

Spirituality and Aging Support Groups: A Psycho-Spiritual Intervention to Address the Mental Health Needs of Older Adults
Abstract
This article describes a support group facilitated by a chaplain and a psychotherapist at On Lok Lifeways, a comprehensive long-term health program for frail adults aged 55 and older in the San Francisco Bay Area. This spirituality and aging group has been running since 2013 with the goal of reducing depressive symptoms and enhancing the total well-being of older individuals. This paper addresses the format, content, and clinical implications of the group.
Key words: older adults, mental health, spirituality, depression, group therapy, peer support
Citation: Ann Longterm Care. 2019;27(6):e13-e18.
DOI: 10.25270/altc.2019.04.00068
Received April 13, 2018; accepted September 4, 2018. Published online April 3, 2019.
Founded in 1971, On Lok Lifeways (On Lok) is the original Program of All-inclusive Care for the Elderly (PACE).1 On Lok provides comprehensive health care services to frail older adults in the San Francisco Bay Area.2 Participants are deemed nursing-home eligible as a criterion for enrollment, yet On Lok provides extensive services enabling older adults to “age in place” or remain in their homes in the community for as long as possible. The core of the PACE model is an interdisciplinary approach to health services. An interdisciplinary team of professionals provides medical and nursing care, physical and occupational therapy, social work services, an adult day health center with daily transportation, meals, and activities, plus in-home care, home-delivered meals, medications, and other related services. In 2005, On Lok added an on-site mental and behavioral health services team and a chaplaincy department to expand its ability to meet the psychological and spiritual needs of participants.3
On Lok participants reflect the racial, ethnic, and linguistic diversity of the Bay Area. Services are provided in up to 30 different languages, which frequently requires use of professional interpreters. Partnering with family members is central to the mission of On Lok, enabling older adults to have stable foundations of care. Yet, in some cases, there is no family with which to partner, or family is estranged or conflictual. In these cases, the wrap-around network provided by On Lok is even more essential.
According to the Centers for Disease Control and Prevention, an estimated 20% of people aged 55 or older experience some type of mental health concern, such as cognitive impairment, anxiety, or mood disorders.4 The most common of these is depression. In 2002, major depression and dysthymic disorder were reported to affect between 5% and 10% of older adults in primary care.5 With demographic shifts, however, current rates are probably higher because adults between ages 50 and 64 years are nearly twice as likely to experience depression as their counterparts aged 65 and older.4 Unfortunately, depression is widely underrecognized in older adults, many of whom go untreated.4 At On Lok, Spirituality and Aging (S&A) groups have proven an effective component of depression treatment plans.
The goal of this article is to describe a helpful intervention that addresses depression, social isolation, and loneliness in older adults. This intervention, the S&A group, combines professional psychotherapy with a spiritual perspective and provides the advantages of peer support. The group can be replicated with older adults in other long-term care settings.
Spirituality and Aging Groups
To meet the needs of older adults such as Elaine (Case Vignette), On Lok’s mental health team partnered with the chaplaincy department to develop a monthly psychospiritual support group. The S&A group uses spirituality to reach out to those who otherwise might not engage in mental health services. For example, most of our S&A group participants feel isolated and/or depressed but may not readily admit to this or identify themselves as needing mental health care. As a 1999 Surgeon General report on mental health explained, “Powerful and pervasive, stigma prevents people from acknowledging their own mental health problems, much less disclosing them to others.”6 It is well-documented that stigma surrounding mental illness poses a significant barrier to accessing treatment, especially among racial and ethnic minority groups.6,7 The spirituality aspect of the S&A groups allows participants to join an activity they perceive as less stigmatizing, and possibly more rewarding, than a traditional psychotherapy group.
Spirituality and mental health often go hand in hand, especially in later life.8-12 Abundant research demonstrates the value of group psychotherapy for this population and that spiritual practice can enhance an older adult’s physical and psychological well-being.8,13-17 At On Lok, “spirituality” is nondenominational, so participants from all faiths are welcome. The goal of the S&A group is to reduce depressive symptoms in older adults by strengthening a sense of meaning and purpose, increasing self-awareness, promoting inner peace, and fostering a sense of connectedness with others. In this context, practical mental health education is provided while keeping the dignity of the “whole human being” at the forefront.
Setting
Most older adults like to receive mental health services in the same place they receive general medical care.18 S&A groups are held on-site at On Lok’s adult day health centers, where participants already spend anywhere from 1 to 5 days per week for medical care, physical therapy, and social activities. Since they are co-located with primary care, the S&A groups are easy for On Lok participants to attend, requiring no special effort to access.
The groups are co-facilitated by an On Lok chaplain and a center psychotherapist. Groups meet once per month for 1 hour. They are open groups and welcome new members at any time. In our experience, groups tend to include roughly the same 8 to 10 participants every month, along with a few new people who join from time to time. Groups run year-round; there is no designated number of sessions.
Participant Demographics
On Lok participants can be referred to the S&A group by any member of the interdisciplinary team. Typically, referrals come either from a medical provider familiar with a person’s medical and psychiatric history or from a psychotherapist, chaplain, or social worker familiar with his or her psychosocial needs. On Lok participants may also refer themselves, though it is up to the facilitators to determine their appropriateness for the group.
Reflecting the diversity of the On Lok population, attendees in the S&A group come from diverse cultural backgrounds including Caucasian, African American, Native American, Latino/a, Indian, Chinese, Vietnamese, and Filipino. For most participants, English is their first or second language. In some cases, groups have been conducted in other languages with the help of professional interpreters. Due to the complexities inherent in language interpretation and group dynamics, this tends to result in longer meetings or content that does not go quite as deep. However, even when interpreters are necessary, we have seen older adults benefit significantly from S&A group participation.
Participants’ religious affiliations have included Christian (eg, Catholic, Protestant, Evangelical), Buddhist, Hindu, Jehovah’s Witnesses, Native American spirituality, atheism, and some who identify as simply “spiritual.” Participants range in age from 57 to 98 years. Reflecting the demographics of the general older adult population, women make up about three-quarters of the group. Most attendees have at least one mental health diagnosis such as major depression, general anxiety disorder, bipolar disorder, or posttraumatic stress disorder. A few are cognitively healthy, although most have some cognitive impairment. Regardless of demographics, all attendees have diverse life histories and unique perspectives.
Content
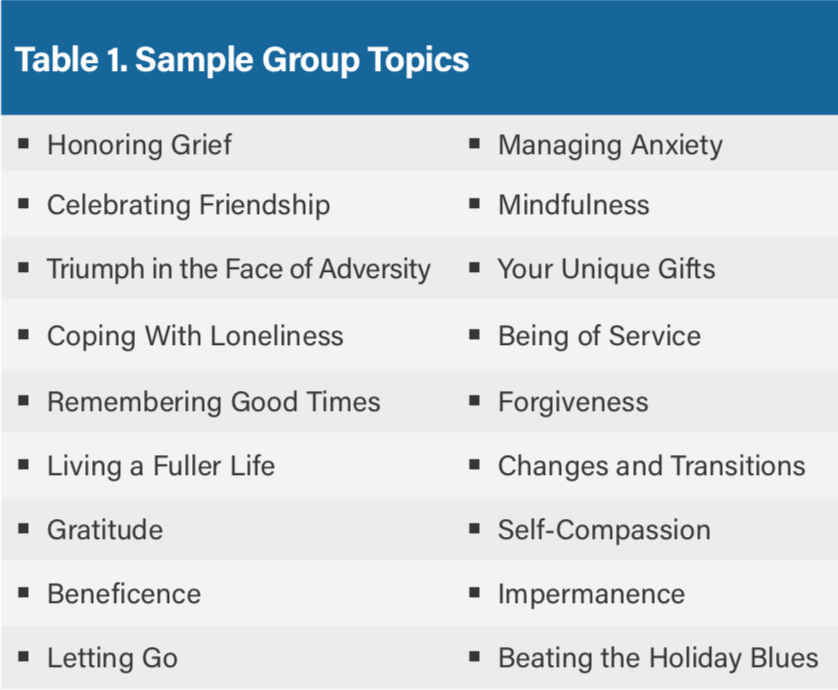
The group topic changes every month and is aimed at reducing stress and improving the ability to cope with stressful life events. Seasons and holidays often serve as inspiration. For example, spring themes may include renewal and hope. In the fall, we explore gratitude, letting go, and impermanence. During the winter, we address beating the holiday blues. Throughout the year, other topics have included honoring grief, remembering good times, forgiveness, managing anxiety, friendship, and mindfulness
(Table 1). The chaplain and psychotherapist cofacilitate every group and collaboratively decide on each month’s topic in advance, choosing the theme, selecting content to share, and agreeing on the order and flow of the group.
Topic Presentations and Group Discussion
Facilitators recognize the importance of engaging the senses to create the right mood and tone. Participants gather around a table with an artfully-crafted centerpiece related to the group’s theme. For example, a basket of flowers and fruit may represent spring. The chaplain begins by lighting a candle, gently ringing a bell, and inviting participants to join in a moment of silence. Participants are encouraged to leave everything else at the door and be fully present in the group. These rituals invoke a sacred space, lending gravity to the group process and supporting participants to feel safe in opening up.
After the silence, the psychotherapist introduces the topic and provides some psychoeducational information. If the topic is loneliness, for example, the therapist may cite statistics about older adults facing loneliness, discuss how this affects mental health, and offer an overview of coping strategies. This section is kept succinct to preserve most of the hour for participant sharing and support. Next, the chaplain provides a spiritual perspective on the topic, such as parables or prayers from different faith traditions. Then participants take turns doing “check-ins,” which consist of a greeting and brief response to the topic. Next, staff provide prompts for further discussion among participants, which usually evolves spontaneously. Near the end of the hour, the psychotherapist gives a brief summary reflection of what has been shared. The chaplain closes with a poem or prayer and blows out of the candle.
Depending on the topic and time, additional interventions can include a short writing exercise, playing a song from the era of the 1940s to the 1960s, a group sand tray therapy exercise writing something down to put in a “Godbox” or “worry box” and thereby let go of, or a short-guided breathing or meditation practice.
While the overall goal remains the same, a hallmark of S&A groups is their flexibility. Content is easily adaptable to meet the needs of participants. More often than not, the intentional safe space for older adults to share and connect is the most important aspect of the group. The primary task of facilitators is holding the space. Often something quite special unfolds among participants.
Discussion
As a psychosocial intervention, S&A groups are uniquely designed to blend the best of professional expertise with the benefits of peer support. The psychotherapist provides educational information (eg, signs/symptoms, coping skills, etc), and the chaplain provides spiritual care. Participants provide their own life experiences and perspectives.
Conducted at a day center with daily transportation services, the group is easily accessible. It is also nonstigmatizing, thus benefitting frail older adults reluctant to engage in traditional mental health services. Perhaps the most important function of the group is to nurture connections and deepen relationships among participants.
S&A groups create an invaluable opportunity for individuals with language or memory deficits to express themselves and share in a meaningful way. While they may not remember, for instance, to practice deep breathing skills taught in the group, they tend to remember the heartfelt stories that were shared. Even if participants forget the specific content, there is a kind of muscle memory that, together in this room, something special happened. They leave the group thinking, “I like it here. I feel safe and welcome. I belong.” For older adults who are lonely, this can be a rare experience, but one that is critical to well-being.
Challenges and Considerations
Inclusion Criteria
As mentioned, most S&A group participants have some degree of cognitive impairment. However, we have found that older adults with severe cognitive impairment are not usually good candidates for this style of discussion group. Potential challenges include lack of understanding of the group’s purpose, difficulty staying on topic, and difficulty reading and responding to the social cues that enable a group to flow smoothly. Another challenge we have encountered is with older adults with severe hearing impairment who cannot follow conversation even while using auditory assistive devices. When one participant is continually shouting or asking everything to be repeated, this is disruptive to other group members.
Group Dynamics
In our experience, many S&A group participants can self-regulate, engaging appropriately in a group context. However, as with any therapeutic group, participants have different temperaments and communication styles. Some may have difficulty opening up, while others’ default mode is to overshare. Managing these group dynamics requires thoughtful, sensitive facilitation. When participants self-disclose to excess (eg, retelling the same personal story in every group or commenting on everyone else’s statements), the group can feel imbalanced.
Facilitators must intervene kindly and skillfully, careful not to shame anyone while providing empathic redirection back to the topic and equitable talking time. For participants who tend to remain quiet, encouragement is provided but so is respect. It is not mandatory that everyone contributes equally. Participants can benefit from listening and being part of the group even if they do not say much.
Additional Practical Considerations
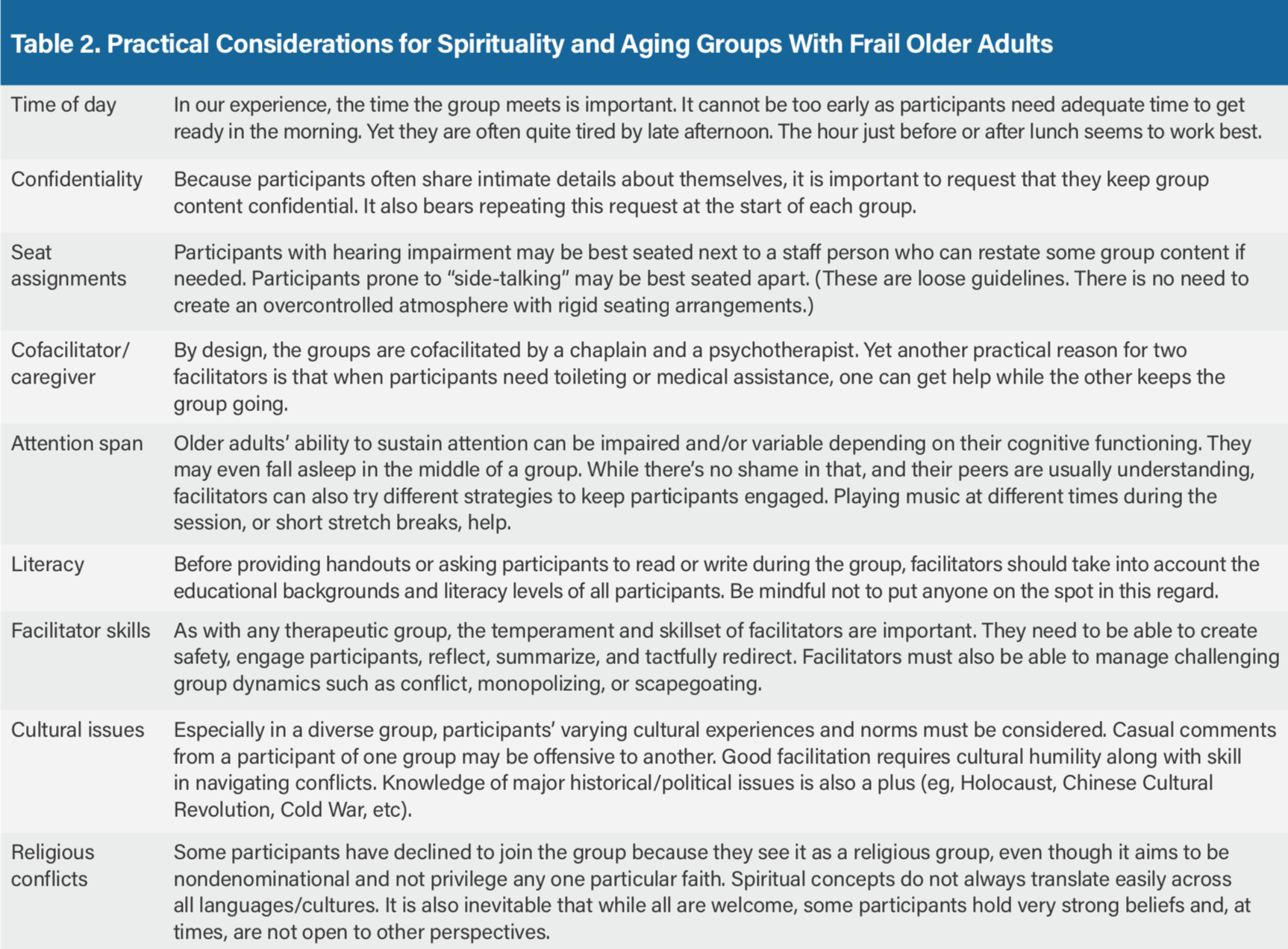
S&A groups have been held at several On Lok centers by a number of staff members. In our experience, the group is flexible in terms of content, process, and setting, and this flexibility makes it an appropriate intervention that could be implemented in a variety of long-term care settings. Additional practical issues to consider are summarized in Table 2.
Observed Benefits
Despite some minor challenges, S&A groups provide observable benefits. At the end of every group, nearly all participants warmly express gratitude for the experience. This is not just polite, compliant behavior; it is earnest appreciation.
The group is typically held the same day every month (eg, first Tuesday). However, between groups, several participants ask the psychotherapist or chaplain, “When is our next group? What will the topic be?” They are clearly looking forward to it and have verbalized as much. For some older adults with few outside activities, this is the highlight of their month.
We have also had occurrences of participants spontaneously bringing new members into the group because they enjoy it and want to share it with friends. Staff have responded flexibly to these requests—yet in some cases, the friend is not a good match for the group. For example, a participant with dementia became anxious, was unable to remain seated, and had to leave the room prior to the meeting’s end. However, the participant who brought him simply wanted her friend to have the benefit of meaningful conversation.
Clinical Implications
S&A groups provide a venue that is different from everyday socialization in other settings. For those who tend to put a positive spin on things or minimize problems, these groups allow them to open up about what is really going on. They notice their peers are facing similar challenges and, as a result, feel less alone. The supportive peer setting allows them to serve both as helpers and recipients of help, which strengthens social bonds.19
There are two women in one of our groups who both like to joke, “I’m not a people person,” making fun of their tendency to isolate because of temperament and long-standing habits. Yet the S&A group has created a venue where their wry senses of humor formed the cornerstone of trust and security to forge new relationships.
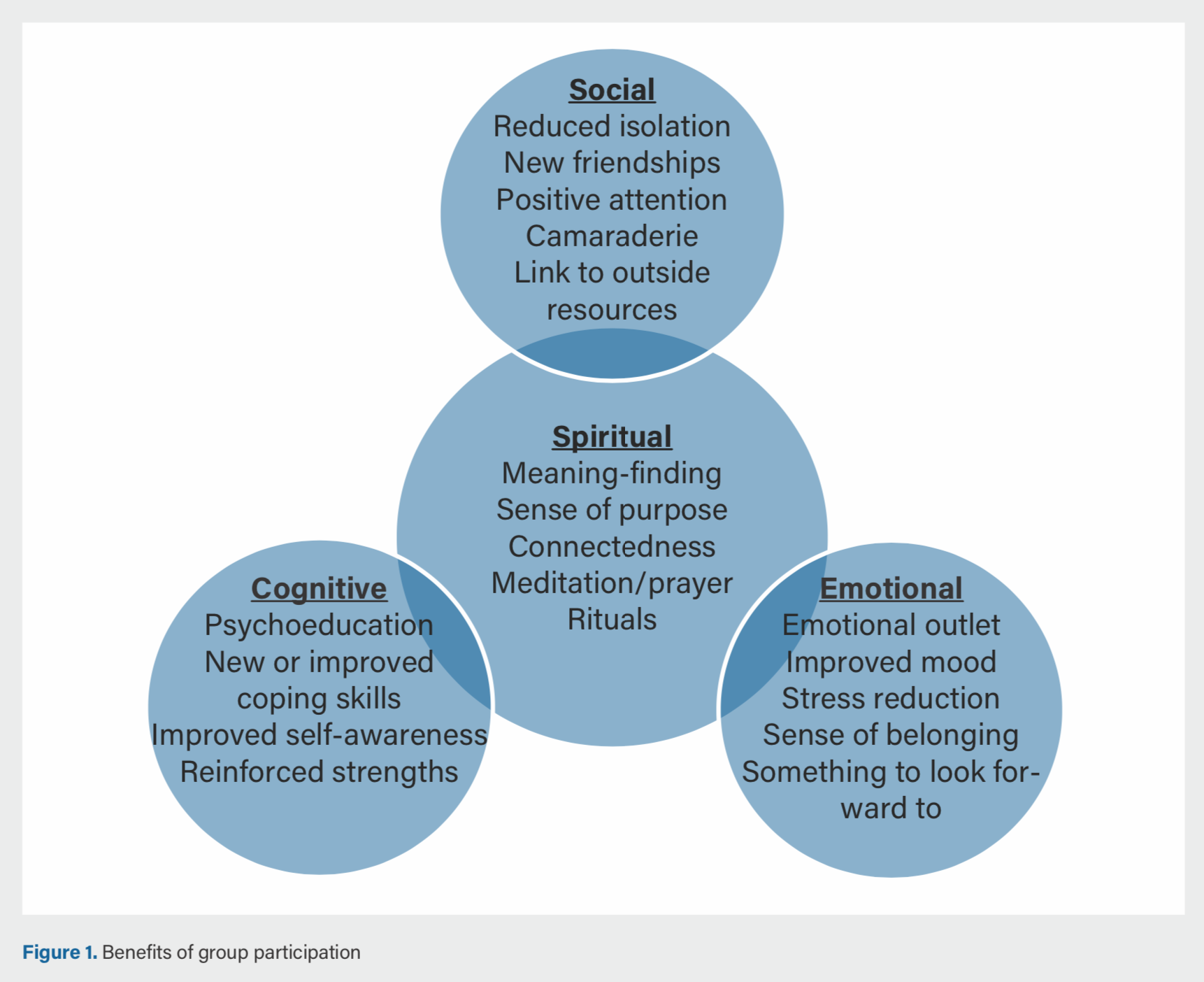
Staff observe and participants report many benefits of S&A groups (Figure 1). In addition to reduced isolation and enhanced social connections, participants report a greater sense of meaning and purpose and demonstrate improved coping skills. In a recent group that discussed the holiday blues, one participant offered to be “on-call” for other participants home alone on Christmas day. This prompted several group members to spontaneously exchange phone numbers during the group. Most had never done this before. We later learned that several of them did call one another, an act that provided joy for both the caller and the receiver, whether home alone or not. One woman put it this way: “She was so surprised that anyone thought of her, and we both laughed so hard.”
For older adults who are isolated, the benefits of group participation and belonging might seem obvious. But even for staff, who are likely to be younger, with full, busy lives, the experience offers benefit. S&A groups create a regular, structured time for mindful presence. It deepens staff relationships with participants and with each other. Many staff also feel a greater sense of satisfaction with their work and a renewed commitment to person-centered care.
References
1. Eng C, Pedulla J, Eleazer GP, McCann R, Fox N. Program of All-inclusive Care for the Elderly (PACE): an innovative model of integrated geriatric care and financing. J Am Geriatr Soc. 1997;45(2):223-232.
2. Li GK, Phillips C, Weber K. On Lok: a successful approach to aging at home. Healthc Pap. 2009;10(1):44-49.
3. Ginsburg IF, Eng C. On-site mental health services for PACE (Program of All-inclusive Care for the Elderly) centers. J Am Med Dir Assoc. 2009;10(4):277-280.
4. Centers for Disease Control and Prevention and National Association of Chronic Disease Directors. The State of Mental Health and Aging in America Issue Brief 1: What Do the Data Tell Us? Atlanta, GA: National Association of Chronic Disease Directors; 2008.
5. Unützer J, Katon W, Callahan CM, et al. Collaborative care management of late-life depression in the primary care setting: a randomized controlled trial. JAMA. 2002;288(22):2836-2845.
6. US Department of Health and Human Services. Mental Health: A Report of the Surgeon General. Rockville, MD: US Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, Center for Mental Health Services, National Institutes of Health, National Institute of Mental Health; 1999.
7. Conner KO, Copeland VC, Grote NK, et al. Mental health treatment seeking among older adults with depression: the impact of stigma and race. Am J Geriatr Psychiatry. 2010;18(6):531-543.
8. Lewis MM. Spirituality, counseling, and elderly: an introduction to the spiritual life review. J Adult Dev. 2001;8(4):231-240.
9. Parker MW, Bellis JM, Bishop P, et al. A multidisciplinary model of health promotion incorporating spirituality into a successful aging intervention with African American and white elderly groups. Gerontologist. 2002;42(3):406-415.
10. Puchalski C. The role of spirituality in health care. Proc (Bayl Univ Med Cent). 2001;14(4):352-357.
11. Kennedy GA, Macnab FA, Ross JJ. The effectiveness of spiritual/religious interventions in psychotherapy and counselling: a review of the recent literature. Melbourne: PACFA; 2015.
12. Stanley MA, Bush AL, Camp ME, et al. Older adults’ preferences for religion/spirituality in treatment for anxiety and depression. Aging Ment Health. 2011;15(3):334-343.
13. Agronin M. Group therapy in older adults. Curr Psychiatry Rep. 2009;11(1):27-32.
14. Syed Elias SM, Neville C, Scott T. The effectiveness of group reminiscence therapy for loneliness, anxiety and depression in older adults in long-term care: a systematic review. Geriatr Nurs. 2015;36(5):372-380.
15. Lindberg DA. Integrative review of research related to meditation, spirituality, and the elderly. Geriatr Nurs. 2005;26(6):372-377.
16. Zimmer Z, Jagger C, Chiu CT, Ofstedal MB, Rojo F, Saito Y. Spirituality, religiosity, aging and health in global perspective: a review. SSM Popul Health. 2016;2:373-381.
17. Lawler-Row K, Elliott J. The role of religious activity and spirituality in the health and well-being of older adults. J Health Psychol. 2009;14(1):43–52.
18. Gum A, Areán PA. Current status of psychotherapy for mental disorders in the elderly. Curr Psychiatry Rep. 2004;6(1):32-38.
19. Griffin M, Waller MV. Group therapy for the elderly: one approach to coping. Clin Soc Work J. 1985;13(3):261-271.

