COVID-19 Realization: The Critical Need for Pharmacists in Health Care and Relationship to Provider Status
 COVID-19 is rapidly reshaping how we live our lives in unimaginable ways, forcing us to review as pharmacists how we practice in a new light. This pandemic puts a strain on the nation’s health care system, most especially on the supply of qualified health care providers. Pharmacists have the ability to provide important health care services during this time. The question is are we ready and do we have the proper training to assume roles which may place us in unfamiliar circumstances.
COVID-19 is rapidly reshaping how we live our lives in unimaginable ways, forcing us to review as pharmacists how we practice in a new light. This pandemic puts a strain on the nation’s health care system, most especially on the supply of qualified health care providers. Pharmacists have the ability to provide important health care services during this time. The question is are we ready and do we have the proper training to assume roles which may place us in unfamiliar circumstances.
Many of the places where pharmacists are currently needed in the current health care system is in the provision of medical assistance/first aid, COVID-19 testing, providing information through a call center, and direct patient triage. In addition, medication reconciliation using a standardized, consistent approach is critical. I want to focus on medical assistance, namely first aid, COVID-19 testing, and direct patient triage. Are we ready for these clinical activities? What skills do we need? The patient care process provides the pharmacist with the necessary skills to be able to conduct all of these important care responsibilities.
The patient care process involves the following steps: Gather Patient Information (subjective [review of systems (ROS), social determinants of health] and objective [physical examination, health screening, laboratory data interpretation]), followed by the ability to assess information in order to apply this data to patient triage or develop a patient care plan, implement the plan and follow-up on intended and non-intended outcomes.
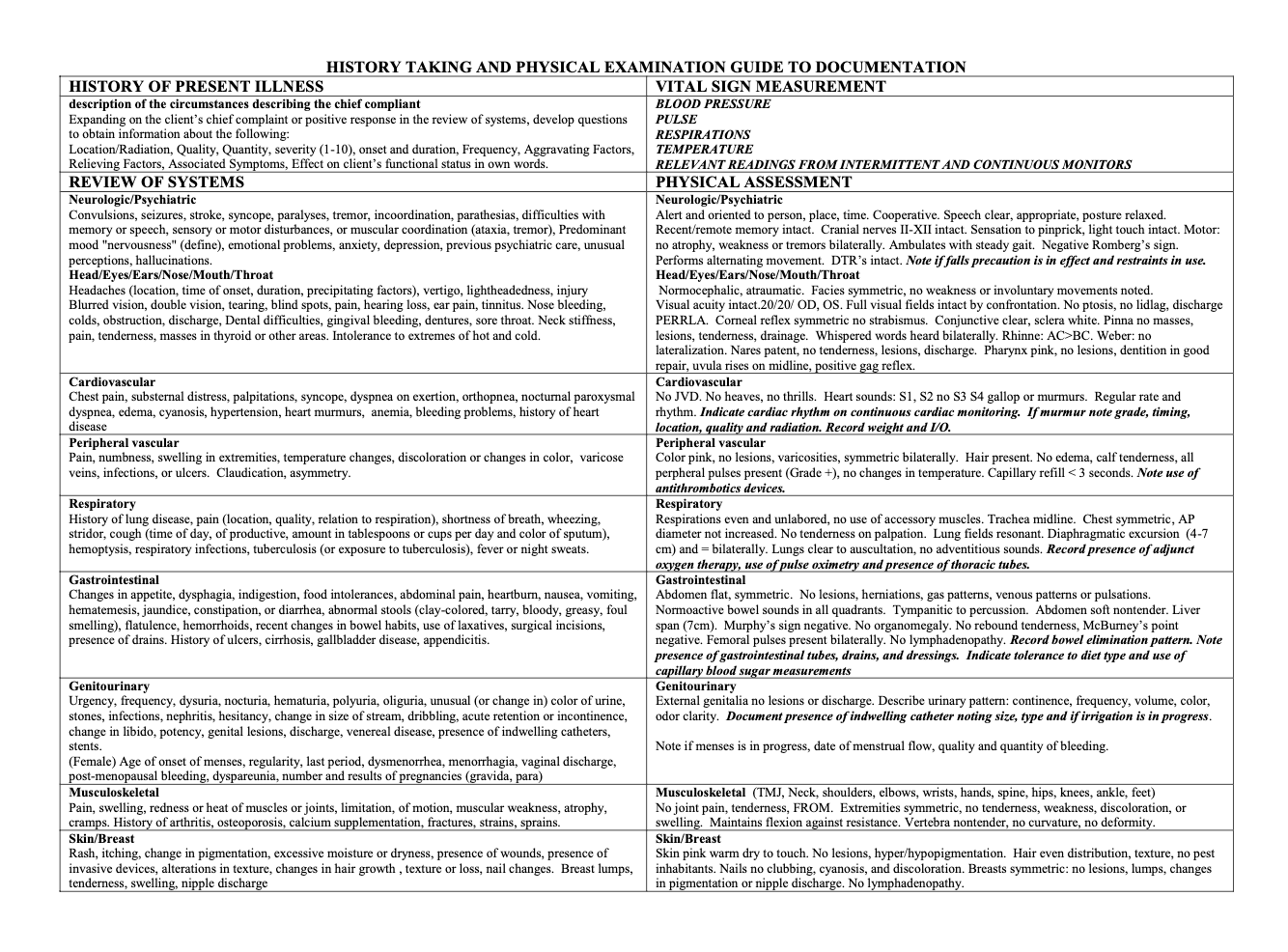
An important subjective skill is the ability to conduct a review of systems. A ROS is an inventory of the body systems that is obtained through a series of questions in order to identify signs and/or symptoms which the patient may be experiencing. The Centers for Medicare and Medicaid Services (CMS) recognizes 14 systems:1 Constitutional symptoms (i.e. fever, weight loss, vital signs); eyes; ears, nose, mouth, throat; cardiovascular; respiratory; gastrointestinal; genitourinary; musculoskeletal; integumentary; neurological; psychiatric; endocrine; hematologic/lymphatic; and allergic/immunologic. (See Figure 1) The ROS serves as a guide to help identify potential or underlying illnesses or disease states subjectively, thus allowing the pharmacist to prioritize systems for follow up in the objective examination. The ROS can also help the provider obtain information about a chief concern as well as the history of present illness.
Next is the physical examination, the critical objective component of the patient care process patient gathering process. A physical examination helps you as the pharmacist to determine the general status of the patient’s health. The exam also gives you a chance to talk to the patient about any ongoing pain or symptoms that they are experiencing or any other health concerns that the patient might have.2 The physical exam can be focused or complete based on the presentation of the patient.
In 2014 I asked the following question. Is the pharmacy profession really ready for provider status? My answer is probably not. Why? Because the pharmacy profession is not ready to take on ALL three pillars of provider status. Every provider profession has incorporated the three critical components into their practice model of patient care. First, each profession makes an assessment of the patient, most by conducting a physical examination, although sometimes the exam is limited to the complaint and signs and symptoms of the patient presentation. Nonetheless, a physical assessment is conducted. Second, each profession diagnoses the patient problem. Then, a treatment plan is discussed with the patient and implemented.
The COVID-19 pandemic has opened the realization door that the pharmacy profession still has not made substantial progress to meeting the 3 pillars of provider status, thus providing patients, the health care system, and the federal government the skill set necessary to be a called a provider. We must change the way we educate our students, the way we practice, thus providing a platform that every profession uses to advocate for the provider status.
Mark A. Munger, PharmD, FCCP, FACC, is a professor of pharmacotherapy and adjunct professor of internal medicine, at the University of Utah, where he also serves as the associate dean of Academic Affairs for the College of Pharmacy.
References:
- Review of Systems. https://www.acc.org/tools-and-practice-support/practice-solutions/coding-and-reimbursement/documentation/evaluation-and-management/review-of-systems Accessed 04/2020.
- The Physical Examination. https://www.healthline.com/health/physical-examination Accessed 04/2020.
Figure 1: (History Taking and Physical Examination Guide to Documentation [includes ROS])
Click on the figure to enlarge