An Interesting Case of a Tattoo Artist’s Subdermal Chest Implants
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of ePlasty or HMP Global, their employees, and affiliates.
Questions
- What are body modifications?
- What is the history of body modification in comparison with that of breast implants?
- What is the prevalence of body modification in the United States?
- What are the complications associated with body modifications, and how do they compare with the complications associated with implants placed by board-certified plastic surgeons?
Case Description
A younger woman presented to a local hospital in Louisville, Kentucky with complaints of chest pain, fatigue, low-grade fever, and emesis. The patient had visited a tattoo artist in the southeastern United States 6 days prior to hospital admission, where she had custom silicone body-modification implants placed under her clavicles (Figure 1). Four days post-placement, she experienced a progressive increase in redness and pain associated with grossly purulent drainage; she presented to the emergency department 2 days later. Upon examination, the patient was found to have erythema and crepitus over the bilateral chest wall, as well as a Laboratory Risk Indicator for Necrotizing Fasciitis score of 7 and subcutaneous gas on computed tomography (Figure 2), Because of concern for necrotizing soft tissue infection, the general surgery team emergently undertook foreign body removal and debridement of the chest wall. Cultures grew Streptococcus pyogenes. The patient returned to the operating room on postoperative days (POD) 1 and 3 for additional debridement and wound vac exchanges. Because of the extent and complexity of the wound, the plastics and reconstructive surgery (PRS) team was consulted for reconstruction. On POD 9, the PRS team performed complex chest wound repair with hematoma evacuation. The patient was discharged on POD 11 (Figure 3). When she was seen in the clinic 4 weeks post-reconstruction, there were no signs of infection and the incision was healing appropriately. She was then lost to follow-up, and no additional images could be obtained.
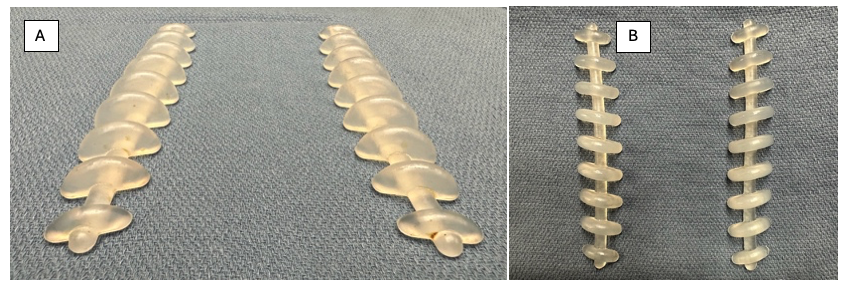
Figure 1. The subdermal custom silicone body modifications shown at (A) worm’s and (B) bird’s eye views.
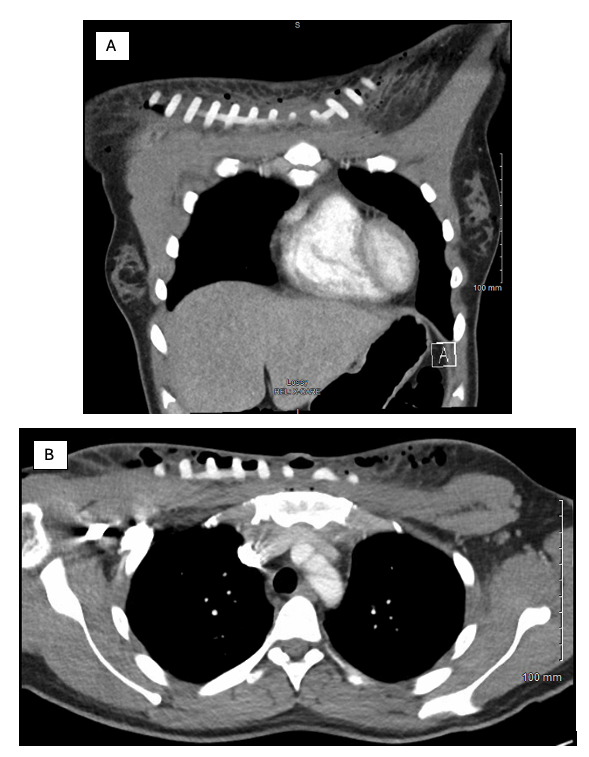
Figure 2. Preoperative computed tomography films of the silicone implants shown at (A) coronal and (B) axial views.

Figure 3. Intraoperative images of the complex wound spanning across the inferior aspect of the clavicle (A) prior to and (B) after closure of the wound.
Q1. What are body modifications?
Body modification, also known as body art, involves deliberately changing the human anatomy or physical appearance. They exist in 3 forms: permanent, semipermanent, or temporary. Body gems, glitter body art, and face and body paint are all temporary forms of body modification. Transdermal implants and piercings are semipermanent. Tattoos can be either permanent or temporary. Finally, subdermal implants, scarification, branding, skinning, and body stretching and sculpting are permanent modifications.1 We will focus primarily on permanent and semipermanent forms of body modification for this case.
Today, tattoos and piercings are the most common forms of body modification.1 Piercings are semipermanent because the skin defect left behind is not guaranteed to close, and healing times range anywhere from 4 to 36 weeks post-jewelry removal depending on vascularity. Tattoos can be either permanent or semipermanent depending on the depth of ink involvement; only the ink residing in the dermis is permanent, as the epidermis continually sloughs, and ink depth ranges from 0.6 to 2.2 mm.
Transdermal implants are another form of semipermanent modification, which involve creating a 1-way hole to hold a small anchor beneath the skin. Attached to the anchor is a “step” that projects through the integument. In contrast, subdermal implants, like those in our case (Figure 1), can be comprised of silicone, polytetrafluoroethylene, or metal, and sit in a subcutaneous pocket, creating a raised, visible design.1,2
Scarification creates permanent designs via scratching, etching, or cutting into the skin. Branding represents an extreme variant, where images are burned onto the body using tools such as an electrocautery knife, laser, hot or cold metal, chemicals, or a tattoo gun without ink. Additionally, skinning involves single-line cuts into the skin to be removed or peeled. People who undergo body stretching use implants to enlarge a body part beyond its normal size; this is often seen in the ear, much like piercing. Body sculpting, the last of the permanent body modifications, includes techniques like tongue splitting, where the middle of the tongue is split from the tip back to resemble a reptile’s tongue.
Q2. What is the history of body modification in comparison with that of breast implants?
The history of body modification or body art is extensive, complex, and multifaceted. The use of tattoos dates to back 3000 BCE, which was brought to light in 1991 when hikers on the Italian-Austrian border found the remains of an ancient, frozen individual with extensive tattoos.1,3,4 The tattoos of “Ötzi the Iceman” were found primarily on the joints, hinting at medicinal motives in the form of acupuncture to treat pain. Since then, body modification has been used in various forms across different civilizations, from the elites of the Roman empire to tribes in Africa. In recent times, piercings have increased in prevalence as a result of jewelry availability, fading negative stereotypes, and convenience. Subdermal implants, as in our case, were recently invented and popularized by Steve Haworth, also known as the “Modfather.”5 His original inspiration derived from his father’s employment as a surgical equipment manufacturer. Haworth diverted from a traditional line of work to create silicone-based body jewelry, which is growing in popularity.
Compared with these nontraditional body modifications, breast implants, often inserted via a sterile process by a board-certified plastic surgeon, have been through vigorous testing and multiple iterations after facing prior scrutiny. The first modern breast implants were introduced by Thomas Cronin and Frank Gerow in 1962, with the first commercially available products—manufactured by the Dow Corning Corporation—reaching the market in 1964.6 The earlier generations of breast implants were associated with high capsular contracture rates, implant failure, gel migration and silicone bleeding, carcinogens, cosmetic disadvantages, pronounced inflammatory reactions, low-grade silicon, and contamination due to improper manufacturing, which led to strict rules being enacted by various regulatory bodies. Arguably, the most defining moment in the history of breast implants occurred in the 1980s when the US Food and Drug Administration (FDA) decided to designate breast implants as a class III medical device; this required rigorous medical testing and FDA approval before a device could be sold and marketed. The newest, sixth generation of breast implants contains a smooth outer surface, an ergonomic and rheologic filler, and an advanced multilayer elastomer shell designed to reduce complications.
Q3. What is the prevalence of body modification in the United States?
The prevalence of body modifications increased in the United States beginning with the counterculture movement in the 1970s and continues to increase today.1,3,7 An unpublished 1990 survey of 10 000 US households found that 3% of the population reported tattoos.8 In 1997, the estimated number of tattoos ranged from 7 million to 20 million people, or 13% of the population.9 In 2012, the Harris Poll reported that 1 in 5 Americans had at least 1 tattoo.10 By 2017, up to 38% of Americans had at least 1 body modification, and, in 2023, 17% of Americans had more than 1 tattoo.3,11 Furthermore, in 2006, Laumann et al observed that 14% of Americans reported body piercings.12 Other body modifications such as subdermal implants, tongue splitting, and deformities of the skull have also increased in recent years, although they are not as common as tattoos.13
Body modifications are more common among adolescents and millennials.11 In 1997, 10% of the population had tattoos, with 56% of individuals having gotten their first tattoo in high school.9 In 2012, a survey reported that 40% of Americans aged 18 to 29 years have a tattoo.14 In addition, women are more likely to have body piercings, while men are more likely to have tattoos.12 An anonymous 2002 survey stated that 60% of women vs 42% of men had body piercings.15 Overall, the earlobe is the most common location of body piercings, with 77% of American survey respondents reporting having pierced at least 1 ear (n = 345).11,16 Other popular locations for body piercing include the mouth, navel, tongue, nose, eyebrows, and genitals. There are many reasons individuals choose to undergo body modification, including religious, cultural, social, cosmetic, medical, personal, and sexual reasons.1
Q4. What are the complications associated with body modifications, and how do they compare with the complications associated with implants placed by board-certified plastic surgeons?
The use of body modifications comes with risk. Overall, complication rates for body piercings were reported in 17% to 46% of cases, with infections in 10% to 30% of all body piercings.17,18 In contrast, most literature suggests an overall incidence of surgical site infections (SSIs) of less than 1% in all aesthetic surgeries performed by all plastic surgeons combined.19
The complications associated with body modification are numerous and include skin infections, bleeding, tissue trauma, immune-mediated reactions, allergic reactions, and psychological effects. Body modifications can cause local skin infections such as cellulitis, contact eczema, and atopic dermatitis, as well as rare systemic infections, including tetanus, tuberculosis, and hepatitis.7,8,16,20 Modifications in the mouth can lead to broken or swollen teeth, tongue abscess, or Ludwig’s angina.1,18 Perichondritis and abscesses can form in the ears and nose.18,21 Piercings in the genital region can cause pelvic inflammatory disease, prostatitis, strictures, and testicular infection.18 In addition to infections, body modification can lead to bleeding, tissue trauma, and keloid scarring.7,15
Hematoma occurrence secondary to plastic surgery varies depending on the procedure performed and the patient population, ranging from 3% to 15% in lipoabdominoplasty and 0.6% to 5.7% in breast augmentation surgery. In fact, there is a less than 2% rate of postoperative bleeding as a result of improved plastic surgery techniques.19 Body modification may trigger immune-mediated reactions such as foreign body reactions (ie, metal), autoimmune diseases with deposition in lymph nodes, angioedema, and granuloma formation.22 Tissue trauma may also occur, resulting in superficial nerve damage leading to increased and lasting pain.18 Permanent modifications are associated with psychological effects such as a lower mental quality of life, increased risk for suicidality, and reported negative behaviors in adolescents.17,20,23 Specifically, complications of subdermal implants include infection; scarring; migration of the implant; and tendon, nerve, or ligament damage.24 Individuals with extreme body modifications are associated with a higher risk of psychological and physical complications.13 Because subdermal implants require surgery, a large concern with this procedure is that the individuals who typically perform these procedures, such as tattoo artists, are unqualified to perform these procedures and may be doing so in unsanitary conditions, increasing the risk for serious complications.24
Overall, the main concern of these procedures is that they are performed in unsanitary conditions. In 2021, a questionnaire reported a 3-times-higher rate of medical complications for street or home tattooing compared with a studio or licensed medical center location.25 Van Hoover et al attributed delayed visits to health care providers in favor of advice from professional piercers as a main contributor to higher rates of complications.17 This may be due to the fact that many piercers may not have adequate knowledge on infection control. A 2022 study of 172 tattoo artists in Ethiopia showed that their knowledge of how to control infections was minimal.26 This highlights the need for proper education for both body modification artists and the general population who may seek various forms of body art. It is important to note that the legislation of body art varies from state-to-state across the US.27
Acknowledgments
Authors: Alexander L. Mostovych, MS1; Claire Fell, BS1; Joshua D. Spiegel, MD, MPH2; Carter Prewitt, BA1; Aryana Jones, MD3; Ryan L. Shaprio, MD2
Affiliations: 1University of Louisville School of Medicine, Louisville, Kentucky; 2Division of Plastic and Reconstructive Surgery, Department of Surgery, University of Louisville, Louisville, Kentucky; 3Division of General Surgery, Department of Surgery, University of Louisville, Louisville, Kentucky.
Correspondence: Alexander L. Mostovych, MS, 550 South Jackson Street Ambulatory Care Building (ACB), 2nd Floor, Louisville, KY 40202, USA. E-mail: almost01@louisville.edu
Disclosures: The authors disclose no financial or other conflicts of interest
References
1. Dunn D. Body art and the perioperative process. AORN J. 2016;104(4):326-340.e4. doi:10.1016/j.aorn.2016.07.011
2. Smith FD. Caring for surgical patients with piercings. AORN J. 2016;103(6):583-596. doi:10.1016/j.aorn.2016.04.005
3. Perper M, Aldahan AS, Tsatalis JP, Nouri K. Modifications of body surface: piercings, tattoos, and scarification. Int J Dermatol. 2017;56(3):351-353. doi:10.1111/ijd.13539
4. Lineberry C, Anderson S. The worldwide history of tattoos. Smithsonian Magazine. Updated October 18, 2023. Accessed February 20, 2024, https://www.smithsonianmag.com/history/tattoos-worldwide-history-144038580/
5. Silverman L, director. Flesh and Blood [film]. 2007.
6. Santanelli di Pompeo F, Paolini G, Firmani G, Sorotos M. History of breast implants: back to the future. JPRAS Open. 2022;32:166-177. doi:10.1016/j.jpra.2022.02.004
7. Meltzer DI. Complications of body piercing. Am Fam Physician. 2005;72(10):2029-2034.
8. Anderson RR. Tattooing should be regulated. N Engl J Med. 1992;326(3):207. doi:10.1056/NEJM199201163260318
9. Armstrong ML, Murphy KP. Tattooing: another adolescent risk behavior warranting health education. Appl Nurs Res. 1997;10(4):181-189. doi:10.1016/s0897-1897(97)80560-5
10. Braverman S. One in five U.S. adults now has a tattoo. PR Newswire. February 23, 2012. Accessed February 20, 2024. https://www.prnewswire.com/news-releases/one-in-five-us-adults-now-has-a-tattoo-140123523.html
11. Statista. Body modification in the United States - Statistics & Facts. Statista Research Department. 2023. Accessed October 12, 2025. https://www.statista.com/topics/1148/body-modification/
12. Laumann AE, Derick AJ. Tattoos and body piercings in the United States: a national data set. J Am Acad Dermatol. 2006;55(3):413-421. doi:10.1016/j.jaad.2006.03.026
13. Weiler SM, Tetzlaff BO, Herzberg PY, Jacobsen T. When personality gets under the skin: need for uniqueness and body modifications. PLoS One. 2021;16(3):e0245158. doi:10.1371/journal.pone.0245158
14. Pew Research Center. Millennials: Confident. Connected. Open to Change. Washington, DC. February 24, 2010. https://www.pewresearch.org/social-trends/2010/02/24/millennials-confident-connected-open-to-change/. Accessed October 12, 2025.
15. Mayers LB, Judelson DA, Moriarty BW, Rundell KW. Prevalence of body art (body piercing and tattooing) in university undergraduates and incidence of medical complications. Mayo Clin Proc. 2002;77(1):29-34. doi:10.4065/77.1.29
16. Preslar D, Borger J. Body piercing infections. 2023 Jul 10. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–.
17. Van Hoover C, Rademayer CA, Farley CL. Body piercing: motivations and implications for health. J Midwifery Womens Health. 2017;62(5):521-530. doi:10.1111/jmwh.12630
18. Stirn A. Body piercing: medical consequences and psychological motivations. Lancet. 2003;361(9364):1205-1215. doi:10.1016/S0140-6736(03)12955-8
19. Montrief T, Bornstein K, Ramzy M, Koyfman A, Long BJ. Plastic surgery complications: a review for emergency clinicians. West J Emerg Med. 2020;21(6):179-189. doi:10.5811/westjem.2020.6.46415
20. Kluger N, Misery L, Seité S, Taieb C. Body piercing: a national survey in France. Dermatology. 2019;235(1):71-78. doi:10.1159/000494350
21. Folz BJ, Lippert BM, Kuelkens C, Werner JA. Hazards of piercing and facial body art: a report of three patients and literature review. Ann Plast Surg. 2000;45(4):374-381. doi:10.1097/00000637-200045040-00004
22. Nielsen C, Andréasson K, Olsson H, Engfeldt M, Jöud A. Cohort profile: the Swedish Tattoo and Body Modifications Cohort (TABOO). BMJ Open. 2023;13(5):e069664. doi:10.1136/bmjopen-2022-069664
23. Hicinbothem J, Gonsalves S, Lester D. Body modification and suicidal behavior. Death Stud. 2006;30(4):351-363. doi:10.1080/07481180600553419
24. Armitage R. Extreme body modification implants causing complications, health authorities warn. ABC News. April 16, 2018. Accessed February 20, 2024. https://www.abc.net.au/news/2018-04-16/extreme-body-modification-procedure-causing-horror-complications/9664130
25. Korn L, Bonny-Noach H, Koren G, Nissanholtz-Gannot R. Factors associated with medical complications after body art among Israeli adults: a retrospective study. Isr J Health Policy Res. 2021;10(1):39. doi:10.1186/s13584-021-00474-w
26. Tamene A, Yemane B. A study of body modification artists' knowledge, attitudes, and practices toward infection control: a questionnaire-based cross-sectional study. Risk Manag Healthc Policy. 2022;15:713-725. doi:10.2147/RMHP.S361711
27. 2023 state legislation on body art. National Environmental Health Association. January 9, 2024. Accessed February 7, 2025. https://www.neha.org/2023-body-art-review