


How Do You Perform Angiography for Your STEMI Patient in the Cath Lab?
© 2024 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Cath Lab Digest or HMP Global, their employees, and affiliates.
I read an interesting article by Levi et al1 that stimulated my curiosity on how our approach to the ST-elevation myocardial infarction (STEMI) patient has changed over the years. Beginning in 1982, my approach to the uncomplicated STEMI patient was adjusted to the trends and best practices of the time. We went from 8 French (F) to 6F femoral access, then to radial-first access; intra-aortic balloon pump (IABP) gave way to microaxial pumps for shock patients, and routine right heart cath (RHC) was nearly abandoned. I recall many discussions of the various angiographic techniques before percutaneous coronary intervention (PCI) for STEMI patients. For example, should we perform culprit vessel angiography first with diagnostic catheters, then non-culprit/target vessels, and then select an appropriate guide catheter and proceed with PCI? Many, including me, advocated for complete angiography often with the non-culprit artery first, then culprit vessel angiography using a guide catheter for the target STEMI vessel. This helped me know about left main (LM) or 3-vessel disease while getting set up to do PCI.
 In uncomplicated STEMI patients, should we do left ventriculography before or after PCI? Some insisted on left ventricular (LV) grams before PCI, while others said no need at all for LV grams. Some wanted LV end-diastolic pressure (LVEDP); others said it could wait until PCI was completed.
In uncomplicated STEMI patients, should we do left ventriculography before or after PCI? Some insisted on left ventricular (LV) grams before PCI, while others said no need at all for LV grams. Some wanted LV end-diastolic pressure (LVEDP); others said it could wait until PCI was completed.
To address the angiographic approach to STEMI, Levi et al1 studied 2 strategies with the goal of reducing needle-to-balloon (N2B) time. They compared: 1) a guide catheter and PCI first to 2) complete angiography first, followed by PCI. The guide catheter-first approach saved 10 minutes on the N2B time. No other clinical endpoint differed in the study. I wanted to share this with my colleagues and get their viewpoints. Here are my questions to them:
Question 1: Do you believe that 10 minutes makes a difference in STEMI outcomes, particularly when the onset of symptoms to emergency department (ED) is so large and variable? Keeping a low (<90- or <60-minute) door-to-balloon (D2B) time makes sense to establish protocols to make STEMI treatments shorter and is in general associated with better outcomes. But 10 minutes? The study by Nallamothu et al2 showed that every 10-minute reduction in D2B time resulted in an 8% decrease in in-hospital mortality and a 6% decrease in 6-month mortality. Wow.
Question 2: What is your best approach to the STEMI patient once in the cath lab?
 Steven L. Goldberg, Monterey, California: Mort, I cannot tell how Levi et al1 did the coronary angiography — was it with a single catheter (like a Tig or Jacky [Terumo]) or standard Judkins, requiring catheter exchanges? That seems like a crucial detail which was missing. It’s kind of surprising the reviewers didn’t pick up on that. A single catheter is likely to be much quicker. [MK: Most had radial approach; a crossover from a radial to a femoral approach occurred more in complete angio-first group (5.6% [5 of 90] versus 14.9% [14 of 94]; P=.04) due to radial artery vasospasm.]
Steven L. Goldberg, Monterey, California: Mort, I cannot tell how Levi et al1 did the coronary angiography — was it with a single catheter (like a Tig or Jacky [Terumo]) or standard Judkins, requiring catheter exchanges? That seems like a crucial detail which was missing. It’s kind of surprising the reviewers didn’t pick up on that. A single catheter is likely to be much quicker. [MK: Most had radial approach; a crossover from a radial to a femoral approach occurred more in complete angio-first group (5.6% [5 of 90] versus 14.9% [14 of 94]; P=.04) due to radial artery vasospasm.]
 David Cohen, Roslyn, New York: I think the emphasis we have had on D2B time over the last 2 decades has been critical to developing reliable and safe practices for primary PCI, and has been an important part of the great strides that have been made during my career in interventional cardiology. However, I also think that we may be overstating the importance of this single factor in our outcomes. My personal belief is that the true D2B vs mortality relationship is much weaker than has been identified in the studies (like the one by Nallamothu et al2), in part because of failure to recognize the role of unmeasured confounding. When an experienced operator has a long D2B time, there is usually a good reason for it such as delays in diagnosis, sick patient in the ED complicating transfer to the cath lab, or even tortuous anatomy making vascular/coronary access more challenging. These factors are not well documented in our datasets and often represent the true cause of increased mortality associated with longer D2B time. None of this is to say that we should ignore time to reperfusion, but simply that it probably isn’t worth focusing on D2B above all other aspects of care for the STEMI patient.
David Cohen, Roslyn, New York: I think the emphasis we have had on D2B time over the last 2 decades has been critical to developing reliable and safe practices for primary PCI, and has been an important part of the great strides that have been made during my career in interventional cardiology. However, I also think that we may be overstating the importance of this single factor in our outcomes. My personal belief is that the true D2B vs mortality relationship is much weaker than has been identified in the studies (like the one by Nallamothu et al2), in part because of failure to recognize the role of unmeasured confounding. When an experienced operator has a long D2B time, there is usually a good reason for it such as delays in diagnosis, sick patient in the ED complicating transfer to the cath lab, or even tortuous anatomy making vascular/coronary access more challenging. These factors are not well documented in our datasets and often represent the true cause of increased mortality associated with longer D2B time. None of this is to say that we should ignore time to reperfusion, but simply that it probably isn’t worth focusing on D2B above all other aspects of care for the STEMI patient.
Given these concerns, I don’t believe it’s worth sacrificing the knowledge of what’s going on in the non-infarct-related artery (IRA) for the sole purpose of reducing D2B by 5 minutes (that was the median time difference in the study by Levi and colleagues). Especially in cases where the IRA is the right coronary artery (RCA), knowing how things look in the left system can be invaluable. One of the most important benefits of primary PCI over lytics is the ability to do much more than open the IRA in a timely fashion (eg, ventriculogram, right heart catheterization [RHC], temp pacer, mechanical circulatory support [MCS]). And understanding the entire coronary anatomy prior to inflating the first balloon can allow us to think much more clearly about these sick patients earlier in the case.
My preferred approach is radial access unless I have a very high suspicion of the need for MCS, non-IRA imaging first with a diagnostic catheter, IRA imaging second with a guide, then PCI of IRA via guide (or switch back to the first vessel if I guessed wrong). I do a ventriculogram at the end of the case unless there is a major disconnect between the coronary anatomy and the degree of patient illness in which case, an LV gram and RHC get moved up the care pathway.
 Bonnie Weiner, Worchester, Massachusetts: I don’t like surprises, particularly with a patient I have just met and most likely don’t have the whole story. I start with what I think is the non-culprit artery. I don’t take a lot of pictures, just enough to be sure I am not missing something and that there are [coronary artery bypass graft (CABG)] targets should the unusual circumstance occur that I need a surgeon. No need to take excessive views. I will usually then go with a guide for the infarct artery, but have a low threshold to switch it out if I am concerned about support after taking pictures.
Bonnie Weiner, Worchester, Massachusetts: I don’t like surprises, particularly with a patient I have just met and most likely don’t have the whole story. I start with what I think is the non-culprit artery. I don’t take a lot of pictures, just enough to be sure I am not missing something and that there are [coronary artery bypass graft (CABG)] targets should the unusual circumstance occur that I need a surgeon. No need to take excessive views. I will usually then go with a guide for the infarct artery, but have a low threshold to switch it out if I am concerned about support after taking pictures.
I still like doing LV grams. I will usually do it at the end unless the pieces of the puzzle don’t seem to fit or there is a murmur I can’t otherwise explain. I discourage the residents and fellows from doing “routine” echos, something which is not always easy. If heart failure symptoms seem out of proportion [to the presentation] or the blood pressure lower than I would expect, RHC is useful. In my opinion, the pendulum has swung way too far away from [practice] that is based on old data saying that outcomes in the intensive care unit (ICU) are not improved, something not relevant to this clinical circumstance. No question in my mind that the data are useful, and can help guide therapy and avoid guesswork.
As far as the timing is concerned, the few minutes where other meaningful things like necessary diagnostic studies, and appropriate antiplatelet and anticoagulant drugs are being administered should not impact outcome. A more significant metric is actually ischemia time, which we don’t measure very accurately but D2B (or now, first medical contact to device) is a greater influence on outcome.
 Fred Welt, Salt Lake City, Utah: In our lab, most operators will use a diagnostic catheter to look at the left system first if the suspected culprit is the RCA. If there is an anterior MI, most will go up with a left guide with the rationale that little that is happening in the RCA that will influence you if the left anterior descending (LAD) is culprit. Of course, there are radial guides that can cannulate both the RCA and left systems. But we don’t use them. Personally, I don’t think LV gram should be done routinely.
Fred Welt, Salt Lake City, Utah: In our lab, most operators will use a diagnostic catheter to look at the left system first if the suspected culprit is the RCA. If there is an anterior MI, most will go up with a left guide with the rationale that little that is happening in the RCA that will influence you if the left anterior descending (LAD) is culprit. Of course, there are radial guides that can cannulate both the RCA and left systems. But we don’t use them. Personally, I don’t think LV gram should be done routinely.
 Jennifer Tremmel, Palo Alto, California: Radial approach, Ikari L3.5 guide (Terumo). [MK: Thanks, Jen. Short and sweet.]
Jennifer Tremmel, Palo Alto, California: Radial approach, Ikari L3.5 guide (Terumo). [MK: Thanks, Jen. Short and sweet.]
Ajay Kirtane, New York, New York: We know that in an individual patient, where the patient is on the ‘salvage curve’ [MK: D2B+clinical factors] influences the relative impact of a minimal decrement in D2B: if symptom onset is outside the “golden hour”, even a 5-10 minute reduction in D2B will have minimal to no impact on salvage in an individual.
As a result, once the systematic changes to reduce overall D2B have been implemented, the overenthusiastic application of D2B (a population-based process metric) can come at a cost which adversely affects some of the highest-risk patients, eg, those who require prompt diagnosis/treatment of shock BEFORE the PCI, assessment of mechanical complications (via echo, RHC, LV gram), or making a firm diagnosis that may require complete assessment of anatomy (in more complex cases of left main coronary artery disease, concomitant chronic total occlusion [CTO], multiple culprits, spontaneous coronary artery dissection [SCAD], diffuse spasm, embolic event).
 Yes, all of these are rare and in most cases, the patient will be fine going with the culprit guide [first], but not assessing the non-culprit vessel, hemodynamics, or ventricular function, and making an incomplete or missed diagnosis in the rare (higher risk, less routine) case often has even worse sequelae for that individual patient. Those are the patients we are more likely to lose through well-meaning misapplication of a process metric. High-risk patients need a clinician to think with complete information, something especially true when it comes to decisions about adjunctive use of hemodynamic support, etc.
Yes, all of these are rare and in most cases, the patient will be fine going with the culprit guide [first], but not assessing the non-culprit vessel, hemodynamics, or ventricular function, and making an incomplete or missed diagnosis in the rare (higher risk, less routine) case often has even worse sequelae for that individual patient. Those are the patients we are more likely to lose through well-meaning misapplication of a process metric. High-risk patients need a clinician to think with complete information, something especially true when it comes to decisions about adjunctive use of hemodynamic support, etc.
A fundamental premise of what we do is to make the diagnosis first and THEN treat based upon that diagnosis. “Occluded artery must open as fast as I can” is too simplified a rubric for these patients on the edge. For us [Columbia University], we start with the non-culprit vessel diagnostic angio, and possible LVEDP and/or LV gram, based upon hemodynamics and how sick the patient is. If an echo was done, we would do a RHC up front to guide decision about MCS (especially for those with shock), and THEN [go with the] culprit guide.
 Steve Ramee, Baton Rouge, Louisiana: Once again, a great question. I love the discussion and the diverse opinions submitted thus far. They illustrate how complex the treatment of STEMI really is. STEMI is an unplanned emergency and each case presents differently, but we all agree that speedy recanalization is beneficial to patient outcomes. I prefer to study the non-culprit artery first, but I like to divide the patients into three groups: 1) Those that are hemodynamically stable, 2) Those that are unstable with tachycardia or shock, and 3) Those with prior CABG.
Steve Ramee, Baton Rouge, Louisiana: Once again, a great question. I love the discussion and the diverse opinions submitted thus far. They illustrate how complex the treatment of STEMI really is. STEMI is an unplanned emergency and each case presents differently, but we all agree that speedy recanalization is beneficial to patient outcomes. I prefer to study the non-culprit artery first, but I like to divide the patients into three groups: 1) Those that are hemodynamically stable, 2) Those that are unstable with tachycardia or shock, and 3) Those with prior CABG.
1) In the hemodynamically stable patient, either radial or femoral access is fine. I try to study the non-culprit artery first, then use a guide for the culprit artery. I always use a hydrophilic guidewire (ie, Choice PT XS [Boston Scientific]) instead of a usual PCI working wire (Balance Middleweight [BMW] [Abbott]) so that it will cross the clot quickly the first time.
2) In an unstable patient with shock, tachycardia, or small pulse pressure, I prefer femoral access because I’m quicker at it, I am competent with closure devices, and I can easily establish central venous access and use MCS, RHC, or transvenous pacing, if needed.
3) In a prior CABG patient, there are often multiple vessel occlusions. I also prefer femoral access so that I can access all of the native arteries and grafts (including left internal mammary artery [LIMA]) and assist in finding the culprit vessel. Assessment of LV and valve function can be done by echo in stable patients but should be done with hemodynamics and/or ventriculography in an unstable patient.
 Michael Lim, Poplar Bluff, Missouri: I think trying to re-energize our treatment of STEMI patients is important, and the data suggesting many patients end up with successful primary PCI and subsequent heart failure coupled with the data about infarct size and heart failure is compelling [and encourages us] to be thoughtful not just about how our patients do acutely, but also over a longer timeframe. I approach the infarct-related artery first. As Jennifer [Tremmel] does, I use a radial approach and Ikari guide. If the electrocardiogram (ECG) and vessel anatomy “match”, then I go ahead and perform primary PCI — not to “shorten D2B time”, but to help patients feel better. Once reperfusion is achieved, they often calm down and relax, allowing us to move forward with far less anxiety across the entire lab. I then turn my attention to looking at everything else (Ikari Left guide will cannulate either artery in most patients and doesn’t require an exchange, as well as being able to measure an LVEDP). I don’t routinely perform V-grams anymore. I will do one when the situation between ECG, symptoms, and coronary anatomy is not straightforward (note: I ALWAYS do them with a pigtail and an automated injection. If it’s going to be done, it should be done right). [MK: see CLD November 2013, “The End of End-Hole Left Ventriculography – A Consensus of Operators”).
Michael Lim, Poplar Bluff, Missouri: I think trying to re-energize our treatment of STEMI patients is important, and the data suggesting many patients end up with successful primary PCI and subsequent heart failure coupled with the data about infarct size and heart failure is compelling [and encourages us] to be thoughtful not just about how our patients do acutely, but also over a longer timeframe. I approach the infarct-related artery first. As Jennifer [Tremmel] does, I use a radial approach and Ikari guide. If the electrocardiogram (ECG) and vessel anatomy “match”, then I go ahead and perform primary PCI — not to “shorten D2B time”, but to help patients feel better. Once reperfusion is achieved, they often calm down and relax, allowing us to move forward with far less anxiety across the entire lab. I then turn my attention to looking at everything else (Ikari Left guide will cannulate either artery in most patients and doesn’t require an exchange, as well as being able to measure an LVEDP). I don’t routinely perform V-grams anymore. I will do one when the situation between ECG, symptoms, and coronary anatomy is not straightforward (note: I ALWAYS do them with a pigtail and an automated injection. If it’s going to be done, it should be done right). [MK: see CLD November 2013, “The End of End-Hole Left Ventriculography – A Consensus of Operators”).
What to do about elevated LVEDPs remains an open question. There is data showing that this [a high LVEDP] is related to larger infarct size, but nothing that I know of changes that trajectory. Potentially, measuring the index of microcirculatory resistance (IMR) routinely to identify those with higher degrees of microvascular dysfunction and provide therapy (eg, SSO2 [ZOLL Medical]) may also be useful, but as yet, is not commonly done. I haven’t seen a great need for “urgent” bypass surgery and believe that patients are better off being stabilized and getting farther away from their acute event prior to undergoing cardiac surgery should anatomy present itself fitting for surgery.
 Neil Kleiman, Houston, Texas: I agree 100% with everything David [Cohen] has said. Sometimes information from the non-culprit helps guide strategy. There is no substitute for a little bit of planning.
Neil Kleiman, Houston, Texas: I agree 100% with everything David [Cohen] has said. Sometimes information from the non-culprit helps guide strategy. There is no substitute for a little bit of planning.
Jeffrey Moses, Roslyn, New York: I agree with David [Cohen] about the overemphasis on D2B and the associated confounders. As we moved from 120- to 90-min D2B, there was no associated drop in mortality.  The societal and financial cost of moving that needle is up for debate.
The societal and financial cost of moving that needle is up for debate.
Knowing the complete anatomy is essential, especially with the open question of when to treat non-culprit lesions. [There are] frequent anatomic surprises, so I prefer non-culprit imaging first. I believe in knowing the LVEDP and getting LV imaging before PCI can help assess mechanical issues that are invariably missed early. Does anyone even listen for a murmur anymore? Lastly, you can get a sense of where the patient is heading before the dwindles set in. I also agree with Steve Ramee’s triage approach.
Kirk Garratt, Newark, Delaware: Despite Nallamothu et al’s paper2, shaving off 10 minutes by choosing to do PCI before you know all the anatomy doesn’t mean your patient’s chances of survival go up 8%. The relationship, if any, between an operator’s approach (as outlined by Mort) and patient outcomes has never been measured, to my knowledge. I agree with the sentiment being expressed by others that not collecting all potentially important information to save a few minutes could lead to worse outcomes.
 I’ve thought a lot about the value of doing a ventriculogram and/or measuring the LVEDP before PCI. In the early years, this was standard practice. I stopped doing routine pre-PCI V-grams years ago because it was so rare to find something that changed my care plan (back then we auscultated the chest before starting the cath), and of course there was pressure to open the coronary occlusion quickly. Today, I’d say a V-gram is only indicated if a mechanical complication is suspected. In my hospital, it’s hard for STEMI patients to avoid an echo for more than a couple hours. Measuring the LVEDP before PCI isn’t helpful in most cases; the exception might be for doing fractional flow reserve (FFR) on a significant lesion in a non-infarct related artery where a high LVEDP might interfere with measurements. Measuring LVEDP after PCI is reasonable, but unless the patient is in — or developing — pulmonary edema, I can’t say I found that terribly useful, either. Of course, if the patient has shock or significant hemodynamic instability, then the LVEDP should be measured when mechanical circulatory support is started; a right heart cath should go in and measurements taken before the patient goes to the CICU.
I’ve thought a lot about the value of doing a ventriculogram and/or measuring the LVEDP before PCI. In the early years, this was standard practice. I stopped doing routine pre-PCI V-grams years ago because it was so rare to find something that changed my care plan (back then we auscultated the chest before starting the cath), and of course there was pressure to open the coronary occlusion quickly. Today, I’d say a V-gram is only indicated if a mechanical complication is suspected. In my hospital, it’s hard for STEMI patients to avoid an echo for more than a couple hours. Measuring the LVEDP before PCI isn’t helpful in most cases; the exception might be for doing fractional flow reserve (FFR) on a significant lesion in a non-infarct related artery where a high LVEDP might interfere with measurements. Measuring LVEDP after PCI is reasonable, but unless the patient is in — or developing — pulmonary edema, I can’t say I found that terribly useful, either. Of course, if the patient has shock or significant hemodynamic instability, then the LVEDP should be measured when mechanical circulatory support is started; a right heart cath should go in and measurements taken before the patient goes to the CICU.
 Mitchell Krucoff, Durham, North Carolina: Presuming radial access (femoral is for MCS as needed), I am in the Fred [Welt] camp: namely, if I suspect the RCA culprit, I take diagnostic pics of the left coronary artery (LCA) and a guide catheter to the RCA. My main agenda of the diagnostic LCA pictures is to understand left main and LAD lesions likely to precipitate shock or require urgent surgery, which may expedite adding MCS into the scenario and/or deferring PCI altogether.
Mitchell Krucoff, Durham, North Carolina: Presuming radial access (femoral is for MCS as needed), I am in the Fred [Welt] camp: namely, if I suspect the RCA culprit, I take diagnostic pics of the left coronary artery (LCA) and a guide catheter to the RCA. My main agenda of the diagnostic LCA pictures is to understand left main and LAD lesions likely to precipitate shock or require urgent surgery, which may expedite adding MCS into the scenario and/or deferring PCI altogether.
For an anterior MI, I take an extra backup (EBU) guide and fix the LAD, presuming the LM, left circumflex (LCx), or collaterals to the RCA don’t touch other buttons making me re-think PCI altogether. Either of the above, nasty surprises are avoided and timelines are the shortest possible.
Advocating for the shortest possible: Once the patient is in the lab, I think D2B times are more for administrators than patient survival or LV function. On the other hand, for patient comfort, relief of pain, and restoration of ability to breathe, 5-10 min (or 15, or 20, if your catheter to the non-IRA doesn’t fit well and you must try others…) may not seem long to the operator, but for the patient lying on the table, it can seem like an eternity.
 Dawn Abbott, Providence, Rhode Island: For the last 20 years in STEMI, I start with a guide to culprit artery with the exception of shock. Never had an issue with non-culprit disease. If diagnosis is not clear after angiography, no culprit identified, then I do a LV gram; otherwise LVEDP, and echo is standard.
Dawn Abbott, Providence, Rhode Island: For the last 20 years in STEMI, I start with a guide to culprit artery with the exception of shock. Never had an issue with non-culprit disease. If diagnosis is not clear after angiography, no culprit identified, then I do a LV gram; otherwise LVEDP, and echo is standard.
Lloyd Klein, Sonoma, California: Reading about all of the various approaches to basically save 5 minutes, maybe 10, has been intriguing. While D2B time in the larger picture is clearly important, I am skeptical that these very few moments are saving lives or even much myocardium. But it does give us a number to suggest our expertise in this realm. What we have here is a process indicator that has become a competition rather than any meaningful medical innovation. I know of no study that suggests that a D2B time of 40 minutes is superior to one of 50 minutes. And I think that Mitch’s point that only the administration really cares about the actual number is fundamentally true. For what it’s worth, I think knowing the anatomy of all 3 vessels will make a difference in the strategy with some patients.
I know of no study that suggests that a D2B time of 40 minutes is superior to one of 50 minutes. And I think that Mitch’s point that only the administration really cares about the actual number is fundamentally true. For what it’s worth, I think knowing the anatomy of all 3 vessels will make a difference in the strategy with some patients.
Timothy D. Henry, Cincinnati, Ohio: We will never have consensus on the issue [guide 1st or non-culprit 1st] because it is a style/comfort issue. My thoughts — THE SYSTEM matters — make sure your system is as good as it can get and continues to keep getting better. TIME matters — myocardium is dying. 
For the record, I have a plan based on the ECG and clinical history. I use a GUIDE-first approach and fix the culprit. But if something is unexpected, you can always take the guide out and do the non-culprit angiogram. I get an LVEDP asap, using the guide if possible. I always listen to the chest after the patient is on the table, especially in late STEMI presenters. My personal goal is always cath lab to device 10 min [MK: a metric unique to this team]. We pre-activate the cath lab from EMS notification in about 50% of our patients, bypassing the ED. All our transfers come straight to cath lab unless something unusual occurs. All our patients are pre-treated with ASA, ticagrelor, and heparin. I use cangrelor if I’m worried about oral absorption, cardiogenic shock, or cardiac arrest.
 James Blankenship, Albuquerque, New Mexico: A decade ago, I favored PCI immediately upon identifying the culprit, but the evidence, along with the embarrassment of mistaking a non-infarct vessel for a culprit vessel on a couple of occasions, convinced me that complete angiography first is better. I start with a diagnostic catheter for the presumed non-culprit artery, but don’t spend more than a few minutes looking for it, if it has an aberrant origin. Then the presumed culprit is cannulated with an appropriate guide. LVEDP is a valuable data point for anterior infarcts and is helpful for non-anterior Mis when it is unexpectedly high. The diagnostic JR4 can be used to check LVEDP before imaging the RCA in anterior infarcts and the JR4 guide can be dipped into the LV before cannulating the culprit in RCA infarcts. LV grams may be a generational thing; younger interventional colleagues seem to do them rarely. However, LV grams may be helpful particularly in cases where LV function is unexpectedly poor. Rarely have they provided an early tipoff to a major complication such as severe mitral regurgitation (which may not have a loud murmur) or even ventricular septal defect (in a case of age-uncertain inferior MI).
James Blankenship, Albuquerque, New Mexico: A decade ago, I favored PCI immediately upon identifying the culprit, but the evidence, along with the embarrassment of mistaking a non-infarct vessel for a culprit vessel on a couple of occasions, convinced me that complete angiography first is better. I start with a diagnostic catheter for the presumed non-culprit artery, but don’t spend more than a few minutes looking for it, if it has an aberrant origin. Then the presumed culprit is cannulated with an appropriate guide. LVEDP is a valuable data point for anterior infarcts and is helpful for non-anterior Mis when it is unexpectedly high. The diagnostic JR4 can be used to check LVEDP before imaging the RCA in anterior infarcts and the JR4 guide can be dipped into the LV before cannulating the culprit in RCA infarcts. LV grams may be a generational thing; younger interventional colleagues seem to do them rarely. However, LV grams may be helpful particularly in cases where LV function is unexpectedly poor. Rarely have they provided an early tipoff to a major complication such as severe mitral regurgitation (which may not have a loud murmur) or even ventricular septal defect (in a case of age-uncertain inferior MI).
 Chris White, New Orleans, Louisiana: The flaw in all of the D2B data is that it doesn’t account for the variable pre-hospital delay, which can be significant for some patients. Not everyone with a STEMI presents within minutes to the ED; some wait hours. Given that, there is no reason not to have complete anatomic information before an intervention is performed.
Chris White, New Orleans, Louisiana: The flaw in all of the D2B data is that it doesn’t account for the variable pre-hospital delay, which can be significant for some patients. Not everyone with a STEMI presents within minutes to the ED; some wait hours. Given that, there is no reason not to have complete anatomic information before an intervention is performed.
Duane Pinto, Boston, Massachusetts: I use Mitch [Krucoff’s] strategy. If the culprit lesion, based on ECG, is in the right coronary, then I shoot the LCA first because there may be something there that gives me pause.  If the culprit is on the left, then I shoot the left first with a guide because there is nothing in the RCA that will dissuade me from fixing the culprit lesion even if collaterals to the RCA are present on the left shot. Nevertheless, I always say to the fellow, “remind me to shoot the right” because after a hard case, it is easy to forget to shoot the right at the end. I improvise at times depending on the situation because if you can’t, you shouldn’t be an interventional cardiologist.
If the culprit is on the left, then I shoot the left first with a guide because there is nothing in the RCA that will dissuade me from fixing the culprit lesion even if collaterals to the RCA are present on the left shot. Nevertheless, I always say to the fellow, “remind me to shoot the right” because after a hard case, it is easy to forget to shoot the right at the end. I improvise at times depending on the situation because if you can’t, you shouldn’t be an interventional cardiologist.
I agree with Chris [White] to keep the goal in mind, which is myocardial salvage (mindful of Mitch’s points about how the patient feels) where 5-10 minutes to get difficult radial access or shoot a non-culprit artery is meaningless, especially if there is a long prehospital delay. I don’t really rush around and cut corners unless there is a reason to do so, and don’t forget that sometimes people get sicker before they get better when we open the artery. Ajay [Kirtane] looked at this, as did we,3,4 and showed that there is significant variation in the time-based benefit based on prehospital delay and culprit artery, reinforcing that the D2B of <90 min is for administrators and not cardiomyocytes.
The Bottom Line
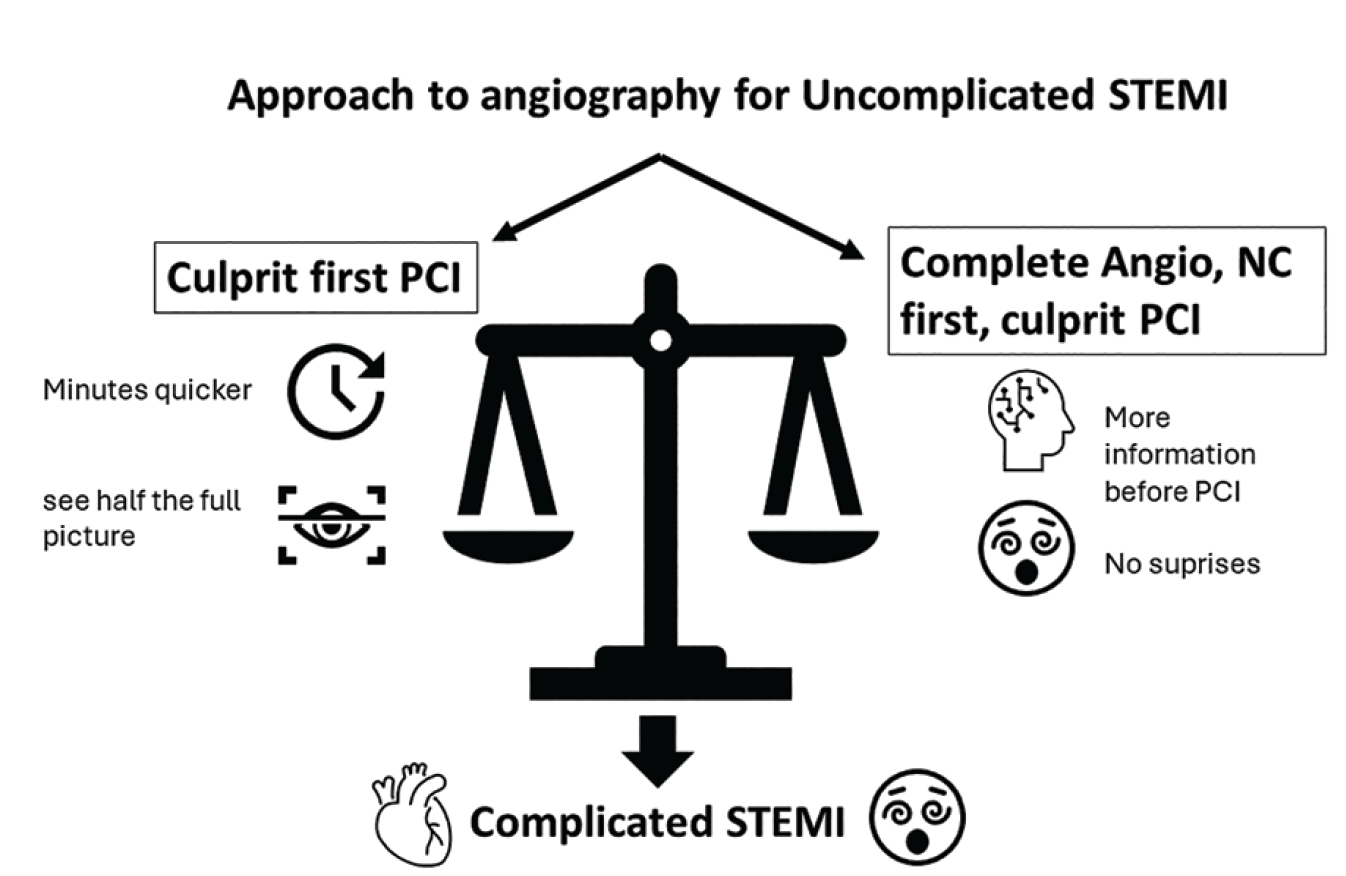
For the uncomplicated STEMI, our expert consensus seems to favor complete angiography of the non-culprit artery followed by culprit PCI (Figure). This approach gives a more complete picture at the expense of the 10 minutes that might be saved by the culprit PCI-first approach. Given the uncertain and often large window of ischemic time before entering medical care, the clinical outcomes are the same. Dr. Garratt summarized his view on LVEDP and use of LV grams in the uncomplicated STEMI patients and I agree that this information is not critical unless the patient’s clinical presentation has confounding features. Nonetheless, I think having more information is important should the uncomplicated STEMI become complicated.
Disclosures: Dr. Morton Kern reports he is a consultant for Abiomed, Abbott Vascular, Philips Volcano, ACIST Medical, and Opsens Inc.
Dr. Kern can be contacted at mortonkern2007@gmail.com
On Twitter @MortonKern
References
1. Levi N, Wolff R, Jubeh R, et al. Culprit lesion coronary intervention before complete angiography in ST-elevation myocardial infarction: a randomized clinical trial. JAMA Netw Open. 2024; 7(3): e243729. doi:10.1001/jamanetworkopen.2024.3729
[Quick Summary: STEMI patients were randomized to either culprit lesion PCI before complete coronary angiography or complete coronary angiography followed by culprit lesion PCI. 90 patients (48.9%) were randomized to undergo culprit lesion PCI before coronary angiography, and 94 (51.1%) were randomized to undergo coronary angiography followed by PCI. The culprit PCI group had shorter needle-to-balloon time (11.4 [5.9] vs 17.3 [13.3] minutes; P < .001). Rates of adverse events were similar between groups. In a subgroup analysis, the effect of culprit lesion PCI before complete coronary angiography on the primary outcome was consistent. There were no differences in rates of in-hospital, 30-day, and 1-year all-cause mortality.]
2. Nallamothu BK, Normand SLT, Wang Y, et al. Relation between door-to-balloon times and mortality after primary percutaneous coronary intervention over time: a retrospective study. Lancet. 2015; 385(9973): 1114-1122. doi:10.1016/S0140-6736(14)61932-2
3. Pinto DS, Frederick PD, Chakrabarti AK, Kirtane AJ, Ullman E, Dejam A, Miller DP, Henry TD, Gibson CM; National Registry of Myocardial Infarction Investigators. Benefit of transferring ST-segment-elevation myocardial infarction patients for percutaneous coronary intervention compared with administration of onsite fibrinolytic declines as delays increase. Circulation. 2011 Dec 6; 124(23): 2512-2521. doi:10.1161/CIRCULATIONAHA.111.018549
4. Chiang A, Gada H, Kodali SK, Lee MS, Jeremias A, Pinto DS, Bangalore S, Yeh RW, Henry TD, Lopez-Cruz G, Mehran R, Kirtane AJ. Procedural variation in the performance of primary percutaneous coronary intervention for ST-elevation myocardial infarction: a SCAI-based survey study of US interventional cardiologists. Catheter Cardiovasc Interv. 2014 Apr 1; 83(5): 721-726. doi:10.1002/ccd.25276
Find More:
Grand Rounds With Morton Kern, MD
The Latest Clinical & Industry News
Podcasts: Cath Lab Conversations
Cardiovascular Ambulatory Surgery Centers (ASCs) Topic Center
