


Caregiver Burden in a Home-Based Primary Care Population: Is Assisted Living a Factor?
Abstract
Caregiver burden is an essential component of long-term care not evaluated within assisted living facilities (ALFs). This study assessed caregiver burden among caregivers of older adults enrolled in a home-based primary care program, comparing burden among caregivers of ALF residents vs patients cared for at home. Caregivers completed a survey with the Short Form Zarit Burden Interview (ZBI-12) via the patient portal; 76 of 364 caregivers completed the survey (20% response rate). The ZBI-12 was used to assess total caregiver burden, personal strain, and role strain. Most caregivers were White (81.3%), female (72%), and held a college degree or higher (79.1%). Male caregivers had higher mean total (23.4) and personal strain (19.7) scores, whereas higher education was associated with a higher role strain score (P=.0425). In exploratory subgroup analyses, caregivers of patients with Alzheimer disease had lower personal strain (P=.0462), and caregivers of patients with diabetes had lower role strain (P=.0473); given the small subgroup sizes and multiple comparisons, these findings are hypothesis-generating only. Caregiver burden did not differ between caregivers of higher-acuity ALF residents and caregivers of lower-acuity community-dwelling patients (mean total 18.6 vs 18.8). Because these represent different patient populations, this null result is consistent with—but does not prove—that ALF placement may only partially offset caregiver burden.
Citation: Ann Longterm Care. 2026. Published online June 24, 2026.
DOI:10.25270/altc.2026.31.004
In the United States, about 1 in 5 adults aged 18 years or older are anticipated to engage in caregiving activities over the course of their lives, predominantly for older individuals. The caregiving population largely comprises women, with a mean age of 49.4 years; approximately 1 in 4 caregivers is between 18 and 34 years of age.1 About 1 in 6 Americans care for an adult aged 50 years or older.2 Family members, friends, and other unpaid caregivers provide approximately 83% of the assistance received by older adults in the United States. Nearly 48% of these caregivers support individuals living with Alzheimer disease or other forms of dementia.2 Caregiver burden prevalence has increased due to the growing population with high chronic disease burden. Over 50% of caregivers experience medium to high burden depending on the time spent providing care and the care recipient’s level of functional dependency.2 In-home caregivers provide an average of 23.7 hours per week providing care, about 20% of whom provide more than 40 hours per week.2 The responsibilities include assisting with basic and instrumental activities of daily living, helping manage medications, scheduling appointments, accompanying the patient to medical visits, making care management decisions, and providing emotional support.
As defined by Zarit et al,3 caregiver burden is “the extent to which caregivers perceive that caregiving has had an adverse effect on their emotional, social, financial, physical, and spiritual functioning.” Factors associated with increased risk of caregiver burden include female sex, low education, and living with the patient.1 Although caregivers whose loved ones live in assisted living facilities (ALFs) may not live with the resident or provide personal care, they often remain involved in decision making. Caregiver burden in this population is often underrecognized and can lead to depression and poor health outcomes.4 Therefore, detecting and minimizing caregiver burden is essential for both the caregiver and the patient.
Previous studies have focused on describing caregiver burden in populations of patients based on specific diseases; however, little research has assessed caregiver burden among patients living in ALFs. Studying caregiver burden specifically in ALFs is important because, despite structured support services, caregivers often remain responsible for decision making, emotional support, and care coordination, and the extent to which ALFs alleviate this burden remains poorly understood. In this study, we aimed to assess caregiver burden among caregivers of older adults enrolled in a home-based primary care (HBPC) program and to compare burden among caregivers of patients residing in ALFs with the home setting.
Methods
After Institutional Review Board approval, patients were selected from the registry of the University of Texas Southwestern Medical Center HBPC program that provides in-home patient evaluation and management. For our study, “patients” refers to all individuals enrolled in HBPC; a subset resided in ALFs and are referred to as “residents” where applicable. For each patient, we identified their primary caregiver who had access to the patient's health information through MyChart (Epic's patient portal). Patients were excluded if they were on hospice or if the caregiver did not have access to MyChart. A survey was sent to the caregiver through MyChart. If the survey remained incomplete after 2 weeks, a reminder survey was sent once. If the survey was incomplete after an additional 2 weeks, caregivers were contacted by phone. The total follow-up period was approximately 4 weeks. The survey contained questions regarding demographics, relation to and amount of time spent with the patient, and the Short Form Zarit Burden Interview (ZBI-12),5 which assessed caregiver burden. Information on the patient’s chronic problems was retrieved from their chart on Epic.
Zarit Burden Interview
The ZBI-12 is a validated and reliable tool for measuring caregiver burden. It consists of 12 questions, each scored on a 5-level Likert scale, with 0 representing “never” and 4 representing “always.” The total score can be divided into 2 domains: personal strain (questions 1–10), which reflects the caregiver's emotional stress, frustration, and impact on personal well-being, and role strain (questions 11–12), which reflects feelings about the caregiver role itself, such as resentment or feeling trapped. Although there is no definitive consensus, prior studies have used this division.6 Accordingly, we used the exact question breakdown to analyze both domains of the ZBI-12 and the total ZBI-12 score against caregiver demographics and the number of chronic problems among patients.
Statistics
Descriptive statistics of patient characteristics were provided as frequencies and percentages for categorical measures. Differences in ZBI-12 scores and personal strain and role strain scores between the categorical demographic variables with 2 groups (such as sex, employment, and personal relationship status) were evaluated using the student t test. Differences in scores between categorical demographic variables with more than 2 groups were assessed using analysis of variance (ANOVA). All tests were 2-tailed and performed at the 0.05 significance level using R. Normality was assessed using visual inspection of histograms and Q-Q plots. Equal variances were evaluated using Levene test where appropriate. The final survey response rate was approximately 20%, which may introduce nonresponse bias if the characteristics or experiences of nonrespondents differ systematically from those who chose to participate. For the principal comparisons, mean differences in total ZBI-12 score are reported with 95% confidence intervals (CIs) and standardized effect sizes (Cohen d). To address the difference in case-mix between the assisted living and community groups, a multivariable linear regression of total ZBI-12 score was fit on caregiver sex, education, ALF status, and number of chronic problems. Because the disease- and demographic-specific comparisons were exploratory and no correction for multiple comparisons was applied, those P values should be interpreted as hypothesis-generating. To assess nonresponse bias, survey responders and nonresponders were compared on caregiver sex and number of chronic problems using the variables available for the full sampled cohort.
Results
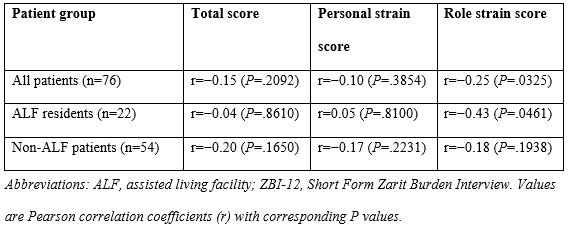
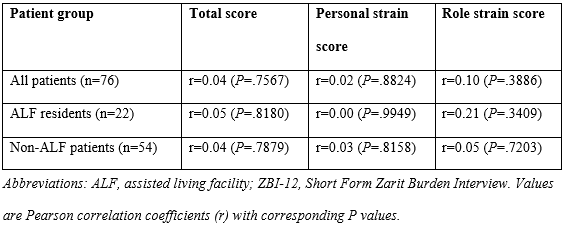
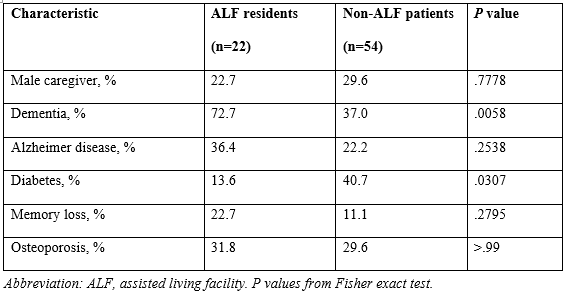
From July 2022 to September 2022, we received 76 responses out of 364 surveys sent. Demographics of the respondents are shown in Table 1. Most respondents were White (81.3%) and female (72%). Most had attained a college degree or higher (79.1%). Nearly 1 in 3 (29.7%) of patients were living in an ALF, and most caregivers were married to or were the child or parent of the patient (89.2%). When comparing ZBI-12 scores (total, personal strain, and role strain) among each demographic variable, as seen in Table 2, significant differences were found by caregiver sex, with male caregivers reporting higher mean total (23.4 vs 16.9; P=.0094) and personal strain scores (19.7 vs 13.3; P=.0033) than female caregivers, and by education, with higher educational attainment associated with greater mean role strain (P=.0425). No significant differences were found for ALF residents with mean total, personal strain, or mean role strain scores. Among patient medical conditions (Table 3), caregivers of patients with Alzheimer disease had lower personal strain (P=.0462) and caregivers of patients with diabetes had lower role strain (P=.0473), whereas no significant differences were observed for osteoporosis, chronic back pain, memory loss, or dementia; these exploratory subgroup findings are hypothesis-generating only. Subgroup sizes for all comparisons are reported in Table 2 and Table 3. When comparing the association between the number of chronic medical problems and total, personal, and role strain ZBI scores (Table 4), a greater number of medical problems was associated with decreased role strain for all patients (P=.0325) and patients in ALFs (P=.0461). In contrast, the number of medications was not significantly associated with total, personal, or role strain scores in any group (all P>.30; Table 5). The male–female difference in total burden corresponded to a moderate-to-large effect (mean difference 6.2 points; 95% CI, 1.4-11.0; Cohen d=0.66), whereas the ALF–non-ALF difference was negligible, with a CI that excluded a clinically meaningful effect (mean difference −0.4 points; 95% CI, −5.7 to 4.8; Cohen d=−0.04). In a multivariable model adjusting for caregiver sex, education, ALF status, and number of chronic problems (R²=0.16; model P=.013), male sex remained the only significant predictor of total burden (adjusted +6.5 points; 95% CI, 1.7-11.2; P=.009), whereas ALF status remained nonsignificant (−1.4 points, 95% CI, −6.1 to 3.4; P=.56). Baseline characteristics differed between the 2 groups (Table 6): ALF residents were substantially more likely than community-dwelling patients to have a dementia diagnosis (72.7% vs 37.0%; P=.006), confirming a higher-acuity ALF population. Survey responders and nonresponders did not differ significantly in caregiver sex (27.6% vs 24.7% male; P=.70) or number of chronic problems (P=.60).
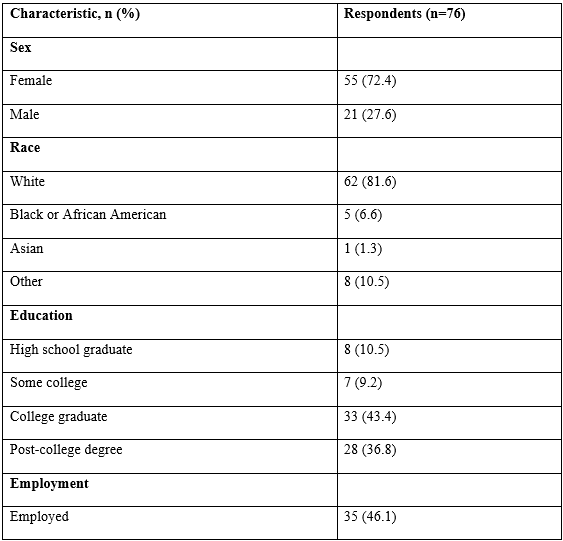
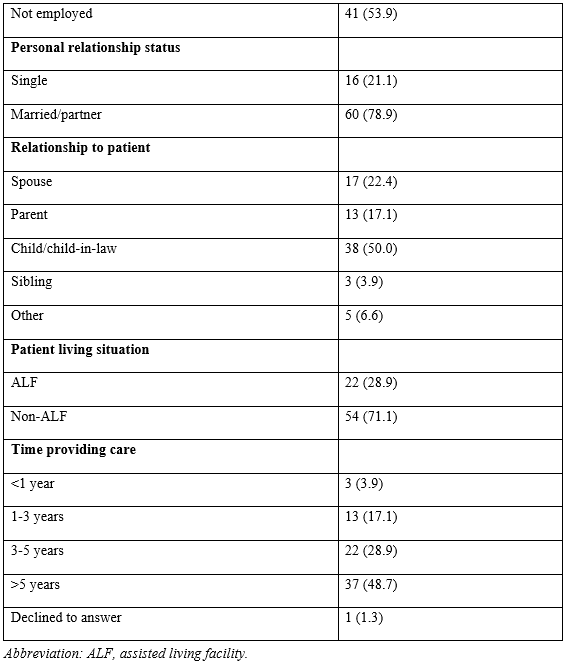
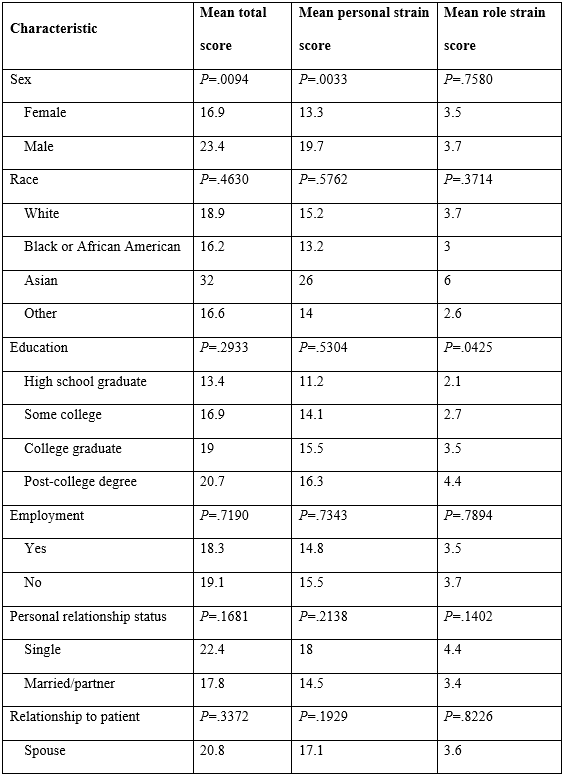
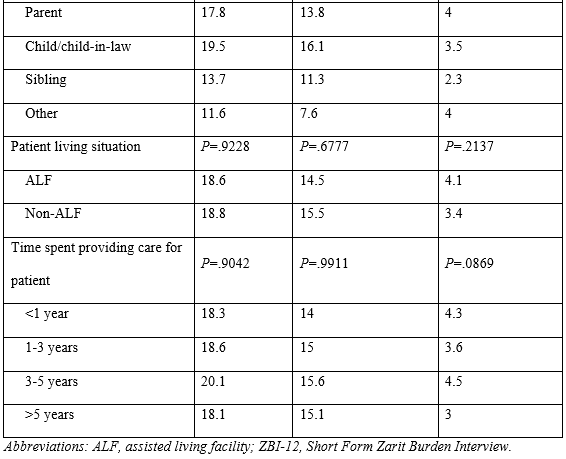
Table 3. Differences Between Patients’ Medical Conditions and Total, Personal Strain, and Role Strain ZBI-12 Scores
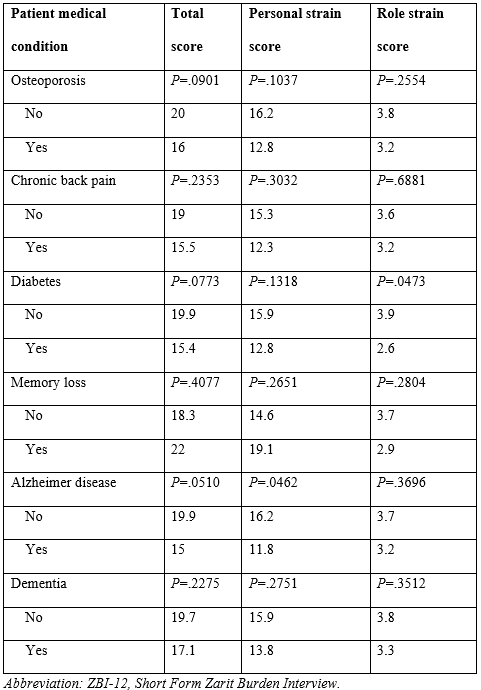
Table 4. Number of Medical Problems and Associated Total, Personal Strain, and Role Strain ZBI-12 Scores
Discussion
Principal Findings
This cross-sectional study explored the demographic, social, and caregiving-related factors that influence caregiver burden among individuals supporting older adults in ALFs. The findings suggest that male caregivers reported higher burden than female caregivers across all 3 domains, and higher educational attainment was associated with greater role strain. Although most respondents were female, the higher burden among the smaller group of male caregivers was robust to adjustment for education, ALF status, and medical complexity. This pattern may reflect true associations or may be influenced by response bias, with caregivers who are more aware of their burden—potentially due to higher health literacy—being more likely to complete the survey and report higher burden levels. Additionally, our study found that, regardless of setting, caregivers of patients with diabetes and Alzheimer disease had lower caregiver burden compared with those caring for patients without either disease. It is possible that caregivers of patients with diabetes or Alzheimer disease may receive more structured external support, including disease-specific education, case management, and caregiver resources, which may help mitigate the burden. Additionally, caregivers of individuals with Alzheimer disease or diabetes may have clearer expectations regarding disease progression, which could help reduce emotional strain. However, these findings should be interpreted with caution, as they may also reflect selection bias within the surveyed population or unmeasured differences in disease severity. For all patients, including those residing in ALFs (residents), a greater number of medical problems was associated with a lower reported caregiver burden. There was no significant association of caregiver burden with the number of medications. Similarly, no significant difference in burden was found for caregivers of residents in ALFs vs caregivers of patients living at home.
In contrast to most prior literature, which identifies female sex as a risk factor for higher caregiver burden, our results showed higher burden among male caregivers. This unexpected finding should be interpreted cautiously given the small number of male respondents (n=21) and the possibility of selection among those who chose to respond; it may also reflect differences in caregiving role, expectations, or reporting and warrants confirmation in larger samples. However, the observed association between higher education and greater caregiver burden may reflect a higher likelihood of survey participation by caregivers with higher educational attainment rather than a true population-level relationship. The impact of education on caregiver burden may be due to confounding factors. In contrast, those with higher educational attainment may experience increased strain as they balance the competing pressures of their professional and caregiving responsibilities. The observed finding in our study could also be skewed by the location of the population study, primarily drawn from a region comprising individuals with greater wealth and education levels.
Additionally, caregivers of individuals with diabetes and Alzheimer disease reported a lower burden compared with caregivers of individuals without these conditions. This may reflect the higher prevalence of these diseases among older adults, which has led to the development of targeted management resources. However, the presence of resources does not necessarily equate to a reduction in caregiver burden, and further research is needed to evaluate the effectiveness of these interventions. Notably, caregivers of those with Alzheimer disease may experience less burden due in part to the additional support services often available for dementia care within ALFs.
A greater number of medical problems was associated with a decreased burden. Older adults with more medical problems may have more resources at their disposal, thus relieving some of the burden for caregivers.
No other characteristics were found to have any associations in our study, which may reflect limited generalizability. Most studies analyzing predisposing factors to caregiver burden focus on homogeneous populations with a particular disease, such as stroke, Parkinson’s disease, or cancer.7-9 The generalizability of these data is therefore limited. Although associations may be found with certain illnesses, they may not apply to the general population, which may explain why our study did not find other significant associations.
Notably, the lack of significant findings regarding caregiver burden in ALFs vs non-ALFs was unexpected. Although ALFs can alleviate stress on informal caregivers by providing such services as meals, medication monitoring, personal care, and health and wellness programs,10 ALFs may be chosen for individuals with greater functional impairment.11 As a result, caregivers of ALF residents may still face substantial demands compared with those caring for more functionally independent individuals at home. Furthermore, the move to an ALF may cause stress to the older adult, which can result in new or worsening depression or other comorbidities. Thus, ALF placement does not necessarily minimize caregiver burden as expected in every instance. In our study population, although functional impairment was not directly measured, patients residing in ALFs tended to have a higher number of chronic medical conditions compared with those living at home, suggesting greater medical complexity that may have contributed to sustained caregiver burden.
Assisted Living and the Comparison of Populations
An important interpretive caveat is that the ALF and non-ALF groups are not the same patients observed in 2 settings but 2 structurally different populations. ALF placement is rarely a random event; it is the endpoint of a decision driven on the patient side by progressive functional and cognitive decline, behavioral and psychological symptoms of dementia, fall risk, and incontinence, and on the caregiver side by caregiver exhaustion, the caregiver’s own health, geographic distance, competing demands, and financial capacity. Consistent with this selection process, ALF residents in our sample were roughly twice as likely to have a dementia diagnosis as community-dwelling patients (72.7% vs 37.0%; P=.006). An unadjusted comparison of these nonequivalent groups therefore cannot establish whether ALF placement reduces burden for a given patient; that question would require a within-patient or case-matched design. Read in this light, the absence of a burden difference between a higher-acuity ALF group and a lower-acuity home group is itself indirect evidence that placement relieves some burden—enough to offset the higher baseline acuity of ALF residents. The domain pattern supports this interpretation: ALF caregivers reported numerically lower personal strain (14.5 vs 15.5) but higher role strain (4.1 vs 3.4) than community caregivers, the shift one would expect if placement reduced hands-on personal care while increasing the care coordination and advocacy that drive role strain.
Regardless of location, constant stress from caregiving leads to a decreased quality of life for caregivers. Many caregivers experience limitations in their own daily activities and ability to care for themselves, depending on the time spent caring for a patient.12 Larson et al13 found that reducing this burden can significantly increase the caregiver's quality of life. Anxiety, depression, and other health consequences are also common among caregivers.12 Social withdrawal and physical decline together erode the mental health capacity that most strongly predicts care quality.14,15 Screening for caregiver burden can be done via the ZBI-12. Interventions to reduce caregiver burden include psychoeducation, cognitive behavioral therapy, caregiver support groups, and the provision of medications for patients with behavioral and psychological symptoms of dementia.1
The major strengths of this study are access to detailed electronic medical records and patient/caregiver online communication through MyChart, which increased the accessibility of our research. Like many other survey-based studies, our study is subject to limitations, including a relatively low survey response rate of 20% and incomplete data, both of which introduce nonresponse bias and limit the generalizability of our findings to the broader caregiver population. The caregiver population in our study was primarily White, female, and highly educated, which may limit the extent to which these findings apply to more diverse populations. The study sample could not be expanded, as participants were drawn exclusively from the HBPC registry. Several additional limitations warrant emphasis. The disease- and demographic-specific associations were based on small subgroups, and no correction for multiple comparisons was applied; most reached only borderline significance and should be regarded as exploratory and hypothesis-generating rather than confirmatory. Diagnoses were coded as present or absent without grading of severity, so a binary dementia or Alzheimer disease flag may combine mild and advanced disease. The ALF vs non-ALF comparison was unadjusted and drawn from two nonequivalent populations and therefore cannot determine whether ALF placement reduces burden for an individual patient. Functional status and caregiver age were not available for analysis, limiting the case-mix characterization. Finally, with only 21 male respondents, the higher burden observed among men requires confirmation in larger and more balanced samples.
Clinical Implications
These findings carry a practical message for HBPC programs and ALF medical directors: caregiver burden persists in the assisted living setting at levels comparable to home, so placement should not be treated as the endpoint of caregiver support. Caregivers of ALF residents warrant active burden screening as much as caregivers of community-dwelling patients, and possibly more, given the higher role strain observed in this group. The ZBI-12 is a brief, validated instrument suitable for this purpose, and our results support its use among ALF caregivers in addition to community caregivers. When elevated burden is identified, evidence-based interventions include caregiver psychoeducation, structured respite, dementia-specific support groups, and care coordination by HBPC or ALF medical staff, with pharmacologic management of behavioral and psychological symptoms of dementia where appropriate. Because burden among ALF caregivers appears to involve care coordination and advocacy more than hands-on personal care, interventions that streamline communication between families and facility staff may be especially valuable.
Conclusion
This study identified several factors associated with caregiver burden. Greater burden was observed among male caregivers and those with higher education levels. In exploratory analyses, caregivers of patients with diabetes or Alzheimer disease reported lower burden, a hypothesis-generating finding. Caregiver burden did not differ between caregivers of ALF residents and caregivers of community-dwelling patients; because these groups represent different, nonequivalent populations, this null result does not establish that ALF placement fails to reduce burden, but it does indicate that placement alone should not be assumed sufficient to resolve it. Caregivers of ALF residents remain an at-risk group requiring active burden screening. Further research with larger, more representative, and case-matched samples is needed to validate these findings.
Key Clinical Summary
- Caregiver burden remained substantial among caregivers of older adults enrolled in a home-based primary care program and did not differ significantly between caregivers of assisted living facility (ALF) residents and caregivers of community-dwelling patients.
- Male caregivers reported significantly higher overall caregiver burden and personal strain than female caregivers, while higher educational attainment was associated with greater role strain, highlighting subgroups that may benefit from targeted support and screening.
- Placement in an ALF should not be assumed to resolve caregiver burden; ongoing assessment using validated tools such as the Zarit Burden Interview and access to caregiver support interventions remain important regardless of care setting.
Affiliations, Disclosures & Correspondence
Matthew Cali1, Ethan Fan, MD2, Namirah Jamshed, MD3
Affiliations:
- Department of Internal Medicine, University of Pittsburgh Medical Center, Pittsburgh, PA
- Department of Internal Medicine, Texas Health Dallas, TX
- Department of Internal Medicine, UT Southwestern Medical Center, Dallas, TX
Disclosure: The authors declare no conflicts of interest.
Address correspondence to:
Namirah Jamshed, MD
Email: namirah.jamshed@utsouthwestern.edu
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Annals of Long-Term Care or HMP Global, their employees, and affiliates.
References
- Adelman RD, Tmanova LL, Delgado D, Dion S, Lachs MS. Caregiver burden: a clinical review. JAMA. 2014;311(10):1052-1060. doi:10.1001/jama.2014.304
- AARP and National Alliance for Caregiving. Caregiving in the US 2025. July 24, 2025. Accessed June 20, 2026. https://www.aarp.org/pri/topics/ltss/family-caregiving/caregiving-in-the-us-2025/
- Zarit SH, Reever KE, Bach-Peterson J. Relatives of the impaired elderly: correlates of feelings of burden. Gerontologist. 1980;20(6):649-655. doi:10.1093/geront/20.6.649
- Swartz K, Collins LG. Caregiver care. Am Fam Physician. 2019;99(11):699-706.
- Gratão ACM, Brigola AG, Ottaviani AC, et al. Brief version of Zarit Burden Interview (ZBI) for burden assessment in older caregivers. Dement Neuropsychol. 2019;13(1):122-129. doi:10.1590/1980-57642018dn13-010015
- Branger C, O'Connell ME, Morgan DG. Factor analysis of the 12-item Zarit Burden Interview in caregivers of persons diagnosed with dementia. J Appl Gerontol. 2016;35(5):489-507. doi:10.1177/0733464813520222
- Kazemi A, Azimian J, Mafi M, Allen KA, Motalebi SA. Caregiver burden and coping strategies in caregivers of older patients with stroke. BMC Psychol. 2021;9(1):51. doi:10.1186/s40359-021-00556-z
- Aamodt WW, Kluger BM, Mirham M, et al. Caregiver burden in Parkinson disease: a scoping review of the literature from 2017-2022. J Geriatr Psychiatry Neurol. 2024;37(2):96-113. doi:10.1177/08919887231195219
- Park S, Mazanec SR, Burant CJ, Bajor D, Douglas SL. Caregiver burden in distance caregivers of patients with cancer. Curr Oncol. 2022;29(11):8967-8974. doi:10.3390/curroncol29110704
- Assisted living facts and figures. American Health Care Association/National Center for Assisted Living (AHCA/NCAL). Accessed March 28, 2024. https://www.ahcancal.org/Assisted-Living/Facts-and-Figures/Pages/default.aspx
- Cummings SM, Cockerham C. Depression and life satisfaction in assisted living residents. Clin Gerontol. 2004;27(1-2):25-42. doi:10.1300/j018v27n01_04
- Liu Z, Heffernan C, Tan J. Caregiver burden: a concept analysis. Int J Nurs Sci. 2020;7(4):438-445. doi: 10.1016/j.ijnss.2020.07.012
- Larson J, Franzén-Dahlin A, Billing E, Arbin M, Murray V, Wredling R. Predictors of quality of life among spouses of stroke patients during the first year after the stroke event. Scand J Caring Sci. 2005;19(4):439-445. https://doi.org/10.1111/j.1471-6712.2005.00369.x
- Pohl JS, Thoits P, Roth DL, et al. Family caregiver social isolation and health: findings in the National Survey of Caregiving. Innovation in Aging. 2019;3(Suppl 1):S438-S439. https://doi.org/10.1093/geroni/igz038.1645
- Hiel L, Beenackers MA, Renders CM, Robroek SJ, Burdorf A, Croezen S. Providing personal informal care to older European adults: should we care about the caregivers' health? Prev Med. 2015;70:64-68. doi:10.1016/j.ypmed.2014.10.028
