Using High-Fidelity Simulation To Improve Teamwork and Clinical Metrics During Procedural Emergencies
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Cath Lab Digest or HMP Global, their employees, and affiliates.
Belen Camacho, DNP, RN, NEA-BC, CV-BC, RCIS1; Sally O. Gerard, DNP, RN, CDCES2
1Director, Clinical Operations (Cardiac Catheterization, Electrophysiology, Structural Heart), Stamford Health, Stamford, Connecticut; Adjunct Faculty, Fairfield University, Fairfield, Connecticut
2Associate Dean of Graduate Studies and Professor, Nursing, Fairfield University, Fairfield, Connecticut
Belen Camacho, DNP, RN, NEA-BC, CV-BC, RCIS, can be contacted at bcamacho@stamhealth.org.
Dr. Sally Gerard DNP, RN, CDCES, can be contacted at sgerard@fairfield.edu.
Abstract
High-fidelity simulation for clinical emergencies can improve clinical skills and teamwork.1-4 Improvement of technical skills such as defibrillation and CPR competence were found after simulation.1,2,4 In an acute care hospital, procedural areas have a low volume of emergencies that occur in high-risk situations. One cardiac cath lab team led a project that sought to apply their standard of excellence to these infrequent events. An interdisciplinary simulation was created to replicate an emergent procedural complication. Outcome measures were teamwork and American Heart Association clinical metrics. This quasi-experimental pre-post-test study used the Mayo High-Performance Teamwork Scale during procedural emergencies using high-fidelity simulation. The sample of 43 respondents were matched across pre versus post survey and included 5 disciplines with the most respondents as registered nurses (n=27). Non-parametric tests for analysis using statistical software were used. Statistical significance was found in all questions resulting in a perceived improvement in teamwork. Comparison of the means for intervention-timed clinical metrics did not show statistical significance; however, overall times improved. Outcomes from the experience found with proper coordination, high-fidelity simulation can be valuable to improve teamwork for procedural emergencies. Team feedback was very positive and the intervention was added as an annual competency training.
Introduction
Simulation has been studied in-depth amongst nursing students, but for high-fidelity simulation, there is limited published outcomes for experienced healthcare professionals working in teams. Studies have found high-fidelity simulation for clinical emergencies can improve clinical skills and teamwork.1,2,4 A common scenario for high-fidelity simulation involves emergency resuscitation, which has been reported to support improvement of technical clinical skills such as defibrillation, interventions to support circulation, and CPR competence.1,2,4 Simulation has also supported improved teamwork after conducting high-fidelity clinical emergency scenarios.1,3,4 However, the existing literature does not address the complexity of a procedural area such as a cath lab, nor the skills necessary for successful outcomes in this environment. The purpose of this study was to evaluate the impact of high-fidelity simulation in a procedural emergency in the cath lab to assess the impact on teamwork and clinical outcomes.
Description of the Problem

The hospital where the study took place has a low volume of intra-procedure emergencies in high-risk situations within the hospital’s procedural areas. For members of the healthcare team, there are limited opportunities to practice these skills together. Emergencies in this area include but are not limited to cardiac arrest, hemorrhage, and open chest interventions. In the procedural area, if there is a cardiac arrest, the “emergency team” will arrive to assist with stabilizing the patient. Often the procedural team assembled is quite large and the additional members can add to the chaos. During multidisciplinary cases, for example, transcatheter aortic valve repair, team members may include but are not limited to an interventional cardiologist, cardiac cath registered nurse (RN), cardiovascular technologists, operating room RN, perfusionist, cardiac physician’s assistant (PA), echocardiographer, and more. Ideally, the procedure or operation should, if possible, be completed before leaving the room. The sheer volume of clinicians and intensity of the emergency support inspired the project concept. The study was based on the idea that a multidisciplinary team skilled in intra-procedural emergencies that practices with high-fidelity simulation will experience improved skills and teamwork.
Literature Review
In a literature review of high-fidelity simulation for emergency teams, some themes emerged.
A literature review of databases CINAHL and PubMed (1985-2022) for English language results produced 376 records with keywords “nurse,” “nurses,” or “nursing”; “team”, and “emergencies”. Studies focused on emergencies in the acute care settings; literature reviewed included many that involved students.
Publications supported the idea that HF simulation for clinical emergencies can improve clinical skills and teamwork.1,2,4 Improvement of technical clinical skills such as defibrillation, interventions to support circulation, and CPR competence were found after simulation.1,2,4 Simulation has also supported improved teamwork after conducting high-fidelity clinical emergencies.1,3,4 Overall, the literature had few interdisciplinary teams but many examples of student simulations.
The literature also supports the specific training of teams for clinical situations. Using team training can be an effective method to improve healthcare personnel’s teamwork competencies.5 Using high-fidelity simulation can also improve the performance of interprofessional healthcare teams in an operating room setting.6 Overall, the evidence supported the concept of high-fidelity simulation with an interdisciplinary procedural team, yet most studies lack the complexity of procedural-specific emergencies.
Project Methods
Overall Design. This quasi-experimental, pretest–posttest study assessed teamwork during procedural emergencies using high-fidelity simulation. Simulations were conducted across four procedural areas in the hospital: the Cardiac Catheterization Lab, HSS Operating Room, Interventional Radiology, and Non-Invasive Cardiology. The project team included additional sites to study the impact across varied procedural areas. Simulations were conducted for all staff.
Participants who volunteered to participate in the project completed pre- and post-tests using the Mayo High-Performance Teamwork Scale (MHPTS). The MHPTS includes 16 questions and has been shown to provide reliability and consistency in rating key behaviors of high-performance teams.7 Interventions for clinical metrics based on American Heart Association guidelines were observed and measured in minutes. Data were collected by trained volunteers observing the simulations. Non-parametric tests for analysis using statistical software were used.
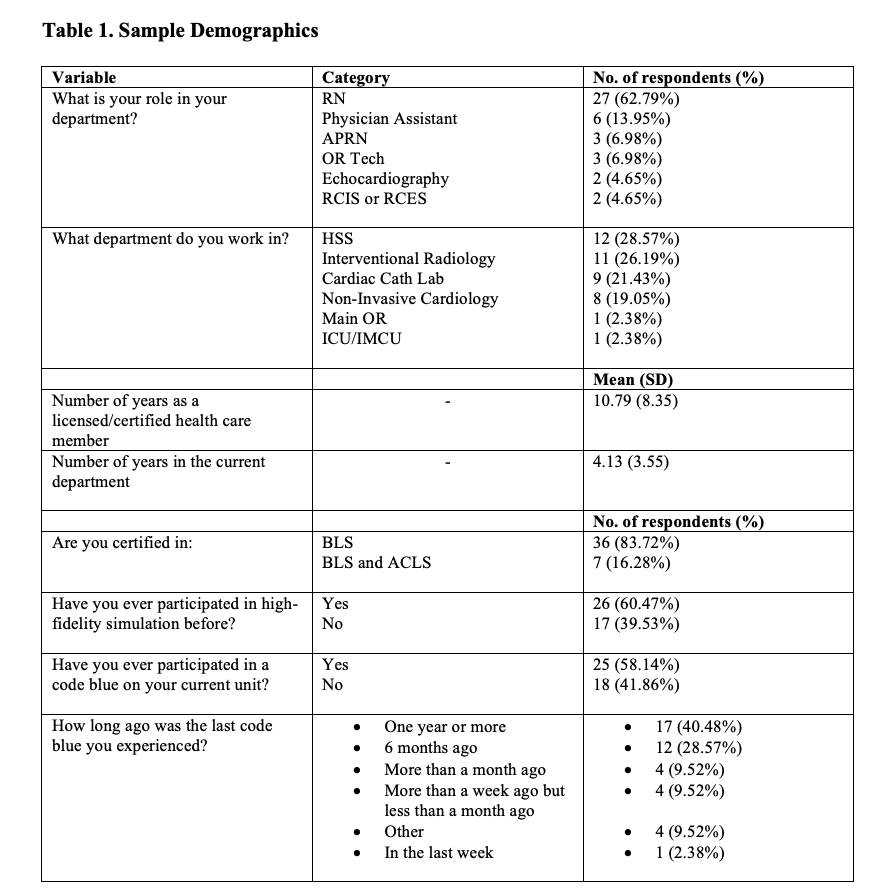
Sample and Sampling Technique. A convenience sample of multidisciplinary staff members from four procedural areas of the community hospital was included. Participants included nurses, technologists, and advanced practice practitioners. A non-participant trained observer documented time intervals for interventions during the simulation (Table 1).
Protection of Participants’ Rights (IRB). The project was deemed exempt by Institutional Review Board (IRB) of the institution.
Data Collection. Data collection included an online survey administered pre- and post-simulation using the MHPTS; completion of the data was voluntary. Timed interventions were documented by a trained observer using video analysis of interventions completed during the simulation.
The primary investigator explained the research project, the voluntary nature of the data collection portion, and that participants could withdraw at any time. Participants scanned a QR code before participating, and consent was obtained before seeing the pre-test and posttest questionnaires. The survey was de-identified but available to link pre- and post-test data using a keycode that cannot be linked back to the participant. Participants completed the demographic questionnaire included in the survey in both the pre- and post-questionnaires to aid in matching surveys. Video recording was part of the simulation activity and is part of the hospital’s continuing education training.
Results
A total of 43 respondents were matched across pre versus post survey and were included in the analysis (Table 1). The largest sample of respondents were RNs (n=27, 62.79%), followed by physician assistants (n=6, 13.95%). The average number of years as a licensed healthcare professional among the participants was 11 years, with an average number of years in the current department of 4 years. Eighty-four percent (84%) of the participants were certified in basic life support (BLS), while 16% were certified in BLS and advanced cardiac life support (ACLS). Twenty-six (26) participants (60%) had participated in high-fidelity simulation before, 25 participants (58%) had experienced a code blue on their current unit, and 17 (40%) said their last code blue experience had been one year or more prior.
A comparison of survey responses was measured by the MHPTS across pre versus post survey:
• Recognition of a leader (by all team members):
- Pre: 51% “consistently”
- Post: 91% “consistently”
- P<.0001
• Team leader maintains balance between command authority and team member participation:
- Pre: 46% “consistently”
- Post: 93% “consistently”
- P<.0001
• Clear understanding of each team member role:
- Pre: 39% “consistently”
- Post: 79% “consistently”
- P=.0003
• Team prompted each other to attend to all significant clinical indicators:
- Pre: 56% “consistently”
- Post: 86% “consistently”
- P=.0025
• Consistent verbalization of activities:
- Pre: 56% “consistently”
- Post: 95% “consistently”
- P<.0001
• Team members paraphrase instructions:
- Pre: 46% “consistently”
- Post: 88% “consistently”
- P≤.0001
• Team members referred to established protocols for the procedure:
- Pre: 56% “consistently”
- Post: 81% “consistently”
- P=.001
• All team members were appropriately involved in the activity:
- Pre: 67% “consistently”
- Post: 93% “consistently”
- P=.004
Wilcoxon rank-sum test (non-parametric statistical testing using matched pair samples) was conducted to compare pre and post test results, and determine whether self-reported perceptions of teamwork improved after high-fidelity simulation. Significant differences were found in all 16 items on the MHPTS across pre and post survey, with values of P<.05.
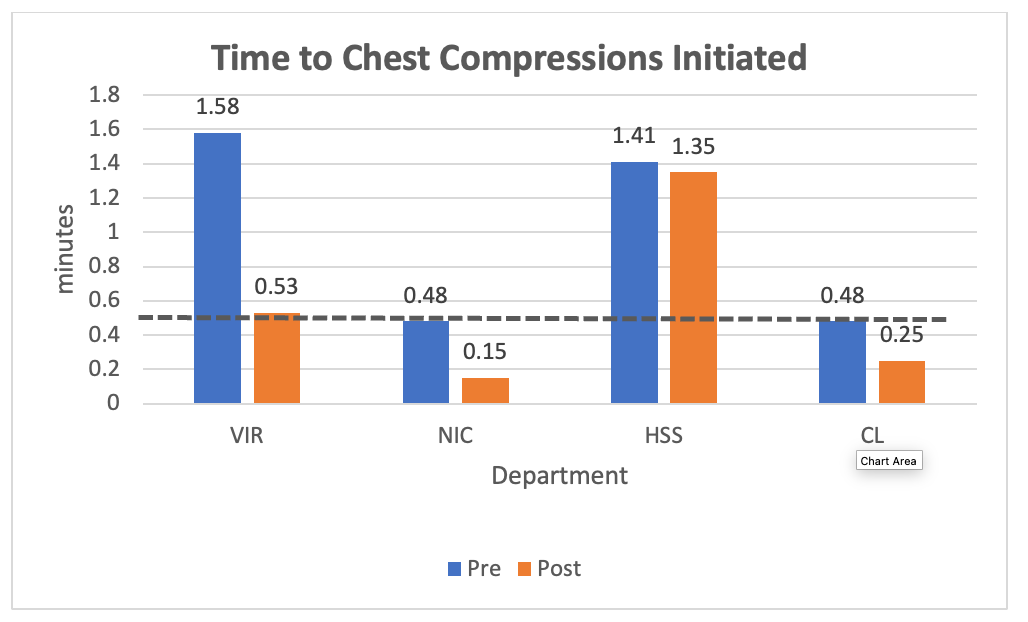
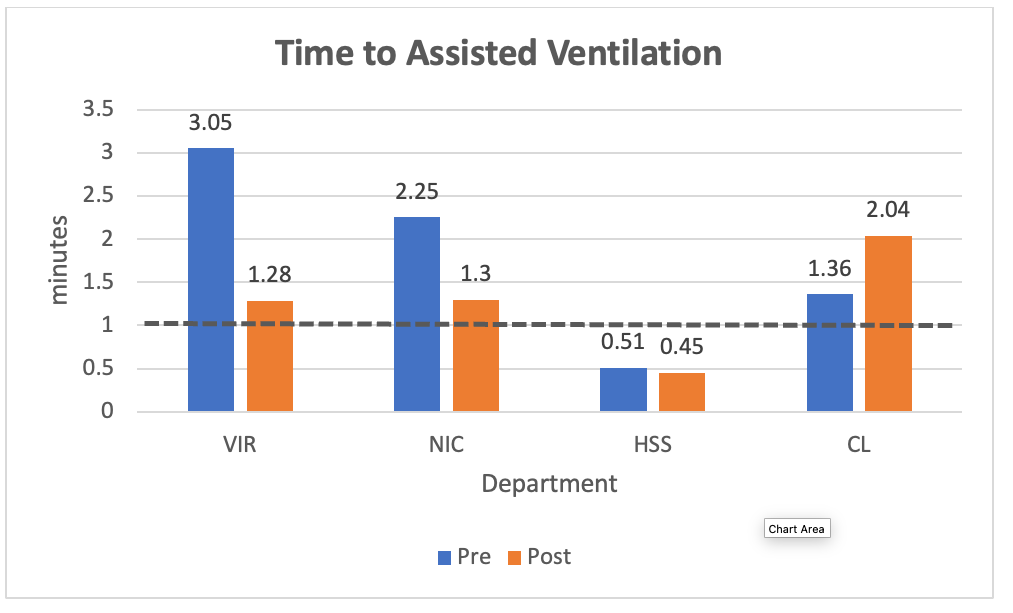
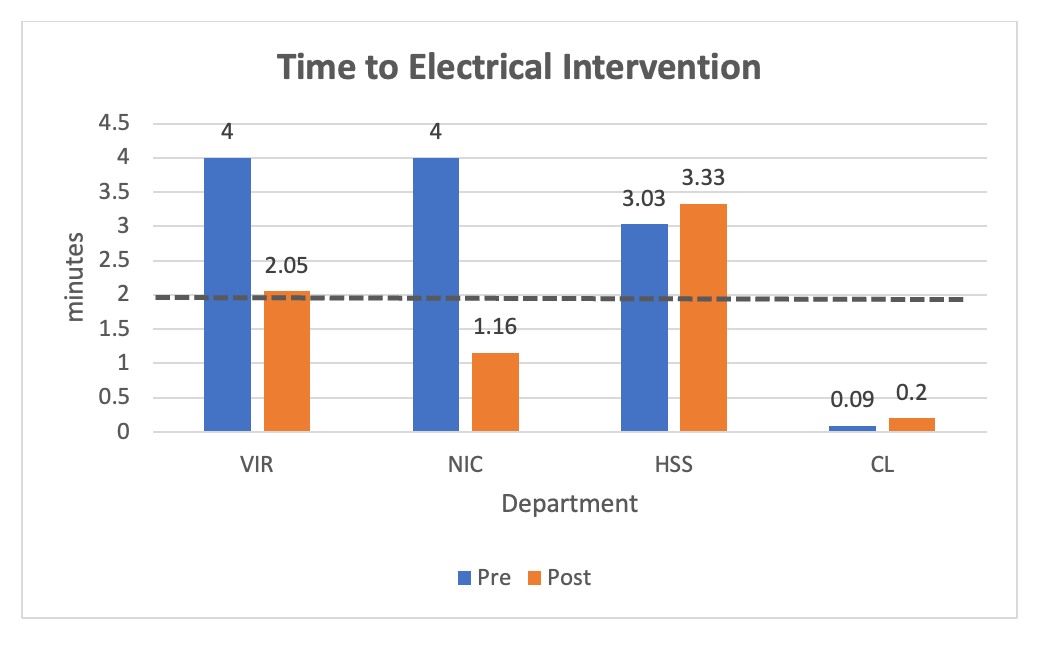
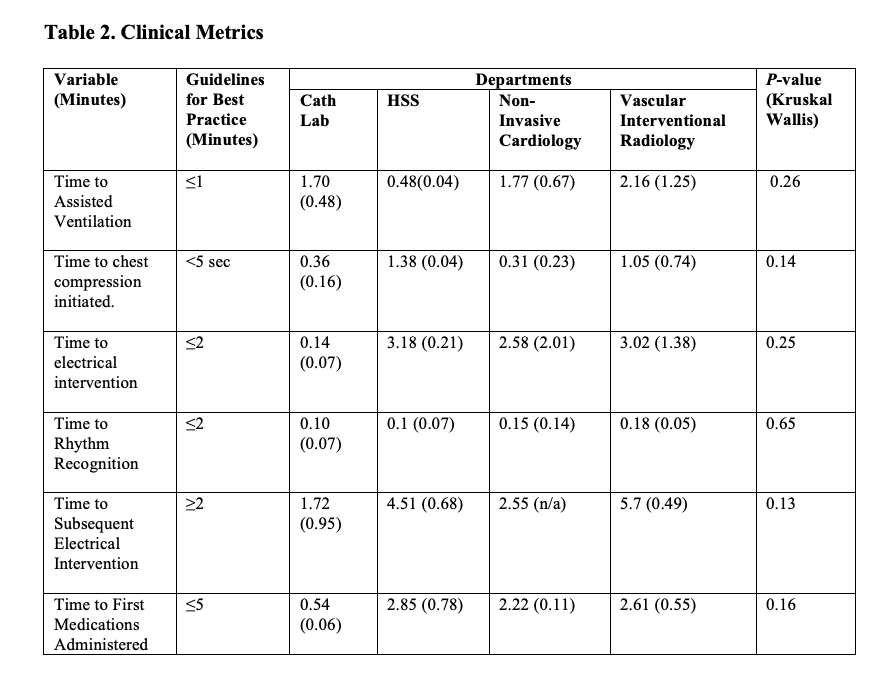
The overall mean comparison of time variables among all the departments that performed simulation showed no significant differences were found for “time to chest compression” (Figure 1), “time to assisted ventilation” (Figure 2), “time to electrical intervention” (Figure 3), “time to rhythm recognition” (Table 2), “time to subsequent electrical intervention” (Table 2), and “time to first medication” (Table 2). There were improvements in “time to compressions initiated” from the first simulation to the second simulation in each department (Table 2).
Discussion
Based on established evidence, the results of the simulation for the departments were expected to improve perceptions of teamwork.1-4 Significant differences were found in all 16 items on the MHPTS across pre and post survey, with P values of <.05.
These outcomes were noted not only in the teamwork assessment, but also in informal staff responses. Having the opportunity to have the full team present for a simulated emergency was a heavy lift, but proved to the team to be well worth the efforts. These emergencies had been a source of significant concern for departments that collectively strive for exceptional patient outcomes. The team felt more prepared, and welcomed the opportunity to address questions and concerns in the debriefing. Due to the intensity of these emergencies in actual practice, there is not the opportunity for such real-time learning.
The clinical metrics for the units were strong but had opportunities for improvement. The timed clinical metrics for the departments improved on the second simulation for some, but not all. This data could be used following the project for specific training needs of individual procedural units. Limitations of the pilot included a single-site project and small convenience sample size. The benefit was that it reflected needs of the organization that could be used for clinical development.
Despite intense effort involved in piloting these simulations, the journey was beneficial to the team. There was a total of 43 participants in the simulation. Challenges included scheduling and protected time for experienced healthcare providers. The physicians were not included in the survey; however, there were at least 8 physician team leaders involved with anesthesia support. The team felt the participation of the medical professionals was vital for realistic experiences. In planning, the team did not have strong buy-in from the physicians and although the physicians were included in the simulations, their participation was not deemed essential to the project. Despite this structure, physicians did embrace the procedural simulation emergency training and had very positive feedback. Discussion during debriefs included positive comments regarding practice amongst experienced healthcare professionals. The interdisciplinary dialogue of the debrief was beneficial and educational.
Staff reactions to simulation were extremely positive with requests for more training in the future. Based on the metrics and the feedback of participants, department leaders were able to advocate for resources to support integrating high-fidelity simulation into annual competencies.
There were varied lessons from this project. A collective planning meeting with the varied stakeholders would have been very helpful. Unfortunately, in the planning phase, prior to the demonstration of value around this project, the interest did not extend outside of nursing. In terms of post-simulation data evaluation, it would have been valuable to have a second phase of data after the units had an actual procedural emergency to evaluate the translation of skills to real-life situations. Considering the infrequency of these events, it would have been logistically difficult, but valuable. This issue came to life after the project when one of the project sites experienced a serious complication that required the highest level of team intervention. Not only did the patient have a very positive outcome, but the team also immediately shared with leadership their perception of the training as the difference in the cohesive and calm approach to the situation.
Conclusion
Procedure emergencies are a high-risk, low-volume occurrence. The residual effects of real emergencies are impactful to highly skilled staff when the response is not optimal. High-fidelity stimulation can be used to improve teamwork for procedural emergencies. Using this training where high-risk, low-volume emergencies occur was found to have many benefits and has been included in annual training for experienced healthcare workers. High-fidelity simulations have supported clinical improvement in a variety of settings but much of the nursing literature involves students. More information is needed to standardize high-fidelity simulations that have supported clinical improvement in a variety of settings.1-4 Intra-procedural use of high-fidelity simulations has not been described in the literature.
The resources for high-fidelity simulations are significant, but data to support improved clinical outcomes supports the training of acute care leaders to provide education and the staff time to participate.
Acknowledgments
Executive Director of Research Suzanne Rose, MS, PhD; Research Statistician Shweta Karki, MPH; Simulation Manager Michelle Saglimbene, DNP, RN, and Fairfield University.
References
1. Gordon CJ, Buckley T. The effect of high-fidelity simulation training on medical-surgical graduate nurses' perceived ability to respond to patient clinical emergencies. J Contin Educ Nurs. 2009 Nov; 40(11): 491-498; quiz 499-500. doi:10.3928/00220124-20091023-06
2. Ali AA, Miller E, Musallam E, Ballman K. Acute care nurse practitioner students' perceptions of a debriefing experience after a cardiac emergency high-fidelity simulation: a qualitative study. AACN Adv Crit Care. 2021 Sep 15; 32(3): 264-274. doi:10.4037/aacnacc2021376
3. Hibberson M, Lawton J, Whitehead D. Multidisciplinary simulation training for perioperative teams: An integrative review. Journal of Perioperative Nursing. 2021;34(2):3-13, s1-s9. https://doi.org/10.26550/2209-1092.1111
4. Laco RB, Stuart WP. Simulation-based training program to improve cardiopulmonary resuscitation and teamwork skills for the urgent care clinic staff. Mil Med. 2022 May 3; 187(5-6): e764-e769. doi:10.1093/milmed/usab198
5. Aaberg OR, Hall-Lord ML, Husebø SIE, Ballangrud R. A complex teamwork intervention in a surgical ward in Norway. BMC Res Notes. 2019 Sep 14; 12(1): 582. doi:10.1186/s13104-019-4619-z
6. Leithead J 3rd, Garbee DD, Yu Q, et al. Examining interprofessional learning perceptions among students in a simulation-based operating room team training experience. J Interprof Care. 2019 Jan-Feb; 33(1): 26-31. doi:10.1080/13561820.2018.1513464
7. Malec JF, Torsher LC, Dunn WF, et al. The Mayo high performance teamwork scale: reliability and validity for evaluating key crew resource management skills. Simul Healthc. 2007 Spring; 2(1): 4-10. doi:10.1097/SIH.0b013e31802b68ee
Sources
Franklin AE, Burns P, Lee CS. Psychometric testing on the NLN Student Satisfaction and Self-Confidence in Learning, Simulation Design Scale, and Educational Practices Questionnaire using a sample of pre-licensure novice nurses. Nurse Educ Today. 2014 Oct; 34(10): 1298-1304. doi:10.1016/j.nedt.2014.06.011
Sewchuk DH. Experiential learning--a theoretical framework for perioperative education. AORN J. 2005 Jun;81(6): 1311-1318. doi:10.1016/s0001-2092(06)60396-7.
Sugarman L. [Review of Experiential Learning: Experience as the Source of Learning and Development, by D. A. Kolb]. Journal of Occupational Behavior. 1987; 8(4), 359-360. http://www.jstor.org/stable/3000261
Thompson Bastin ML, Cook AM, Flannery AH. Use of simulation training to prepare pharmacy residents for medical emergencies. Am J Health Syst Pharm. 2017 Mar 15; 74(6): 424-429. doi:10.2146/ajhp160129
Experiential Learning. Institute for Teaching and Learning Innovation. The University of Queensland. Accessed April 6, 2026. https://itali.uq.edu.au/teaching-guidance/teaching-practices/active-learning/experiential-learning
Van Wyk C. Exploring the effects of climate change communication and training efforts: Lessons from training courses aimed at mid-career professionals. 2017. University of Cape Town. Accessed April 6, 2026. https://www.researchgate.net/figure/Kolbs-experiential-learning-theory-states-that-effective-learning-takes-place-when-a_fig1_317689748
Wigginton JG, Agarwal S, Bartos JA, et al. Part 9: Adult Advanced Life Support: 2025 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2025 Oct 21; 152(16_suppl_2): S538-S577. doi:10.1161/CIR.0000000000001376