



Decreased Health Care Expenditure and Average Length of Therapy With Facilitated Transition Discharge Program for Patients Receiving Negative Pressure Wound Therapy
Abstract
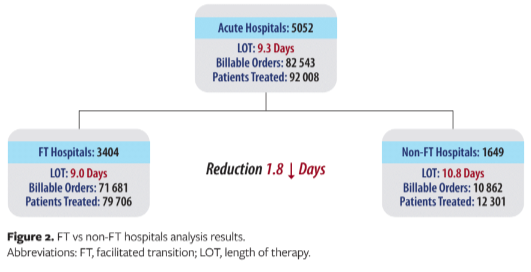
This study compares LOT between patients discharged from hospitals with FT discharge programs providing NPWT to patients at/before discharge versus those without (non-FT). FT facilities were further segmented: active-FT (≥1 transition order during past 90 days) versus inactive-FT (FT set up but no orders during past 90 days). There were 82 543 billable orders and 92 008 patients analyzed. LOT was 1.8 days shorter for FT versus non-FT facilities (potential per-patient savings of $5071 for FT facilities). LOT was 1.2 days shorter in active-FT versus inactive-FT facilities. This study shows shorter stays and LOT for patients in facilities actively using FT.
Abbreviations
FT, facilitated transition; LOT, length of therapy; NPWT, negative pressure wound therapy.
Introduction
Delays in hospital patient discharge are associated with increased cost and risk of
infection, lower patient satisfaction, and even mortality.1,2 Device consignment programs that allow for on-site home care equipment to be provided to the patient at or before hospital discharge can ease logistics and facilitate the transition out of acute care. This study compares the average length of inpatient NPWT between patients discharged from acute care facilities that have instituted an FT discharge program allowing for
on-site NPWT systems to be provided to the patient at or before discharge versus patients in facilities without such programs (non-FT).
Materials and Methods
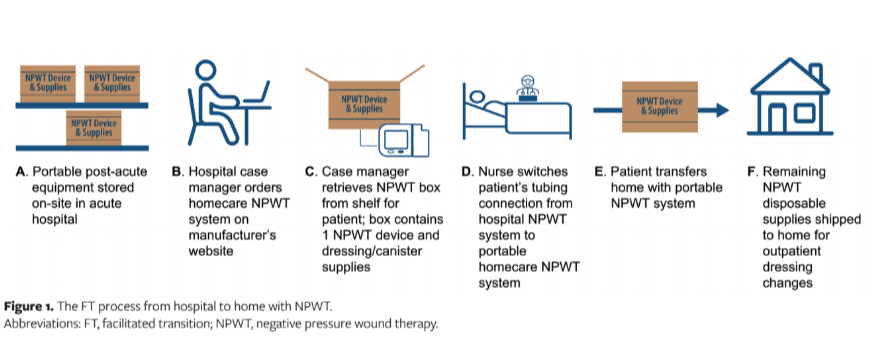
Billable orders from January 1, 2021 through September 30, 2021 were obtained through Oracle data sources and analyzed in 3-month rolling intervals. Hospitals with an FT discharge program (V.A.C. Ready Care Program, 3M) were further segmented into active FT facilities (≥1 FT program transition order within the prior 90 days) versus inactive FT facilities (FT program set up but no FT program transition orders within the past 90 days). Figure 1 is a description of the FT program.
Billable orders were counted for NPWT systems (ActiV.A.C. Therapy System, 3M) among patients treated with NPWT within the last 3 months. A total of 82 543 billable orders and 92 008 patients were analyzed. The average LOT was computed as: (sum of total inpatient therapy days)/(number of patients treated).
Results
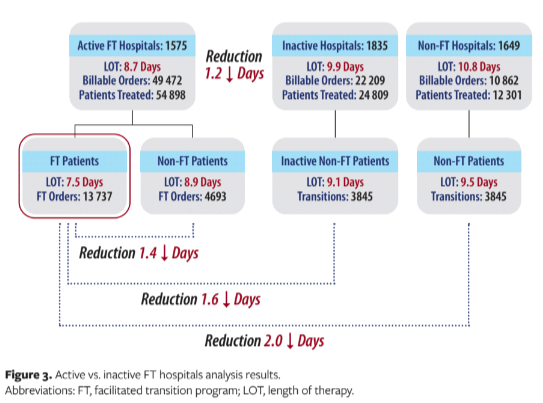
Inpatient LOT was 1.8 days shorter for FT versus non-FT facilities (9.0 vs 10.8 days); this equated to a potential per patient hospital savings of $5071 (1.8 days × $2817 estimated daily inpatient cost3) for FT facilities. Overall, 69% (49 472) of billable orders and 69% (54 898) of patients were in active FT facilities. Also, 75% (13 737) of transitions from active FT facilities were placed via the FT program. LOT was 1.2 days shorter in active FT versus inactive FT facilities (8.7 vs 9.9 days) and 1.4 days shorter for the FT program versus non-FT program discharges in active FT facilities (7.5 vs 8.9 days). There was a 2.0-day LOT decrease for the active FT program versus the non-FT program (7.5 vs 9.5 days). Results of the analysis are shown in Figures 2 and 3.
Discussion
Patient discharge processes are complicated and involve many cross-institutional complexities that contribute to delayed discharges. Particularly for patients being discharged from hospitals with high-tech equipment, in-hospital consignment programs are designed to streamline the ordering process and provide cost savings by reducing the risk of equipment-related delays. The return on investment can be high for these programs, because they are typically free and require only storage space and time to set up the program.
Results of this study showed a decrease in LOT of 2 days for patients in the active FT program versus the non-FT program (7.5 vs 9.5 days). LOT reduction is an important means for improving health care utilization and has been associated with improved patient satisfaction as well as potentially lower infection risk and cost.2,4-6 Consignment programs also limit the need for same-day deliveries, which reduces the service burden and overall health care system costs.
Limitations
There are several limitations to these study results. Importantly, the data did not account for delays due to other external factors. In addition, patient- and disease-specific complexities, hospital size, and number of NPWT systems in storage for FT facilities were unknown and not factored into the results. Also, the data set did not include an entire year of data, which may not fully account for seasonal effects.
Conclusion
This study shows the benefits of shorter inpatient stays and LOT for patients hospitalized in facilities actively using an FT program. Shorter inpatient stays and LOT may potentially reduce health care expenditures.
Acknowledgments
Authors: Leila Boti, MS; Laura Soloway, PhD, MPH; Deb Myers, BBA; Dinu Pillai, BS; and Javad Zabihi, MS
Acknowledgements: This information was presented at the Symposium on Advanced Wound Care Spring/Wound Healing Society Meeting in Phoenix, Arizona, April 6-10, 2022.
Affiliations: 3M Health Care, St. Paul, MN
Disclosure: All authors are employees of
3M Health Care.
Correspondence: Leila Boti, BS; 7703 Cypress View, Boerne, TX 78015; lboti@mmm.com
References
1. Thorup CB, Hougaard M, Blindum PF, Sørensen EE. Hospitalised patients’ experiences during negative pressure wound therapy due to surgical site infection after vascular and cardiac surgery. Int Wound J. 2018;15(5):707-716. doi:10.1111/iwj.12913
2. Rojas-García A, Turner S, Pizzo E, Hudson E, Thomas J, Raine R. Impact and experiences of delayed discharge: a mixed-studies systematic review. Health Expect. 2018;21(1):41-56. doi:10.1111/hex.12619
3. HCUP Reports. Healthcare Cost and Utilization Project (HCUP). Hospital Inpatient National Statistics 2017 (non-neonatal, non-maternal discharges only). Agency for Healthcare Research and Quality. Accessed Oct. 27, 2021. www.hcup-us.ahrq.gov/reports.jsp
4. Baek H, Cho M, Kim S, Hwang H, Song M, Yoo S. Analysis of length of hospital stay using electronic health records: a statistical and data mining approach. PLoS One. 2018;13(4):e0195901. doi:10.1371/journal.pone.0195901
5. Lagoe RJ, Abbott JH, Littau SA. Reducing hospital lengths of stay: a five-year study. Case Rep Clin Med. 2021;10(6):160-167. doi:10.4236/crcm.2021.106020
6. Park M, Giap TTT, Lee M, Jeong H, Jeong M, Go Y. Patient- and family-centered care interventions for improving the quality of health care: a review of systematic reviews. Int J Nurs Stud. 2018;87:69-83. doi:10.1016/j.ijnurstu.2018.07.006






