The First Dorsal Metatarsal Artery “Kite” Flap: A Case Report
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of ePlasty or HMP Global, their employees, and affiliates.
Abstract
Soft tissue coverage of the lower extremity and foot is challenging due to limited tissue reach and high functional demand. The hand, in contrast, is rich with reconstructive options that may be translated to the foot because of its analogous structure. A workhorse flap in the hand is the first dorsal metacarpal artery “kite” flap; however, the analogous first dorsal metatarsal artery flap is rarely described. We present a case of successful use of the first dorsal metatarsal artery flap for reconstruction of a soft tissue defect overlying the dorsal left metatarsophalangeal joint. This flap has proved useful as a local tissue option for the distal, dorsal foot, and its indications may be expanded similarly to those of the first dorsal metacarpal artery flap in the hand.
Introduction
Soft tissue coverage of the lower extremity and foot is challenging because local reconstructive options are hindered by limited tissue reach and high functional demand.1 In contrast, there are many local flaps described for soft tissue coverage of the hand and upper extremity.2 A workhorse flap for the radial region of the hand is the first dorsal metacarpal artery (FDMcA) perforator flap. It is a powerful tool for reconstruction of the dorsal thumb and metacarpals and is often preferred for its reliable blood supply and sensate coverage.2 Because the hand and foot share analogous structures, the FDMcA flap can be translated to the foot for reconstructive purposes. The first dorsal metatarsal artery (FDMtA) flap has been published a handful of times in the literature for traumatic indications.3,4 This report presents a successful case of the FDMtA flap to reconstruct a defect over the first metatarsophalangeal joint following soft tissue necrosis after intra-articular corticosteroid injection.
Case Presentation
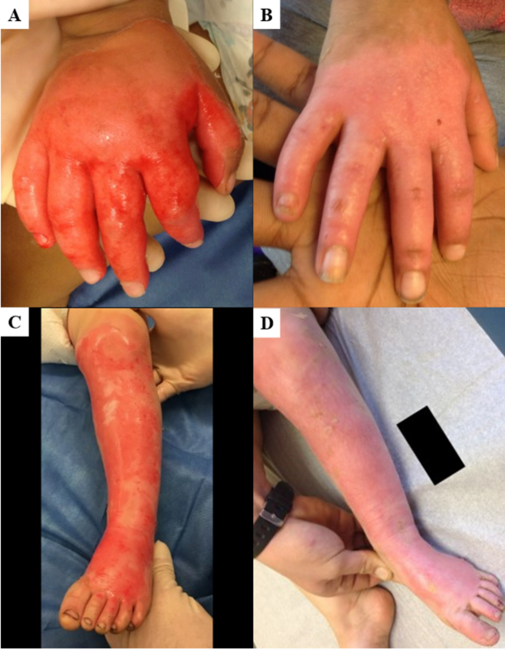
A 73-year-old nonsmoking female with a history of Raynaud phenomenon presented to the clinic with a chronic nonhealing wound overlying the left dorsal first metatarsophalangeal joint (MTPJ). Six months prior to presentation, the patient received multiple corticosteroid injections into the joint for osteoarthritis, which resulted in ulceration and dermal necrosis complicated by a pseudomonal infection. On physical examination she was found to have a 2 × 2-cm defect over the first MTPJ with exposed joint capsule, threatening the integrity of the great toe. The patient was referred to the plastic surgery practice for flap coverage; the surgical team determined that the case was an excellent indication for use of the FDMtA flap.
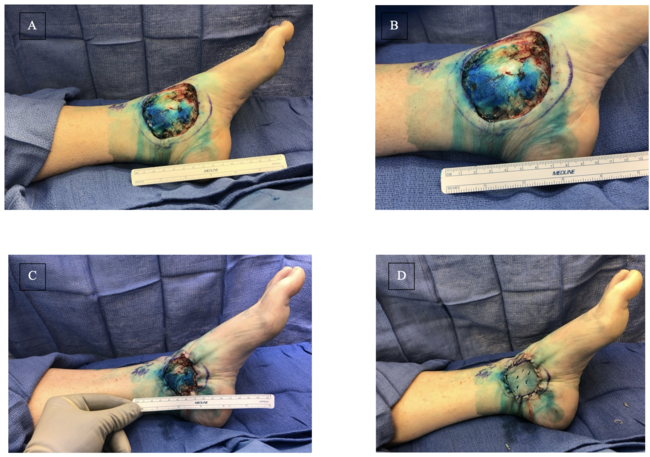
The patient was brought to the operating room, and the course of the FDMtA was confirmed using Doppler ultrasound. A 2 × 2-cm fasciocutaneous flap was fashioned and centered over a robust perforator (Figures 1 and 2). The flap was raised in a distal-to-proximal fashion, mobilizing the FDMtA, the deep plantar artery, and the dorsalis pedis artery (DPA) from which they both originate. Preserving the deep plantar artery, the distal end of the FDMtA was ligated. The flap achieved reach to the distomedial border of the defect via a combination of medial rotation and 1.5 cm of advancement, and the flap was inset to the surrounding skin. Good Doppler flow was confirmed following inset to ensure flap viability. The donor site deficit was covered with a dermal skin substitute and similarly secured to the surrounding skin (Figure 3).
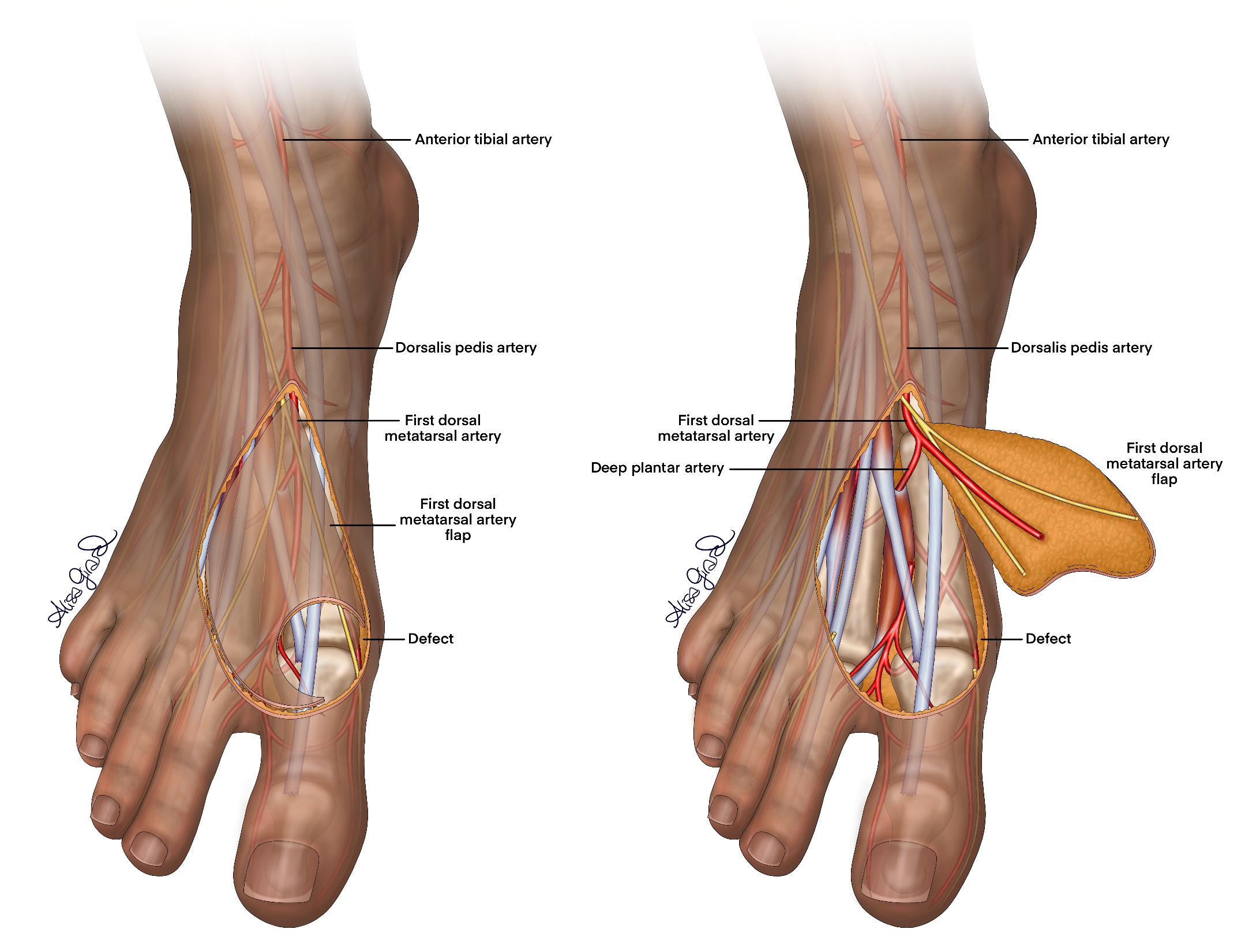
Figure 1. Anatomical illustration of the first dorsal metatarsal artery flap.

Figure 2. Elevated first dorsal metatarsal artery flap.

Figure 3. Flap inset over the first dorsal metatarsal phalangeal joint with acellular dermal matrix applied over the donor site.
There were no postoperative complications other than a superficial surgical site infection that resolved with a short course of antibiotics.
The patient returned to the operating room 8 weeks after the index procedure for planned skin grafting of the donor site deficit, which healed unremarkably, completing a successful reconstruction of the patient’s foot (Figure 4).

Figure 4. Dorsal foot at 3 months after FDMtA flap and 1 month after split-thickness skin graft.
Discussion
The first dorsal metacarpal artery “kite” flap was first described in 1979 to treat cutaneous ulcers on the dorsal thumb.5 This flap is typically raised on the ulnar branch of the FDMcA, which arises from the radial artery, where it ends as an arterial plexus over the dorsum of the index finger. We describe a successful 2-stage approach to adapt the “kite” flap for reconstruction of a defect overlying the dorsal MTPJ. The DPA divides into the FDMtA and the deep plantar artery between the first and second metatarsals. The proximally based FDMtA flap is therefore distinguished from the DPA flap by the preservation of the deep plantar artery.6 FDMtA flaps have been reported infrequently in the literature, most often for patients suffering from burns or trauma to the foot,3, 7 often in a reverse fashion from a distally-based pedicle.3, 8 In the current case, a reverse flap would have required substantial rotation of a small-caliber pedicle located near the region of prior steroid-induced soft tissue necrosis and infection. An anterograde flap was instead favored for its pedicle outside the zone of injury and the short distance of rotation and advancement needed to cover a small, immediately adjacent wound.
The FDMtA flap offers several advantages, including a dependable vascular supply, minimal donor site morbidity, and positive aesthetic outcomes due to the similarity of donor site skin. One caveat is that the viability of the FDMtA flap can be compromised during transposition due to its variable vascular anatomy.1 Thus, surgeons must carefully assess present vascular patterns when designing each flap and center the skin paddle over a robust perforator.
Conclusions
We present a case of an adapted “kite” flap based on the first dorsal metatarsal artery as an acceptable choice for coverage of a defect of the dorsal great toe in a patient with a history of complicated wound healing. This flap has proved useful as a local tissue option for the distal dorsal foot, and its indications may be expanded analogously to the first dorsal metacarpal artery flap in the hand.
Acknowledgments
Authors: Sophia Chryssofos, BS1; Alisa O. Girard, MS, MD2; Michael Arthur, MD, DPM, PhD3; Alec Fisher, MD2; David Millili, DPM3; Jordan Fishman, MD2
Affiliations: 1Cooper Medical School of Rowan University, Camden, New Jersey; 2Cooper University Hospital, Division of Plastic & Reconstructive Surgery, Camden, New Jersey; 3Cooper University Hospital, Department of Podiatry, Camden, New Jersey
Correspondence: Alisa Girard, MD; girard-alisa@cooperhealth.edu
Ethics: The institution’s IRB determined the study exempt from review. Written informed consent was obtained for publication of the case details and images.
Funding: The authors received no financial support for this work.
Disclosures: The authors disclose no relevant financial or nonfinancial interests.
References
- Hallock GG. The first dorsal metatarsal artery perforator propeller flap. Ann Plast Surg. 2016;76(6):684-687. doi:10.1097/SAP.0000000000000264
- Wink JD, Gandhi RA, Ashley B, Levin LS. Flap reconstruction of the hand. Plast Reconstr Surg. 2020;145(1):172e-183e. doi:10.1097/PRS.0000000000006311
- Khan W, Loh CYY, Gkorgkolis V, El-Muttardi N. Dorsal metatarsal artery perforator (DMtAP) flap reconstruction of the foot: a review. JPRAS Open. 2020;26:37-42. doi:10.1016/j.jpra.2020.09.002
- Vazales R, Masadeh S. First dorsal metatarsal artery flap for coverage of soft tissue defects of the distal foot: delayed technique, proximal- and distally based fasciocutaneous and adipofascial variants. Clin Podiatr Med Surg. 2020;37(4):765-773. doi:10.1016/j.cpm.2020.07.001
- Foucher G, Braun JB. A new island flap transfer from the dorsum of the index to the thumb. Plast Reconstr Surg. 1979;63(3):344-349. doi:10.1097/00006534-197903000-00008
- Saboye M, Majchrzak A, d’Andréa G, Bronsard N, Camuzard O, Lupon E. The first dorsal metatarsal artery perforator flap: a description and anatomical study. J Clin Med. 2025;14(12):4136. doi:10.3390/jcm14124136
- Godwin Y, Wadi M, Harb L, et al. Dorsal metatarsal artery perforator flaps (DMTAPF) applied for paediatric foot reconstruction: a review of the aetiology of primary injury, surgical technique applied, and long-term outcome for the child. J Plast Reconstr Aesthet Surg. 2024;99:619-627. doi:10.1016/j.bjps.2024.05.025
- Bharathwaj VS, Quaba AA. The distally based islanded dorsal foot flap. Br J Plast Surg. 1997;50(4):284-287. doi:10.1016/S0007-1226(97)91161-9