Reconstruction of an Upper Lip Midline Defect With Bilateral Lip Advancement Flaps
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of ePlasty or HMP Global, their employees, and affiliates.
Questions
- How is basal cell carcinoma (BCC) risk assessed and treated?
- What are the options for upper lip reconstruction?
- What are the features of the lateral lip advancement flap?
- What are the considerations for reconstructing the upper lip?
Case Description
A 90-year-old woman presented with a papule on her upper lip. She was diagnosed with basal cell carcinoma (BCC) on biopsy. An almost pigmentless papule measuring 8 x 6 mm was observed on the philtrum of her upper lip. Mohs surgery is not generally performed in Japan; instead, reconstruction is performed after resection and a negative pathological diagnosis. The tumor was excised on the orbicularis oris muscle with a 5-mm margin, and an artificial dermis was applied (Figure 1A and B). The tissues were fixed in formalin. Small cords of tumor cells had infiltrated and dissected the stroma parallel to the skin surface, which is consistent with the morphea form of BCC (Figure 2). The horizontal and deep margins were intact. The skin defect was 13 x 11 mm, and the Cupid’s bow had not been invaded. We designed a lateral lip advancement flap on both sides of the defect. In addition, we excised the skin of the paranasal wing in a "crescent" shape to promote medial extension. We also placed the incision line on the mouth side, away from the white skin roll (Figure 3A). We dissected over the nasolabial sulcus on the orbicularis oris muscle and elevated the flaps (Figure 3B). The skin was extended bilaterally and sutured (Figure 3C). One-year postoperative, excellent aesthetic and functional results were achieved (Figure 4); the suture line scar was not noticeable, and the Cupid’s bow morphology was preserved. In addition, the nasolabial sulcus was shallow postoperative because of the dissection and advancement of the flap beyond the nasolabial sulcus. We also moved the mouth-side incision line away from the white skin roll.
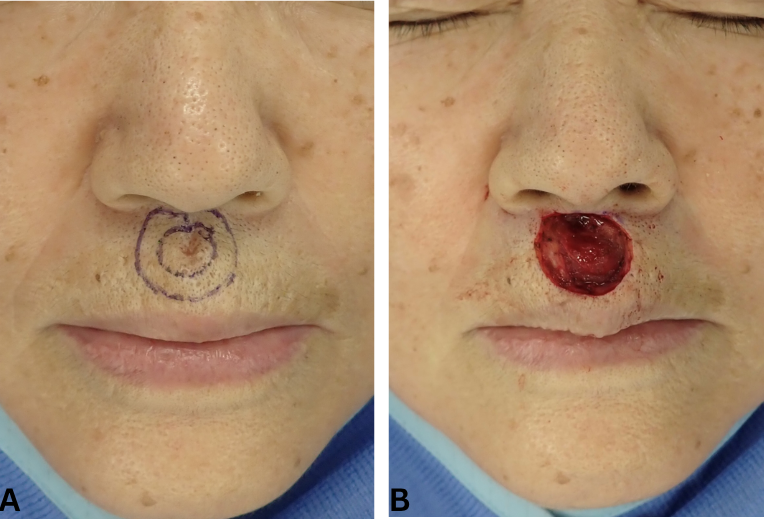
Figure 1. (A) The excision margin was set at 5 mm. (B) The tumor was excised on the orbicularis oris muscle.
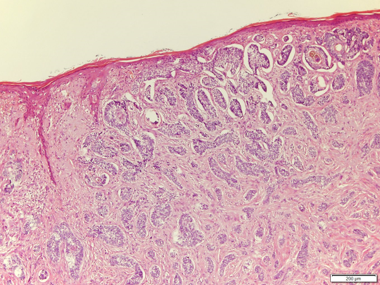
Figure 2. Small cords of tumor cells infiltrated and dissected the stroma parallel to the skin surface (hematoxylin and eosin stain).
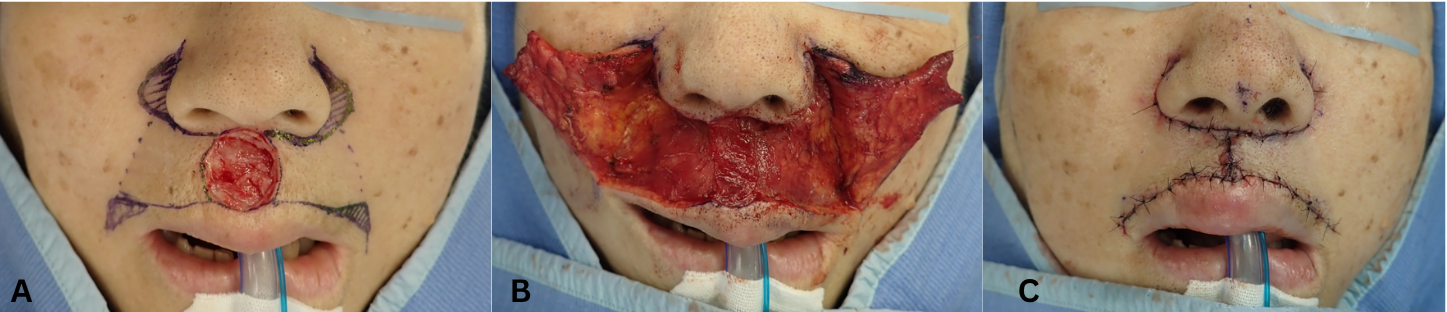
Figure 3. (A) A bilateral lip advancement flap was designed. (B) The flap was elevated over the orbicularis oris muscle and dissected beyond the nasolabial sulcus. Adjustment of the caudal of the elevated skin flap can be used to shape the Cupid's bow. We intentionally retained the skin on the caudal side of the flaps and inserted them into the lower part of the defect to maintain a Cupid's bow (yellow arrows). (C) The skin was extended bilaterally and sutured.

Figure 4. One-year postoperative.
Q1. How is BCC risk assessed and treated?
The patients at high risk of BCC have the following risk factors: involvement of the head, neck, hands, and feet; tumor size of greater than 2 cm; recurrent cases; and pathologically aggressive growth patterns (such as micronodular and morpheaform). Morpheaform, a rare infiltrative type, may present as a flat, slightly firm lesion without well-demarcated borders.1 Histologically, the morpheaform growth pattern shows prominent fibrosis of the surrounding dermis.
The typical treatment for BCC is a standard resection with postoperative marginal assessment because the metastatic rate of BCC is less than 0.1%.2 For high-risk BCC, a resection margin of 4 to 6 mm is recommended.3 This patient had a morpheaform pattern pathologically and was considered to be high risk. We resected the lesion with a 5-mm margin and performed postoperative marginal assessment before reconstruction.
Q2. What are the options for upper lip reconstruction?
Reconstruction methods for upper lip defects include V-to-Y advancement flap,4 para-alar flap,5 and bilateral lip advancement flaps. The V-to-Y advancement flap involves creating an island flap by making a V-shaped incision next to the tissue defect. The V-shaped flap advances by recoiling or pushing toward the recipient site rather than stretching or pulling.5 It can be elevated easily, but the entire circumference of the flap is scarred. The para-alar flap is a local skin flap taken from the paranasal wings. Scars are inconspicuous because they are aligned within the nasolabial folds. However, it is difficult to make a large flap, and the subcutaneous area is raised because of the island flap.5 In the case of a philtrum defect, it is necessary to raise the flaps from both sides. Moreover, careful manipulation is required to move it over a long distance. Bilateral lateral lip advancement flaps are appropriate for reconstructing skin defects in the midline of the upper lip.4 It is important that the aesthetic unit be considered in the flap's design.6 The upper lip has 3-dimensional (3D) structures, including the philtrum column and hollow as well as the white roll of the vermilion-cutaneous junction.7
Q3. What are the features of the lateral lip advancement flap?
The lateral lip advancement flap is a simple technique and can be performed in a short amount of time. In addition, it does not require the sacrifice of other parts of the body, unlike skin grafting. The incision lines on the nasal and oral sides follow the shape of the aesthetic unit, so the scar is not noticeable. The incision line can be extended to compensate for the advancement of the local skin flap. It can also create postoperative shallowness of the nasolabial sulcus in a secondary fashion if it is detached beyond the nasolabial sulcus. In the present case, there was a defect in the philtrum. Adjustment of the caudal of the elevated skin flap can be used to shape the Cupid’s bow (Figure 3B). We reconstructed the defect with bilateral lip advancement flaps. We also intentionally retained the skin on the caudal side of the flaps and inserted them into the lower part of the defect to maintain a Cupid’s bow.
Q4. What are the considerations for reconstructing the upper lip?
In upper lip reconstruction, it is important to maintain the aesthetic unit, Cupid’s bow, and lip symmetry. Violating the aesthetic borders formed by aesthetic units and vermilion borders will result in noticeable deformities.8 If the white skin roll is excised, the 3D structure is lost and the lips become flat, resulting in an unnatural impression. Even if the white skin roll discrepancy is only 1 mm, it can be noticed at conversational distance.9 The white scarring of the vermilion border also stands out because of the contrast in color tone. We preserved symmetry by elevating the bilateral lip advancement flaps. The incision line was placed away from the white skin roll, and the scar was left on the white lip to prevent deformation of the white skin roll and tonal problems with the red lip. In addition, if the flap is elevated beyond the entire nasolabial fold, the nasolabial fold becomes shallower but remains in position when advanced.
A bilateral lip advancement flap is one of the appropriate reconstructive methods for upper midline lip defects.
Acknowledgments
Authors: Tomoki Himejima, MD; Michika Fukui, MD, PhD; Sakurako Kunieda, MD; Hiromu Masuoka, MD, PhD; Masakatsu Hihara, MD, PhD; Toshihito Mitsui, MD, PhD; Natsuko Kakudo, MD, PhD
Affiliation: Kansai Medical University, Department of Plastic and Reconstructive Surgery, Hirakata, Osaka, Japan.
Correspondence: Tomoki Himejima, MD, Department of Plastic and Reconstructive Surgery, Kansai Medical University, Shin-machi, Hirakata, Osaka 573-1010, Japan. E-mail: apollo.snoopy@gmail.com
Ethics: Informed written consent was obtained from the patient for the publication of this report.
Disclosures: The authors report no conflict of interest.
References
- Vincent T, Theodore S, Steven A. Cancer of the Skin. 12th ed. Wolters Kluwer; 2023: pp. 1181-1185.
- von Domarus H, Stevens PJ. Metastatic basal cell carcinoma. Report of five cases and review of 170 cases in the literature. J Am Acad Dermatol. 1984;10(6):1043-1060. doi:10.1016/s0190-9622(84)80334-5
- Quazi SJ, Aslam N, Saleem H, Rahman J, Khan S. Surgical margin of excision in basal cell carcinoma: a systematic review of literature. Cureus. 2020;12(7):e9211. doi:10.7759/cureus.9211
- Baker SR. Local Flaps in Facial Reconstruction. 4th ed. Elsevier; 2022: pp. 93-95, 737-738.
- Suzuki S. Para-alar crescentic subcutaneous pedicle flap for repair of skin defects in the philtrum. Ann Plast Surg. 1989;23(5):442-446. doi:10.1097/00000637-198911000-00012
- Luce EA. Upper lip reconstruction. Plast Reconstr Surg. 2017;140(5):999-1007. doi:10.1097/PRS.0000000000003400
- Baumann D, Robb G. Lip reconstruction. Semin Plast Surg. 2008;22(4):269-280. doi:10.1055/s-0028-1095886
- Salibian AA, Zide BM. Elegance in upper lip reconstruction. Plast Reconstr Surg. 2019;143(2):572-582. doi:10.1097/PRS.0000000000005279
- Flores RL, Zide BM. Chin IX: Unusual soft tissue problems of the lower face. Craniomaxillofac Trauma Reconstr. 2009;2(3):141-150. doi:10.1055/s-0029-1224776