


Beyond Symptoms: How Pulmonary Artery Pressure Monitoring With the CardioMEMS™ HF System Guides Heart Failure Management
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Cath Lab Digest or HMP Global, their employees, and affiliates.
CLD talks with Matthew H. Gonzalez, MD.
Advanced Heart Failure and Transplant Cardiologist, Corewell Health, Grand Rapids, Michigan; Clinical Assistant Professor of Medicine, Michigan State University
This interview is sponsored by Abbott.
Individual patient results may vary. This reflects one center’s clinical experience.
Heart failure is a growing national burden, with an expanding patient population and high mortality, especially after hospitalization. As a chronic, progressive disease, some patients advance to later stages, and outcomes often worsen with repeat admissions.
From your perspective as an advanced heart failure specialist, what are the biggest hurdles in managing these patients effectively?
There are several major challenges. The first is that patients with heart failure can appear less sick than they truly are, even to a heart failure cardiologist. As much as it pains me to say it, relying on the traditional physical exam and on patients’ symptom narratives doesn’t always tell the full story. We still get burned if we don't have an objective way to assess the status of a patient's HF, such as hemodynamic data.
 The second challenge is working with our non-advanced heart failure cardiology colleagues around referrals. This is a very difficult patient population, and there is constant tension around when to send a patient. Is it too early? Is it too late? More than 90% of providers caring for patients with stage C and advanced heart failure are not advanced heart failure specialists. As a field, we have struggled with how to optimize which patients we see and when. What we do know is that, nationally, we are still seeing patients too late. When you really dig into the data, I don’t think that it is anyone’s fault. This is an incredibly hard population to assess.
The second challenge is working with our non-advanced heart failure cardiology colleagues around referrals. This is a very difficult patient population, and there is constant tension around when to send a patient. Is it too early? Is it too late? More than 90% of providers caring for patients with stage C and advanced heart failure are not advanced heart failure specialists. As a field, we have struggled with how to optimize which patients we see and when. What we do know is that, nationally, we are still seeing patients too late. When you really dig into the data, I don’t think that it is anyone’s fault. This is an incredibly hard population to assess.
Many individuals who ultimately require advanced therapies such as left ventricular assist devices (LVADs) are implanted at INTERMACS 1 or 2, when outcomes would likely have been better if they had been identified earlier, at INTERMACS 3 or 4.*
What has become increasingly clear, through the American Heart Association’s Cardiogenic Shock Registry data and through data from CardioMEMS™ HF System clinical trials, including CHAMPION, GUIDE-HF, and MONITOR-HF, is that understanding pulmonary artery (PA) pressures, whether in the hospital or remotely, enables proactive management that helps reduce morbidity and mortality. Regardless of symptoms, elevated PA pressures are associated with increased mortality risk.1,2
*Interagency Registry of Mechanically Assisted Circulatory Support (INTERMACS) 1 = critical cardiogenic shock; INTERMACS 2 = declining function despite intravenous inotrope support; INTERMACS 3 = stable but inotrope dependent; INTERMACS 4 = resting symptoms on oral therapy at home.3
Given these challenges, can you talk more about why PA pressure monitoring is important in the management of heart failure? And how has technology like the CardioMEMS™ HF System helped you address some of these unmet needs in heart failure management?
Pulmonary artery pressure monitoring is important because once the CardioMEMS™ HF System is implanted, it gives us objective, actionable data on a daily basis. After implantation, the patient goes home and simply lies on a special reader or mat each day to take a PA reading, which transmits the signal. That data is sent to us through the Merlin.net™ PCN application, and we can pull up the patient’s waveforms, which look essentially identical to what you would see with a PA catheter in place. So we know very clearly whether Mr. Smith’s PA pressures are within the goal we have set for that day or not.
The real art is how do you build a CardioMEMS™ HF System program that can efficiently respond to outliers and actually do something with that information? If you don’t act on the data, it is not going to help anyone. You also have to protect your program. We all only have 24 hours in a day, and this has to be efficient as the program grows.
What we have done at Corewell is structure management around two phases: optimization and maintenance.
During the optimization phase, we review daily pressures and tailor management to the patient’s specific heart failure phenotype. Heart failure with preserved ejection fraction (HFpEF) and HF with reduced EF (HFrEF) require different approaches. We focus on titrating guideline-directed medical therapy (GDMT) and, when necessary, decongestion. Sometimes this involves trial and adjustment, guided by pressure trends, symptoms, and response to therapy. In our program, we generally target a PA mean <30 mmHg and a PA diastolic <25 mmHg. We know that elevations beyond those ranges are associated with a significantly increased risk of mortality.
During the optimization phase, we build a patient-specific action plan. By the end of the optimization phase, ideally the patient is at what I would call a healthy hemodynamic level, is optimized on GDMT, and we have a clear plan in the chart outlining what works for them.
At that point, we want the patient to coast. That brings us to the maintenance phase. For a program to be sustainable, the majority of patients need to be stable, at goal, and not triggering notifications.
A small subset of patients — in our program, about 5% — enter what we call the “red zone.” These are patients whose pressures remain elevated despite optimization. At that point, we take a multidisciplinary approach and discuss why their pressures remain high.
We have identified patients who needed cardiac resynchronization therapy (CRT) optimization. We have found chronic total occlusions that we have intervened on after multidisciplinary discussion. We have referred patients for an LVAD because their PA pressures remained elevated, and they had the appropriate structural features of low ejection fraction and dilated ventricles that made that decision reasonable.
Patients can coast in the maintenance phase for long periods of time, until they don’t. When pressures drift out of range repeatedly and nurses have to intervene more than once, that patient gets pulled back into the red zone for a deeper evaluation.
It really is a platform centered on a simple principle: elevated PA pressures are risky. The CardioMEMS™ HF System empowers us with data to objectively identify those at risk. Once you establish that, the next step becomes much clearer: Why are their PA pressures elevated, and is this patient a candidate for something that can meaningfully change their trajectory? What can we do to lower PA pressures in a way that meaningfully helps the patient?
Could you share with us some of the latest outcomes data for the CardioMEMS™ HF System in heart failure management? How has it influenced mortality rates, heart failure hospitalizations, patient satisfaction and/or the optimization of GDMT in your heart failure patients?
 I’ll start with the CHAMPION trial4, which was the original randomized controlled trial evaluating the CardioMEMS™ HF System. It included about 550 patients overall, with comparable numbers in each group, and importantly, all patients received the CardioMEMS™ HF System. The difference was that half of the patients were actively monitored, meaning their PA pressures were used to guide management, while the other half received usual care.
I’ll start with the CHAMPION trial4, which was the original randomized controlled trial evaluating the CardioMEMS™ HF System. It included about 550 patients overall, with comparable numbers in each group, and importantly, all patients received the CardioMEMS™ HF System. The difference was that half of the patients were actively monitored, meaning their PA pressures were used to guide management, while the other half received usual care.
In the monitored group, if PA pressures were elevated, clinicians acted on that information regardless of whether the patient reported symptoms. A patient could say, “I feel fine,” but if pressures were up, the response might be to increase diuretics or optimize GDMT. It is also worth noting that all patients in CHAMPION were already considered optimized on GDMT by heart failure cardiologists, so this wasn’t a comparison against undertreated patients.
The primary endpoint looked at heart failure hospitalizations at six months. This was a relatively small trial, limited to NYHA class III patients, and it was not powered to detect a mortality signal, which is an important point. What CHAMPION did show was an early and meaningful separation of the curves for the composite endpoint of hospitalization and mortality, driven primarily by a reduction in heart failure hospitalizations. There was about a 28% reduction in heart failure-related hospitalizations.4
What I really like about the data is the mechanism. The first question is: Okay, hospitalizations went down, but why? Follow-up analyses showed that more actions were taken in the CardioMEMS™ HF System treatment arm.5 There were more medication changes — more diuretic adjustments, more GDMT optimization — compared with the control group.5 The next logical question is whether those actions actually lowered PA pressures, and the answer was yes. Patients in the CardioMEMS™ HF System arm had significant reductions in PA pressures compared with usual care.6 That really completes the circle: asymptomatic elevations in PA pressure are identified, clinicians act on them, pressures come down, and decompensation events that would have led to hospitalization are prevented.
More recently, Dr. Zile and colleagues published a pooled analysis (2025) combining CHAMPION, GUIDE-HF, and five CardioMEMS™ HF System registries, totaling over 4,000 patients.2 This larger dataset allowed for evaluation of mortality, and lower PA pressures were associated with a significant decrease in mortality, with consistent benefit across both HFrEF and HFpEF populations. Systolic, diastolic, and mean pressures are all predictive of outcomes.
One clinically useful observation from that analysis was that each 1 mmHg reduction in PA pressure during the first 6 months was associated with approximately a 3% improvement in survival at 2 years.2 While observational in nature, it provides a helpful framework for understanding the relationship between hemodynamics and outcomes.
Regarding patient experience, both anecdotal observations and published data7 suggest high acceptance. Patients who choose this approach are generally engaged and willing to transmit daily readings.
Avoiding hospitalization is also meaningful. Heart failure admissions are burdensome for patients and often associated with a decline in functional status. Many patients report feeling better after pressures are lowered, even if they initially did not recognize symptoms. Published analyses from CHAMPION and subsequent studies have shown improvements in quality-of-life measures using validated heart failure instruments,4,8 and some reports suggest improvement in functional capacity metrics such as six-minute walk distance.8,9
Taken together, the trial data and real-world experience support the concept that sustained reductions in PA pressure are associated with improved clinical outcomes.
Can you describe the procedure to implant the CardioMEMS™ HF System?
The implantation procedure is straightforward, particularly for operators comfortable with right heart catheterization. Fundamentally, it is performed as a standard right heart cath and can be done via either internal jugular or femoral venous access using a 12-French sheath.
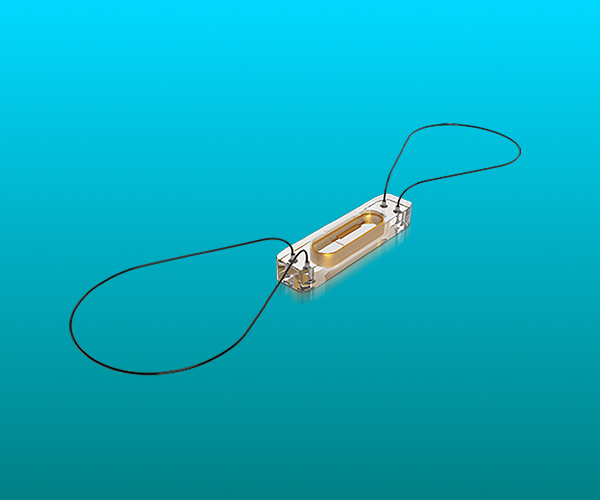
The procedure begins with routine hemodynamic assessment. The operator then advances into the left pulmonary artery and performs a limited pulmonary angiogram to identify an appropriate target vessel, typically a posterior branch. The device is approximately 10 mm in width, and the final position is often similar to the location where one would normally obtain wedge measurements during angiography.
After selecting a suitable landing zone, an .018-inch guidewire is advanced slightly distal to the intended implant site. The delivery catheter is then advanced over the wire, and the device is deployed in the chosen position.
Following deployment, calibration is performed. The delivery catheter is removed, a Swan-Ganz catheter is reintroduced, and simultaneous pressure measurements are obtained to confirm appropriate correlation between invasive readings and the device-generated values. Once satisfactory correlation is established, the procedure is complete.
From start to finish, the procedure usually takes about 30 to 45 minutes. Overall, it is a very straightforward and efficient implant.
What is the ideal time that patients should be seen for evaluation for a CardioMEMS™ HF System?
That’s an important question, and I tend to think about it in two ways.
First, I’ll use an example. The ROADMAP study10 evaluated LVAD therapy in INTERMACS 4 or better patients, what we sometimes call the “walking wounded.” These are stage D heart failure patients who are not in shock, not inotrope dependent, and not hospitalized, but remain significantly limited despite medical therapy. They often don’t look critically ill.
What was striking was how patients perceived their health. A substantial proportion of those who declined an LVAD described their health as “exceptional.” That underscores a reality we see in practice: patients do not always appreciate how sick they are. I love my patients, and listening to their stories matters, but sometimes they truly don’t realize how sick they are.
That’s exactly the kind of patient I worry about. Outside of a trial, I might look at that person and say, “Okay, I’ll see you back in six months or a year.” And that’s when they fall off the cliff. That’s when they show up in the hospital in shock. That’s when my colleagues play Monday-morning quarterback and ask, “Why didn’t Dr. Gonzalez send this patient sooner?”
My honest response is this is hard. What would have helped is objective data. If I had CardioMEMS™ HF System data showing that this patient’s PA mean was 35, I wouldn’t care that my patient told me they felt exceptional. If I have a patient with HFrEF, an EF of 20%, and a PA mean of 35, as an advanced heart failure cardiologist I’m immediately asking, why is this patient not being evaluated for advanced therapies?
That’s where the CardioMEMS™ HF System can be helpful. We only touch a small fraction of these patients, and we depend heavily on referrals. This problem is even bigger for general cardiologists, who see many more patients and have less time with each one. Just imagine a world where you actually knew the PA pressures of your heart failure patients. It makes referral decisions far more objective.
At the end of the day, any patient who’s been admitted multiple times for heart failure, doesn’t tolerate GDMT, continues to have symptoms, and despite appearing compensated, has high-risk hemodynamics on right heart catheterization, is someone who should at least get an eyeball from an advanced heart failure cardiologist.
Managing heart failure patients with the CardioMEMS™ HF System requires integrating new data into clinical workflows. How do you incorporate CardioMEMS monitoring into your day-to-day practice, and what challenges or efficiencies have you experienced?
Integrating the CardioMEMS™ HF System into practice requires infrastructure. In our case, we are fortunate to have three advanced practice providers (APPs) who don’t have dedicated time, yet do a fantastic job of integrating it into their daily schedules. You absolutely need APP support and nursing support for this to work.
Right now, at Corewell, we are following about 198 patients. For the program to be sustainable, you want only a small percentage of those patients triggering notifications at any given time. If you do the upfront work correctly, the response to an alert becomes very straightforward, meaning what we do when a patient is out of range, and ideally that intervention quiets things down. Only a very small subset of patients should continue to trigger alerts repeatedly.
That’s where our “red zone” concept comes in. For those patients, we hold a multidisciplinary meeting once a month. I also think it is important to have periodic (at the very least, annually), program-level meetings to review how things are working overall and to discuss challenging patients. A big part of those discussions is asking, how can we help the system with this patient who keeps alerting? Sometimes, continuing to escalate diuretics isn’t the answer, and the CardioMEMS™ HF System helps us recognize when we need to change strategy rather than repeat the same intervention that isn’t working.
This naturally ties back to referrals. We’re fortunate to be at a center with advanced heart failure capabilities, including LVAD and transplant, so when persistent elevations in PA pressure reveal that a patient needs more than medical therapy, we have those options available. If you are not in an urban center or at a quaternary hospital with advanced therapies, one way to help both the patient and your system is to refer those patients to a center that does have those capabilities. Persistently elevated PA pressures can be a very clear marker that it is time to do so.
CardioMEMS™ HF System programs should exist in any center with a meaningful heart failure population. Whether implantation is done by general or interventional cardiology, you need to have the infrastructure in place: how you are going to follow patients, who is reviewing the data, and what you are going to do when patients go out of range. That takes some work on the front end, but if you do it right, the program should largely coast, and in the process, actually help both patients and the healthcare system.
For physicians in the community who are considering adopting the CardioMEMS™ HF System, what practical advice can you offer to help optimize both workflow integration and patient care?
Because this is highly program-dependent, my first piece of advice is to see an established program in action. If you are starting from scratch, visiting a center with an operational CardioMEMS™ HF System program can be extremely helpful. You may not replicate their workflow exactly, but observing how they structure monitoring, escalation, and follow-up provides a concrete framework to adapt to your own environment.
Operational planning is critical. Before implanting your first device, you need clarity on authorization pathways, cath lab access, and most importantly, who is responsible for reviewing incoming data. That team must not only monitor transmissions, but also understand how to interpret PA pressures and respond appropriately.
As the program grows, infrastructure becomes increasingly important. Beyond simply using the monitoring platform, you need a longitudinal tracking process. Establish clear medication titration strategies, define what constitutes an out-of-range alert, and agree on standardized response pathways. I think it is helpful to structure care around an initial optimization phase followed by a maintenance phase. That approach promotes sustainability and reduces unnecessary reactive interventions.
You also need to decide, as a group, what you are going to do with patients who consistently have elevated pressures. Are you going to agree that, at some point, you need to look under the hood more deeply? And if you truly don’t have the time or resources to do that locally, are you willing to refer those patients out? Having that agreement ahead of time is important.
The last thing I would emphasize is that anyone setting up a CardioMEMS™ HF System program should, at a minimum, track their rehospitalization data. If you are doing this right, those numbers will improve. And at the end of the day, that’s how you get buy-in and ongoing support from your healthcare system and from local payers.
View the CardioMEMS HF System Indications, Safety & Warnings Here
References
1. Zalawadiya S, Abraham J, Rathman L, et al. Early reduction of pulmonary artery pressures is associated with improved mortality among Medicare beneficiaries with heart failure. JACC Heart Fail. 2025;13(10):102589. doi:10.1016/j.jchf.2025.102589
2. Zile MR, Abraham WT, Stevenson LW, et al. Relationship between remote, ambulatory pulmonary artery pressures, and all-cause mortality in patients with chronic heart failure. Circ Heart Fail. 2025 Jun;18(6):e012754. doi:10.1161/CIRCHEARTFAILURE.124.012754
3. Stevenson LW, Pagani FD, Young JB, et al. INTERMACS profiles of advanced heart failure: the current picture. J Heart Lung Transplant. 2009 Jun;28(6):535-541. doi: 10.1016/j.healun.2009.02.015
4. Abraham WT, Stevenson LW, Bourge RC, et al. CHAMPION Trial Study Group. Sustained efficacy of pulmonary artery pressure to guide adjustment of chronic heart failure therapy: complete follow-up results from the CHAMPION randomised trial. The Lancet. 2016;387:453-461. doi:10.1016/S0140-6736(15)00723-0
5. Costanzo MR, Stevenson LW, Adamson PB, et al. Interventions linked to decreased heart failure hospitalizations during ambulatory pulmonary artery pressure monitoring. JACC Heart Fail. 2016 May; 4(5): 333-344. doi:10.1016/j.jchf.2015.11.011
6. Adamson PB, Abraham WT, Stevenson LW, et al. Pulmonary artery pressure-guided heart failure management reduces 30-day readmissions. Circ Heart Fail. 2016 Jun; 9(6): e002600. doi:10.1161/CIRCHEARTFAILURE.115.002600
7. Rathman LD, Sears SF, Brett ME, et al. Patients report increased control and decreased impact of heart failure during pulmonary pressure-guided management. ESC Heart Fail. 2025 Oct; 12(5): 3381-3387. doi:10.1002/ehf2.15364
8. Lindenfeld J, Zile MR, Desai AS, et al. Haemodynamic-guided management of heart failure (GUIDE-HF): a randomised controlled trial. The Lancet. 2021 Sep 11; 398(10304): 991-1001. doi:10.1016/S0140-6736(21)01754-2
9. Case L, Deibert J, Jonsson O, Preister S. Treating PA pressures with use of a CardioMEMS device affects quality of life measures by improving Kansas City Cardiomyopathy Questionnaire (KCCQ) and 6 minute walk test (6mwt). Heart & Lung. 2020 Mar-Apr; 49(2): 217. https://doi.org/10.1016/j.hrtlng.2020.02.025
10. Stehlik J, Estep JD, Selzman CH, et al; ROADMAP Study Investigators. Patient-reported health-related quality of life is a predictor of outcomes in ambulatory heart failure patients treated with left ventricular assist device compared with medical management: results from the ROADMAP study (Risk Assessment and Comparative Effectiveness of Left Ventricular Assist Device and Medical Management). Circ Heart Fail. 2017 Jun;10(6):e003910. doi:10.1161/CIRCHEARTFAILURE.116.003910
™ Indicates a trademark of the Abbott group of companies.
©2026 Abbott. All Rights Reserved.
MAT-2602461 v1.0 | Item approved for global use.
