner; Stefan Hergenröder; Hannes Schrammel; Lisa Spreitzer; Elzbieta Szkiler, MSN; Adam Zielinski, MD, PhD; and Claas Roes, PhD
Affiliations: 1Remed Usługi Pielęgniarskie i Opiekuńcze, Olesno, Poland; 2MediCare Patientenberatung Strack e. K., Bad Staffelstein, Germany; 3Wundmanagement Gastl, Hammelburg, Germany; 4Wundmanagement Schrammel und Reiner OG, Gloggnitz, Austria; 5Ellipsa Medical Services GmbH, Lappersdorf, Germany; 6Indywidualna Specjalistyczna Praktyka Pielęgniarska, Elbląg, Poland; 7Centrum Medyczne Doktor A, Warszawa, Poland; 8Head of Scientific Support, Lohmann & Rauscher GmbH & Co. KG, Rengsdorf, Germany
Disclosure: The authors disclosed receipt of the following financial support for the research, authorship, and publication of this manuscript: This work was supported by L&R. An expense allowance was paid to study centers.
Correspondence: Lohmann & Rauscher GmbH & Co. KG, z.Hd. Dr. Claas Roes, Westerwaldstraße 4, 56579 Rengsdorf, Germany
References
1. Guest JF, Vowden K, Vowden P. The health economic burden that acute and chronic wounds impose on an average clinical commissioning group/health board in the UK. J Wound Care. 2017;26(6):292-303. doi:10.12968/jowc.2017.26.6.292
2. Olsson M, Järbrink K, Divakar U, et al. The humanistic and economic burden of chronic wounds: a systematic review. Wound Repair Regen. 2019;27(1):114-125. doi:10.1111/wrr.12683
3. Cheng Q, Gibb M, Graves N, Finlayson K, Pacella RE. Cost-effectiveness analysis of guideline-based optimal care for venous leg ulcers in Australia. BMC Health Serv Res. 2018;18(1):421. doi:10.1186/s12913-018-3234-3
4. Han G, Ceilley R. Chronic wound healing: a review of current management and treatments. Adv Ther. 2017;34(3):599-610. doi:10.1007/s12325-017-0478-y
5. Ather S, Harding KG, Tate SJ. 1 - Wound management and dressings. In: Rajendran S, ed. Advanced Textiles for Wound Care, 2nd ed. Woodhead Publishing; 2019:1-22.
6. Lee KY, Mooney DJ. Alginate: properties and biomedical applications. Prog Polym Sci. 2012;37(1):106-126. doi:10.1016/j.progpolymsci.2011.06.003
7. Aderibigbe BA, Buyana B. Alginate in wound dressings. Pharmaceutics. 2018;10(2):42. doi:10.3390/pharmaceutics10020042
8. O’Meara S, Martyn-St James M, Adderley UJ. Alginate dressings for venous leg ulcers. Cochrane Database Syst Rev. 2015;2015(8): CD010182. doi:10.1002/14651858.CD010182.pub3
9. Hickman DA, Pawlowski CL, Sekhon UDS, Marks J, Gupta AS. Biomaterials and advanced technologies for hemostatic management of bleeding. Adv Mater. 2018;30(4):1700859. doi:10.1002/adma.201700859
10. Weller C, Team V. Interactive dressings and their role in moist wound management. In: Rajendran S, ed. Advanced Textiles for Wound Care, 2nd ed. Woodhead Publishing; 2019:105-134.
11. Vowden K, Vowden P. Wound dressings: principles and practice. Surgery (Oxford). 2017;35(9):489-494. doi:10.1016/j.mpsur.2017.06.005
12. McCarthy S, Dvorakova V, O'Sullivan P, Bourke JF. Anaphylaxis caused by alginate dressing. Contact Dermatitis. 2018;79(6):396-397. doi:10.1111/cod.13100
13. McBride CA, Kimble RM, Stockton KA. Prospective randomised controlled trial of Algisite™ M, Cuticerin™, and Sorbact® as donor site dressings in paediatric split-thickness skin grafts. Burns Trauma. 2018;6:33. doi:10.1186/s41038- 018-0135-y






