


Infections in Older Adults: The Art of Early Recognition
Abstract
Older adults are at greater risk for infection due to underlying immune senescence, multiple comorbidities, and communal residence. They are also at higher risk of poor outcomes not only because of frailty but also because of the high risk of infection with resistant organisms. In the context of long-term care facilities, patients often require empiric use of broad-spectrum antibiotics. Challenges in the evaluation and management of infection in the older adult include absent or blunted signs and symptoms at initial presentation. Vigilance is required to identify nonspecific symptoms, including confusion, decline in functional status, generalized weakness, anorexia, stroke mimics, and falls. Several scoring systems have been developed to assist with clinical decision-making when diagnosing infections in the older adult. Treatment of infection emphasizes the importance of optimal antibiotic dosing based on renal function.
Citation: Ann Longterm Care. 2021.
DOI: 10.25270/altc.2021.07.00002
Received July 30, 2020; accepted January 4, 2021.
Published online September 21, 2021.
Introduction
Compared with younger adults, older adults are more likely to contract certain infections and have higher morbidity and mortality.1 Specifically, pneumonia and influenza are among the most common mortality causes.2 Infections of the urinary tract, lower respiratory tract, and skin and soft tissue, as well as intra-abdominal infections appear to have a higher incidence in older adults. The mortality rates of most of these infections are at least three times higher in older patients than in younger adult patients with the same disease.3
In the long-term care setting, the majority of people who live in long-term care facilities (LTCFs) are frail or pre-frail, and older. More than 4 million Americans are admitted to or reside in nursing homes (NHs) and skilled nursing facilities each year, and nearly 1 million people reside in assisted living facilities.4 Data on infections in LTCFs are limited, but it has been estimated that 1 to 3 million serious infections occur every year in these facilities.5 Infections are a major cause of hospitalization and mortality, with as many as 380,000 LTCF residents dying of infections every year.5 The reported incidence of infections in such facilities varies depending on the type of institution and the frailty of its residents, but it is estimated to be 10 to 20 infections per 100 residents per month. Coupled with comorbidities and declining functional status, frailty leads to increased morbidity and mortality, including from infection. It also blunts the early infection signs, leading to delays in treatment.6 Nearly 75% to 80% of infections in this setting are caused by urinary tract infections (UTIs), lower respiratory tract infections, and skin and soft tissue infections, which include infected pressure wounds.6
Older adults in general, whether they reside in the community or LTCFs, are highly vulnerable to infections because of their frailty, physical disabilities, and altered host resistance. This article summarizes the factors contributing to increased risk of infection in older adults, attempts to characterize challenges we can monitor when diagnosing infections, and reviews common infections and scoring systems that can be applied to assist with clinical decision-making when diagnosing these infections.
Factors Contributing to Increased Risk of Infection in Older Adults
Natural barriers to infection within the skin, lungs, and gastrointestinal tract often lose effectiveness with age, allowing invasion of pathogenic organisms. The aging immune system shows withering of the cellular and humoral immunity, including decreased cell populations, loss of proliferating capacity of immune cells, and decreased production of cytokines. This loss of immune function can lead to high risk of intracellular pathogens.7 Decreased antibody response to vaccines, related to low toll-like receptors, senescence of CD8 T cells, reduced CD4+ naïve, and changes in B-cell biology can also contribute to a blunted immune response.8
Immunosuppression is augmented by concomitant medical problems, such as diabetes mellitus, chronic obstructive pulmonary disease, and heart failure, as well as malnutrition and polypharmacy, which have been noted to render older adult patients more susceptible to common infections and increase the exhibition of poorer vaccine responses.9
Blunted physiologic reserves in older adults cause various changes that increase risk of infection, such as decreased cough reflex, impaired arterial and venous circulation, decreased detrusor muscle tonicity, decreased gastric acidity, and prostate enlargement.
Communal residence in NHs and time spent at community social centers contribute to increased risk of infection in older adults. Institutionalization is a major risk factor for acquiring infection and exposure to antibiotic-resistant organisms.10 Methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant Enterococcus (VRE), fluoroquinolone-resistant Streptococcus pneumoniae, and multidrug resistant gram-negative bacilli tend to be more common in institutions.11 Antibiotic resistance is facilitated by frail hosts, proximity of residents, and persistent antibiotic pressure in this context. Indwelling devices, such as urinary catheters, intravenous catheters, feeding tubes, and tracheostomies, are more common in older adults and contribute to an increased susceptibility to infection.
Challenges in Diagnosing Infection
Older adults often present with nonspecific decline from their baseline functional status. Cognitive impairment contributes to the atypical presentation of infections, which further reduces their capacity to communicate symptoms. The classical manifestations of infection, fever, and leukocytosis, may be absent or blunted in 20% to 30% of cases.12 Fever can be absent in 30% to 50% of frail older adults, even in cases of serious infections, such as pneumonia or endocarditis.13 Thermoregulation mechanisms, such as shivering, vasoconstriction, hypothalamic regulation, and thermogenesis by brown adipose tissue, are impaired in older age and can be responsible for these presentations. Women, patients with dementia, patients who are dependent in their activities of daily living, and patients with a BMI less than 20 may be at particularly high risk for this presentation.14
In a prospective study of patients over 75 years of age in the emergency department setting, it was demonstrated that a tympanal body temperature higher than 37.3°C (99.14°F) and a rectal body temperature higher than 37.8°C (100.04°F) is a reliable marker of a bacterial infection.14,15 Viral illness presents with fever in less than 5% of cases.14 The definition of fever in older adults is a temperature of 37.8°C (100°F) and tends to be associated with markers of serious illness more than 75% of the time.16 But severe infection may occur in the absence of fever. Failure to mount a febrile response to infection has been noted in NH patients.17 Mean baseline morning rectal temperature was 37°C in 22 patients whose oral temperatures could not be easily determined. The mean oral temperature of 85 other residents was 37.3°C. Diurnal variation was only 0.3°C for rectal temperatures and 0.2°C for oral temperatures. 14 In another study, 74 afebrile hospitalized geriatric inpatients were similarly studied to determine the normal range of temperatures for the frail older adult.18 This study established the upward limits for normal temperatures: 37.5°C rectal, 37.3°C oral, 37°C axillary, and 37°C proximal auditory canal.
Fever of unknown origin often occurs in older adults. It is defined as temperature greater than 38.3°C (101°F) for 3 weeks and undiagnosed after 1 week of medical evaluation.19 The etiology varies and may include abscess, bacterial endocarditis, tuberculosis, perinephric abscess, or osteomyelitis. Giant cell arteritis and polymyalgia rheumatica account for 10% of fever of unknown origin and should be held high in the differential diagnosis, especially in context of an elevated erythrocyte sedimentation rate and abnormal liver function tests.20 Malignancy, especially lymphoma, drug fever, deep vein thrombosis, and hyperthyroidism, should also remain high in the differential diagnosis of a febrile older adult.
Pneumonia in the Older Adult
In the United States, pneumonia and influenza combined rank high and are among the leading causes of death in patients older than 65 years of age.21 Morbidity and mortality for pneumonia increases dramatically with age. Half of all cases of pneumonia involve patients over the age of 65 years.22 For NH residents, pneumonia is the second leading cause of infection and the second leading cause of bacteremia. Predisposing factors leading to high prevalence include aging of the respiratory tract and lung tissue, changes in the mucocilliary transport system associated with age and smoking, and changes in lung capacity, elasticity, and compliance. Additionally, etiology can be associated with microaspiration of bacterial pathogens colonizing the oropharynx in the setting of dysphagia.23 The prevalence of dysphagia in NHs is approximately 50%, and 30% of older adults with dysphagia develop aspiration.24
Some of the classic symptoms of pneumonia in older adults include productive cough, fever, pleurisy, and rigors. However, only 34% of NH patients were noted to have a cough in the setting of pneumonia compared with 60% of community dwellers.25
The most common causative organism in community-acquired pneumonia (CAP) and nursing home–acquired pneumonia (NHAP) patients is S pneumoniae and is isolated from sputum in 20% to 30% of CAP cases in older adults.26 Haemophilus influenzae tends to occur in patients who have chronic lung disease, are male, and present with productive cough.27 Legionella pneumophila infection is sporadic, mainly occurring in summer or fall and may be found in the water condensed from air conditioning. Mycoplasma pneumoniae is an atypical pathogen less likely to be found in older adults. S aureus occurs with nosocomial infection, and these pneumonias tend to have multilobar infiltration, are often associated with bacteremia, and classically occur after influenza. Gram-negative bacilli are more common in NHs, accounting for 12% of NHAP cases.28 A causative organism is not identified in 60% of older adults with pneumonia.29 A newly discovered agent, human metapneumovirus, should be considered in presence of bronchospasm or if the patient exhibits wheezing.30
NH-acquired pneumonia fits under the umbrella term of healthcare-associated pneumonia and is defined as pneumonia occurring under the following conditions: (1) within 48 hours of admission to an LTCF or NH; (2) if the patient has been treated with intravenous antibiotics, chemotherapy, or wound care in the past 30 days while in an LTCF or NH; (3) if the patient has been hospitalized in an acute care setting for 2 days or more in the preceding 90 days; or (4) if the patient attends hemodialysis sessions. NH–acquired pneumonia is associated with increased comorbidity and poorer functional status. The mortality rate of NHAP is 19% to 53% compared with 8% to 14% of CAP.31 With NHAP, gram-negative rods, anaerobes, and S aureus are more common.31 Pseudomonas rates vary from 4% to 25% but can be as high as 52%.31
Aspiration pneumonia is common in the NH population and is often associated with oropharyngeal dysphagia and regurgitation of gastric contents. Inadequate oral care significantly increases the risk for developing pneumonia.32 Dental plaque has been particularly studied as a source of bacteria that may cause respiratory infections. A study in Japan showed an association between periodontal disease and increased mortality from pneumonia.32
Urinary Tract Infections
UTIs are also very common infections in older adults and should be considered a spectrum of infections from asymptomatic bacteriuria and cystitis to pyelonephritis and urosepsis, with a mortality rate of 20% to 40%.33 The prevalence in the community is 5% to 30%, but in the NH it rises to 17% to 55% of women and 15% to 31% of men.31 Anatomic changes with aging, such as changes in prostatic size, changes in vaginal flora associated with menopause, obstructive uropathy (from pelvic fractures, tumors, gastrointestinal disease, kidney stones, or blood clots), and anatomic changes related to childbirth or reproductive surgery, such as higher rates of incontinence, frequent urologic instrumentation, comorbid diseases, and medications that alter bladder function, all lead to a high incidence of UTIs. The most common pathogens are Escherichia coli, Proteus, Klebsiella, Enterococcus, Pseudomonas, and Staphylococcus. The prevalence of gram-positive organisms has also been increasing.34 A catheter change in the setting of UTI is associated with improved clinical outcomes.
UTIs have dramatically increased since 2000, particularly in those aged 85 years and over.35 The incidence of sepsis and its associated mortality increases disproportionately with age, and UTI in men is more likely to be severe. The diagnosis again can be problematic because these patients are less likely to present with typical urinary symptoms compared to younger patients. Many markers for UTIs have been studied, but the gold standard for diagnosis of a UTI remains a positive urine culture. Delaying or withholding antibiotics in older adults with clinical symptoms of UTI seems to be associated with a higher risk of sepsis and death.36 Recent studies show that bloodstream infections are significantly more common in patients who had delayed administration of antibiotics. Patients not treated immediately were nearly twice as likely to be admitted to hospital compared with patients who were treated quickly.37
Bacteremia
In the same context of vague presentation, bacteremic older adults are more likely to have gram-negative rods isolated, which tend to be from gastrointestinal and genitourinary sources. This trend seems to increase steeply during the eighth and ninth decades of life.38 Mortality of bacteremia increases with age, with gram-negative bacteremia mortality rates of 37% to 50% in older adults.38 Diabetes mellitus doubles the risk of bacteremia. Other risk factors include cardiovascular disease, neuropsychiatric disease, malignancy, stroke, recent invasive procedures, and presence of indwelling catheters.39 As with other infectious states discussed, absence of fever cannot be taken as proof of absence of bacteremia. Normal white blood cell count is present in 20% to 45% of older bacteremic patients.40 Independent predictors for bacteremia include change of mental status, vomiting, and white blood cell count band forms greater than 6.40 gram-negative bacteremia is most common and accounts for 70% of patients, followed by gram-positive bacteremia at 25%; anaerobes account for less than 10%, and polymicrobial infections at 5% to 17%.40 E coli is the most commonly isolated bacteria, accounting for 22% to 54% of the cases, with other gram-negative isolates such as Klebsiella pneumoniae at 8% to 16% and pseudomonas at 4% to 14%, and gram-positives, such as S pneumoniae at 4% to 20%, S aureus at 4% to 14%, Enterococcus at 3% to 9%, and viridans streptococcus at 4%.40 S aureus bacteremia is more common in residents of LTCFs than in community-dwelling older adults. It is also associated with high mortality, at 20% to 37% in most studies.41
Biomarkers and Scores Used in Diagnosis and Severity Prediction of Infection in the Older Adult
It has become increasingly evident that additional investigation of prognostic modeling is necessary, as the aging population is rapidly increasing. Prognostication of patients with pneumonia and sepsis can be particularly challenging. The Table summarizes biomarkers and scores used in the diagnosis and evaluation of severity of different infections in older adults.
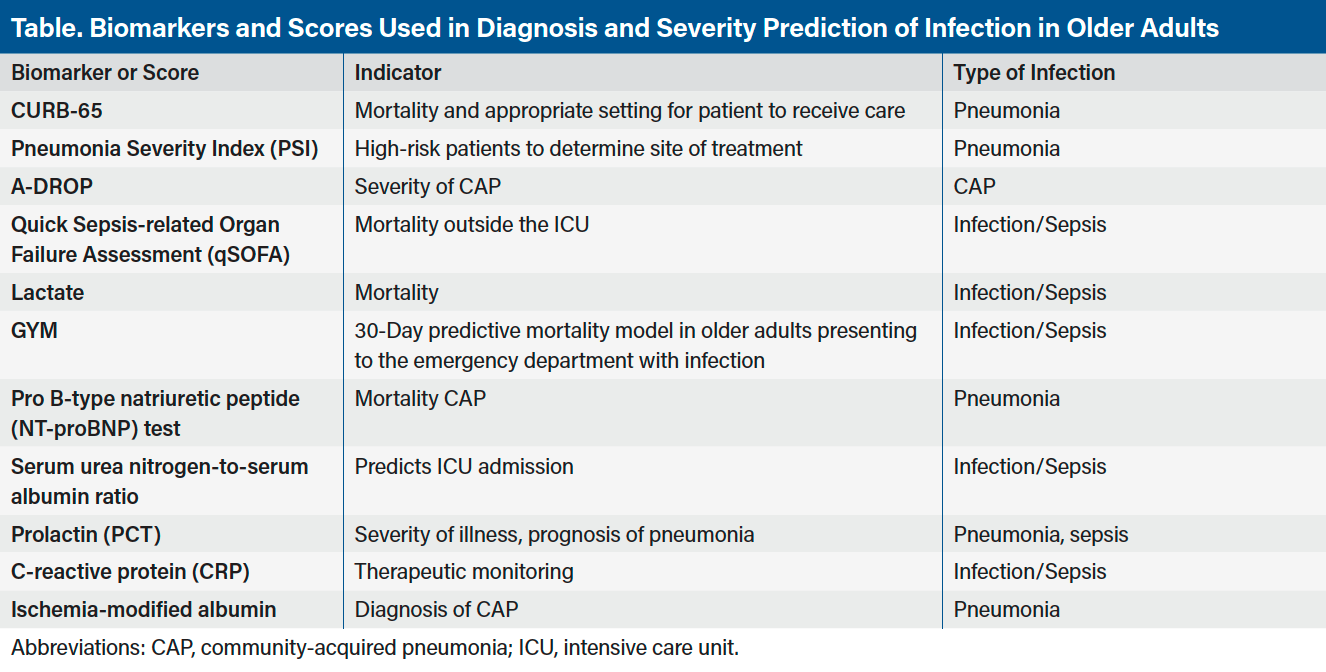
The CURB-65 score, consisting of confusion, uraemia, respiratory rate of 30 breaths per minute, low blood pressure (BP), and age 65 years or older, has been validated in older adults,42 and it can indicate mortality and the appropriate setting for patient to receive care.43 The Pneumonia Severity Index (PSI) is widely applied and risk-stratifies patients with CAP to determine whether patients can be treated as inpatient or outpatient. It includes parameters such as residence in NH, neoplastic disease, liver disease, congestive heart failure, cerebrovascular accident, renal disease, altered mental status, respiratory rate of more 29 breaths per minute, low BP, high temperature, fast pulse, serum urea nitrogen, pH, sodium plasma levels, glucose levels, hematocrit, and pleural effusion observed on x-ray. The PSI score was the best indicator predicting different clinical outcomes of older adult patients with CAP among pro B-type natriuretic peptide (NT-proBNP) test, CURB-65, and APACHE II.44 Another score comparable to CURB-65 in assessing the severity of CAP is the A-DROP, which includes parameters such as sex, serum urea nitrogen greater than 210, respiratory failure/pulse oximetry, orientation disturbance, and low BP.45 Another easy to use tool is the Quick Sepsis-related Organ Failure Assessment (qSOFA), which uses 3 criteria: low BP (<100 mm Hg), altered mentation (Glasgow coma scale <15), and tachypnea (>22 breaths per minute). It can be applied as an easy tool for quick bedside screening that predicts mortality, but it is lacking substantial validation.46 Recent studies showed little use of qSOFA for the diagnosis of sepsis; only 24% of patient with confirmed diagnosis of sepsis fulfilled the qSOFA criteria. A lactate level of more than 2 mmol/L (18.02 mg/dL) is routinely used to assess mortality, and they are linearly associated with relative risk of mortality during hospitalization at 30 days and at 60 days, when compared with patients with a lactate level of less than 2. In studies, lactate has shown a better mortality association compared with a complete blood count or serum creatinine; however, this trend was irrelevant to infection.47
The GYM score is a 30-day predictive mortality model in older adults who present to the emergency department with infection and is based on the criteria of a Glasgow score less than 15, tachypnea (>20 bpm), and Charlson Comorbidity Index score greater than 3. It is particularly accurate for patients older than 75 years of age.48 Pro B-type natriuretic peptide levels are not only predictive of congestive heart failure, but they are also useful for risk stratification and prediction of mortality in CAP.49 However, studies indicate NT-proBNP levels are not as good of a biomarker as PSI.49 The use of serum urea nitrogen-to-albumin ratio can predict admission to the intensive care unit if high enough. However, low albumin itself can predict CAP.50 A procalcitonin test (PCT) may also be helpful to identify severely ill older adults but not to discriminate patients with infection from those without. It is a particularly valuable diagnostic tool and can help characterize prognosis and severity of pneumonia in older adults.51 In a recent meta-analysis, the diagnostic accuracy of the PCT test was not inferior in older patients with sepsis compared with younger patients, hence not influenced by immunosenescence.52 In a study of older patients admitted to an acute geriatric care unit, a PCT level of 0.5 ng/mL was associated with an infection at admission together with other parameters studied. However, in the cases that the PCT test had good specificity (94%), it had low sensitivity (24%).53 A false-negative PCT test was related to lower severity of infection (lower inflammatory reaction and lower acute renal failure) than a true-positive PCT test. In other studies, sensitivity and specificity of PCT to bacterial infection with the cut-off value of 0.5 ng/mL was 72% and 92%, respectively.54
C-reactive protein (CRP) is another marker of inflammation that seems to rise 6 hours after infection and peaks at 48 hours, has a half-life of 19 hours, and is affected by immunosenescence but not by comorbidities. It can therefore be used for therapeutic monitoring. Rises are more sensitive than a PCT test but are less specific.55 Lastly, the level of ischemia-modified albumin has been studied in the diagnosis of CAP in the emergency department and has so far shown promising correlation with CRP, with sensitivity of 75.3% and specificity of 92.3%.56 For severity indicators of pneumonia and when comparing NHAP with CAP, it is apparent that NHAP has greater mortality based on patient characteristics and coexisting illnesses; pathogens differed. Of note, the existing and aforementioned severity indicators (ie, CURB-65, A-DROP, PSI) have less prognostic value for NHAP.57
Antibiotic Dosing When Treating Infection in Older Adults
The rule “start low and go slow” is true for most drugs in older adults, but for antibiotics intending to treat serious infections, the rule changes. Older patients should receive a first antibiotic dose at the highest level with known safety profile, with subsequent dosing to maintain drug levels in the treatment range.58 Patients with indwelling catheters or those who reside in a facility should have broad coverage based on their risk for resistant organisms. Broad coverage is detrimental in engendering resistance and increasing the risk of Clostridium difficile. Currently, the Centers for Disease Control and Prevention recommends an antibiotic time-out at 48 hours after initiating therapy and de-escalation to narrow spectrum treatment if culture results are available.59
Empiric antibiotic selection in older patients with CAP, if seen on an outpatient basis, can be started on doxycycline, a macrolide, or a fluoroquinolone; however, if concerns for penicillin-resistant S pneumoniae infection arise, then a fluoroquinolone would be the antibiotic of choice. If aspiration pneumonia is suspected, amoxicillin/clavulanate potassium or a fluoroquinolone would be considered as first choice. For hospitalized patients, the antibiotic of choice is a cephalosporin with a macrolide or a beta-lactam/beta-lactamase inhibitor combined with a macrolide, or fluoroquinolone alone.60
Oseltamivir is approved for treatment of influenza; however, it needs to be implemented within 48 hours of the onset of illness, which is difficult because most patients treat their illness at home for several days before seeking treatment from a physician.
Treatment of suspected UTIs should be directed to organisms identified by Gram stain and culture. Polymicrobial infections occur in about 30% of patients, more often in the setting of a catheter or recent broad-spectrum antibiotic use. Treatment of asymptomatic bacteriuria does not appear to reduce morbidity and mortality and may increase the likelihood of development of drug-resistant microorganisms and adverse reactions to antibiotics. Exceptions include patients scheduled for genitourinary procedures who have obstructive uropathy, stones, or a history of symptomatic infections.61 Older adults commonly present with MRSA. Vancomycin is the treatment of choice with or without gentamicin in cases of UTI and pneumonia. For VRE treatment, antibiotic choices vary by strain and resistance.62
Interventions for Prevention
Prevention of infection in older adults is of prime importance. Undernutrition is common and has an adverse effect on the immune system. Both protein and micronutrient deficits affect immunity, with key players being zinc, selenium, folic acid, and vitamins C, E, B6, and B12; thus, supplementation is important to consider in this patient population.63-66 Nutritional supplements have frequently been the focus of strategies to boost immune responses in clinical trials,67 but randomized controlled trials with clinical end points are rare and often report conflicting findings.68-70 Hence, controversy exists concerning every nutritional regimen tested to date. For example, while vitamin E deficiency is rare, intake above the recommended level has been shown to enhance T-cell function in aged animals and humans. This effect is believed to lead to increased resistance to influenza infection in animals and reduced incidence of upper respiratory infection in older adults. However, vitamin E is associated with adverse cardiac outcomes, namely heart failure, and caution is advised with its use. Zinc deficiency, common in older adults, is linked to impaired immune function and increased risk for acquiring infection, which can be rectified by zinc supplementation. However, higher than recommended upper limits of zinc may adversely affect immune function. Increased intake of fish or n-3 polyunsaturated fatty acids may be beneficial to inflammatory and autoimmune disorders, as well as to several age-related diseases. Conversely, the immunosuppressive effect of fish oils on T-cell–mediated function has raised concerns regarding their impact on resistance to infection. The studies published thus far describe a critical role for nutrition in maintaining the immune response of older individuals, but they also indicate the need for a more in-depth, holistic approach to determining the optimal nutritional strategies that would maintain a healthy immune system in older adults and promote their resistance to infection and other immune-related diseases. There are currently no discrete guidelines regarding supplementation, but the dominating notion is that supplementation may cause more harm than good, except for vitamin D and vitamin B12 if found low.
Immunization plays a key role in preventing infections. Vaccinations such as Tdap (tetantus, diphtheria, pertussis), pneumococcal, seasonal influenza, and zoster should be visited in all medical encounters. In the United States, 60% to 65% of older adults receive the pneumococcal vaccine and 70% to 75% receive the influenza vaccine.72 Immunization for influenza and pneumococcus are the most important preventive strategies. While pneumococcal vaccination may not prevent pneumonia in older adults, rates of bacteremia and invasive pneumococcal disease are decreased in immunized patients, and mortality in older patients hospitalized with pneumonia is lower for patients who were vaccinated before admission.7
Conclusion
In summary, infection risk in older adults is elevated because of immune deficiencies, comorbidities, and changes in environmental setting. These patients are highly likely to present atypically; thus, care needs to be taken in noticing subtle, vague changes in mental and functional status. Early identification of infection can prove life-saving in older adults because they are at high risk for poor outcomes.
Affiliations, Disclosures, & Correspondence
Authors: Fotini Debonera, MD, PhD¹ • B Brent Simmons, MD FAAFP²
Affiliations:
1Department of Family Medicine, Division of Geriatrics, UPMC Home Visits Program, Litiz, PA
2Department of Family, Community and Preventive Medicine, Division of Geriatrics,Tower/Drexel Medical group, Drexel University School of Medicine, Philadelphia, PA
Disclosures:
The author report no relevant financial relationships.
Address correspondence to:
Fotini Debonera, MD, PhD
Department of Family Medicine
Division of Geriatrics
UPMC Home Visits Program
Litiz, PA
Email: deboneraf@upmc.edu
References
1. Yoshikawa TT. State of infectious diseases health care in older persons. Clin Geriatr Med. 1999;7:55-61.
2. Leading causes of death and number of deaths according to age: United States, 1980 and 1993. In: Health, United States, 1995. Public Health Service; 1996. Publication No. 96-1232.
3. Yoshikawa TT. Epidemiology and unique aspects of aging and infectious diseases. Clin Infect Dis. 2000;30(6):931-933.
4. Long-term care providers and services user in the United States, 2015-2016. National Center for Health Statistics Vital and Health Statistics. 2019;3(43). Accessed July 30, 2020. https://www.cdc.gov/nchs/data/series/sr_03/sr03_43-508.pdf
5. Serious infections and outbreaks in LTCFs. Centers for Disease Control and Prevention; 2020. Accessed July 30, 2020. https://www.cdc.gov/longtermcare/staff/report-publications.html
6. Yoshikawa TT, Norman DC. Approach to fever and infection in the nursing home. J Am Geriatr Soc. 1996;44:74-82.
7. Weiskopf F, Weinberger B, Grubeck-Loebenstein B. The aging of the immune system. Transpl Int. 2009;22:1041-1046.
8. Scholz, JL, Diaz A, Riley RL, et al. A comparative review of aging and B cell function in mice and humans. Curr Opin Immunol. 2013;25:504.
9. Castle SC, Uyemura K, Fulop T, Makinodan T. Host resistance and immune responses in advanced age. Clin Geriatr Med. 2007;23:463-467.
10. Kuproni BA, Richards CL, Whitney CG, Active bacterial core surveillance team. Invasive pneumococcal disease in older adults residing in long term care facilities and in the community. J Am Geriatr Soc. 2003;51:1520-1525.
11. O’Fallon E, Schreiber R, Kandel R, D’Agata EM. Multidrug-resistant gram-negative bacteria at a long-term care facility: assessment of residents, healthcare workers and inanimate surfaces. Infect Control Hosp Epidemiol. 2009;30:1172-1175.
12. Norman DC. Special infectious disease problems in geriatrics. Clin Geriatrics. 1999;(1):3-5.
13. Musgrave T, Verghese A. Clinical features of pneumonia in the elderly. Semin Respir Infect. 1990;5:269-287.
14. Norman DC. Fever in the elderly. Clin Infect Dis. 2000;31:148-151.
15. High KP, Bradely SF, Gravenstein S, et al. Clinical practice guideline for the evaluation of fever and infection in older adult residents of long term care facilities: 2008 update by the Infectious Diseases Society of America. Clin Infect Dis. 2009;48:149-155.
16. Downton JH, Andrews K, Puxty JAH. Silent pyrexia in the elderly. Age Ageing 1987;16:41-44.
17. Castle SC, Norman DC, Yeh M, Miller D, Yoshikawa TT. Fever response in elderly nursing home residents: are the older truly colder? J Am Geriatr Soc. 1991;39(9):853-857.
18. Darowski A, Weinbert JR, Guz A. Normal rectal, auditory canal, sublingual and axillary temperature in elderly afebrile patients in a warm environment. Age Ageing. 1991;20:113-119.
19. Tal S, Guller V, Gurevich A. Fever of unknown origin in older adults. Clin Geriatr Med. 2007;23:649-655.
20. Mourad O, Palda V, Detsky AS. A comprehensive evidence-based approach to fever of unknown origin. Arch Intern Med. 2003;163:545.
21. Kochanek MA, Murphy BS, Xu J, Arias E. Deaths: Final data for 2017. National Vital Statistics Report. Centers for Disease Control and Prevention; 2019. Accessed July 30, 2020. https://www.cdc.gov/nchs/data/nvsr/nvsr68/nvsr68_09-508.pdf
22. Fry AM, Shay DK, Holman RC. Trends in hospitalizations for pneumonia among persons aged 65 years or older in the USA, 1988-2002. JAMA. 2005;294:2712-2719.
23. Young G, Jungho S, Ryu H. Pneumonitis and pneumonia after aspiration. J Dent Anesth Pain Med. 2017;17(1):1-12.
24. Satoru E, Hideki S, Miyagi M,1 Takae E, Okazaki T. Dysphagia, dystussia, and aspiration pneumonia in elderly people. J Thorac Dis. 2016;8(3):632-639.
25. Henig O, Kaye K. Bacterial pneumonia in older adults. Infect Dis Clin North Am. 2017;31(4):689-713.
26. El-Solh AA, Sikka P, Ramdan F, Davies J. Etiology of severe pneumonia in the very elderly. Am J Respir Crit Care Med. 2001;163:645-649.
27. Madenll LA, Bartlett JG, Dowell SF, et al. Update of practice guidelines for the management of CAP in immunocompetent adults. Clin Infect Dis. 2003;37:1405-1409.
28. Ewig S, Torres A. Is chlamydia pneumoniae an important pathogen in patients with CAP? Eur Respir J. 2003;21:741-747.
29. Stupka J, Mortensen E, Anzueto A, Restrepo M. Community-acquired pneumonia in elderly patients. Aging Health. 2009;5(6):763-774.
30. Falsey AR, Erdman, D, Anderson LJ, Walsh EE. Human metapneumovirus infections in young and elderly adults. J Infect Dis. 2003;187:785-789.
31. Montoya A, Mody L. Common infections in nursing homes: a review of current issues and challenges. Aging Health. 2011;7(6):889-899.
32. Müller F. Oral Hygiene Reduces the mortality from aspiration pneumonia in frail elders. J Dent Res. 2015; 94(3):14S-16S.
33. Om Prakash K, Raizada A. Approach to a patient with urosepsis. J Glob Infect Dis. 2009;1(1):57–63.
34. Foxman, B, Brown, P. Epidemiology of urinary tract infections, transmission and risk factors, incidence, and costs. Infect Dis Clin North Am. 2003;17:227-231.
35. Rowe T, Juthani-Mehta M. Urinary tract infection in older adults. Aging Health. 2013;9(5):2217-2223.
36. Kmietowics Z. Delaying antibiotics in over the 65s with UTI may increase risk of sepsis. BMJ. 2019;364:922-925.
37. Gharbi M, Drysdale J, Lishman H, et al. Antibiotic management of UTIs in the elderly in primary care and its association with bloodstream infections and all-cause mortality: a population based cohort study. BMJ. 2019;364:525-530.
38. Pien BC, Sundaram P, Raoof N. The clinical and prognostic importance of positive blood cultures in adults. Am J Med. 2010;123:819-822.
39. Nasa P, Juneja D, Singh O. Severe sepsis and septic shock in the elderly: An overview. World J Crit Care Med. 2012;1(1):23-30.
40. Yahav D, Eliakim-Raz N, Leibovici L, Paul M. Bloodstream infections in older patients. Virulence. 2016;7(3):341–352.
41. Norman DC. Clinical features of infection in older adults. Clin Geriatr Med. 2016;32:433-441.
42. Gianella M, Tedeschi S, Bartoletti M, Viale P. Prevention of infections in nursing homes: antibiotic prophylaxis versus infection control and antimicrobial stewardship measures. Expert Rev Anti Infect Ther. 2016;14(2):219-230.
43. Montoya A, Cassone M, Mody L. Infections in nursing homes: epidemiology and prevention programs. Clin Geriatr Med. 2016;32(3):585-607.
44. Kun X, Su LX, Han BC, et al. Analysis of the severity and prognosis assessment of aged patients with community acquired pneumonia: a retrospective study. J Thorac Dis. 2013;5(5):626-633.
45. M Ugajin, K Yamaki, N Hirasawa, T Kobayashi, Yagi T. Prognostic value of severity indications of nursing home-acquired pneumonia versus community-acquired pneumonia in elderly patients. Clin Interventions Aging. 2014;9:267-274.
46. Ramos-Rincón J, Fernández-Gil A, Merino E, et al. The quick Sepsis-related Organ Failure Assessment (qSOFA) is a good predictor of in-hospital mortality in very elderly patients with bloodstream infections: a retrospective observational study. Scientific Reports. 2019;(9):15075.
47. Del Portal D, Schofer A, Mikkelsen M, et al. Emergency department lactate is associated with mortality in older adults admitted with and without infections. Acad Emerg Med. 2010;17(3):260-268.
48. González Del Castillo J, Escobar-Curbelo L, Martínez-Ortíz de Zárate M, et al. GYM score: 30-day mortality predictive model in elderly patients attended in the emergency department with infection. Eur J Emerg Med. 2017;24(3):183-188.
49. Xiao K, Su LX, Han BC, et al, Analysis of the severity and prognosis assessment of aged patients with CAP: a retrospective study. J Thorac Dis. 2013;5(5):626-633.
50. Feng D, Zhou Y, Zou X, et al. Elevated blood urea nitrogen-to-serum albumin ratio as a factor that negatively affects the mortality of patients with hospital-acquired pneumonia. J Infect Dis Med Microbiol. 2019;16:154-174.
51. Heppner HJ, Bertsch T, Alber B, et al. Procalcitonin: inflammatory biomarker for assessing the severity of community-acquired pneumonia--a clinical observation in geriatric patients. Gerontology. 2010;56:385-389.
52. Lee SH, Chan RC, Wu JY, Chen HW, Chang SS, Lee, CC. Diagnostic value of procalcitonin for bacterial infection in elderly patients - a systemic review and meta-analysis. Int J Clin Pract. 2013;67:1350-1357.
53. Stucker F, Herrmann F, Graf J, et al. Procalcitonin and infection in elderly patients. J Am Geriatr Soc. 2005;53(8):1392-1395.
54. Gómez-Cerquera J, Daroca-Pérez R, Baeza-Trinidad R, Casañas-Martinez M. Validity of procalcitonin for the diagnosis of bacterial infection in elderly patients. Enferm Infecc Microbiol Clin. 2015;33(8):521-524.
55. Zhang H, Wang X, Zhang Q, Xia Y, Liu D. Comparison of procalcitonin and high sensitivity CRP for the diagnosis of sepsis and septic shock in the oldest old patients. BMC Geriatrics. 2017;17:173-177.
56. Bolatkale M, Duger M, Ulfer G, et al. Am J Emerg Med. 2017;35(8):1121-1125.
57. Dhawan N, Pandya N, Khalili M, et al. Predictors of mortality for nursing home-acquired pneumonia: a systematic review. Biomed Res Int. 2015;2015:285983-285990.
58. Drusano GL, Preston SL, Flowler C. relationship between fluoroquinolone area under the curve: minimum inhibitory concentration ratio and the probability of eradication of the infecting pathogen, in patient with nosocomial pneumonia. J Infect Dis. 2004;189:1590-1596.
59. Fridkin, S, Baggs J, Fagan R. Vital signs: improving antibiotic use among hospitalized patients. MMWR Morb Mortal Wkly Rep. 2014;63:194-196.
60. Thiem U, Heppner HJ, Pientka L. Elderly patients with community-acquired pneumonia: optimal treatment strategies. Drugs Aging. 2011;28(7):519-537.
61. Trautner BW, Grigoryan L, Petersen NJ. Effectiveness of an antimicrobial stewardship approach for urinary catheter associated asymptomatic bacteriuria. JAMA Intern Med. 2015;175:1120-1128.
62. Michael M, Guttmann L. MRSA and VRE therapeutic realities and possibilities. Lancet. 1997;349:1901-1906.
63. Talbott MC, Miller LT, Kerkevliet NI. Pyridoxine supplementation: effect on lymphocyte responses
in elderly persons. Am J Clin Nutr. 1987;46:659-662.
64. Mocchegiani E, Romeo J, Malavita M, et al. Age. 2013;35(3):839-860.
65. El Chakhtoura NG, Bonomo RA, Jump LP. Influence of aging and environment ofn presentation of infection in older adults. Infect Dis Clin North Am. 2017;31(4):593-608.
66. Barnett JB, Hamer DH, Meydani SN. Low zinc status: a new risk factor for pneumonia in the elderly. Nutr Rev. 2010;68:30-36.
67. High KP. Nutritional strategies to boost immunity and prevent infection in elderly individuals. Clin Infect Dis. 2001;33:1892-1898.
68. Forster SE, Powers HJ, Foulds GA. Improvement in nutritional status reduces the clinical impact of infections in older adults. J Am Geriatr Soc. 2012;60:1645-1655.
69. Barringer TA, Kirk JK, Santaniello AC. Effect of a multivitamin and mineral supplement on infection and quality of life. A randomized, double blind, placebo controlled trial. Ann Int Med. 2003;138:365-375.
70. Avenell A, Campbell MK, Cook JA. Effect of multivitamin and multimineral supplements on morbidity form infections in older people (MAVIS trial). BMJ. 2005;331:324.
71. Munkyong P, Simin NM, Dayong W. The role of nutrition in enhancing immunity in aging. Aging Dis. 2012;3(1):91-129.
72. CDC vaccination. Accessed April 2021. https://www.cdc.gov/vaccines/imz-managers/coverage/adultvaxview/pubs-resources/index.html
73. Porchia BR, Bonanni P, Bechini A, Bonaccorsi G, Boccalini S. Evaluating the costs and benefits of pneumococcal vaccination in adults. Expert Rev Vaccines 2017;16(2):93-107.
