


Comparison of Two Methods for Transradial Hemostasis After Cardiac Catheterization and Impact on Post-Procedure Efficiency
© 2024 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Cath Lab Digest or HMP Global, their employees, and affiliates.
Transradial access (TRA) for invasive cardiac catheterization procedures has increased over the last decade.1 According to the National Cardiovascular Data Registry, the practice of TRA for percutaneous coronary intervention procedures increased from 16.1% in 2012 to 53.7% in 2021.2 Despite this rapid increase in TRA utilization, the United States still lags behind other countries.3 Research has shown that use of radial access offers earlier mobilization, less risk of kidney injury, decreased mortality, and shortened length of stay as compared to the transfemoral approach.4
However, with TRA, there is a risk for radial artery occlusion (RAO), at 7.7% within 24 hours and 5.8% through 30 days.5 RAO, which is typically asymptomatic, can be the result of acute arterial thrombosis caused by use of a large-size catheter, lack of procedural anticoagulation, and prolonged duration of radial compression after sheath removal.6,7 Among the various strategies used to prevent RAO, recent data suggest that shorter clamp time in conjunction with the patent hemostasis technique significantly reduces the incidence of RAO.6 Care needs to be taken to balance the extent of reduced clamp application to minimize RAO risk without compromising hemostasis.6
Advances in radial compression device (RCD) and clinical practice standards, based on the RAVE trial8 at our institution, led to the implementation of a new standard of care in regard to achieving hemostasis in TRA patients for a select group of providers who adopted the change. Despite the RAVE trial results,8 there was variation in removal methods based on provider preference and variations in the literature.9 This prompted questions regarding best practice, safety, and efficacy for post-procedure care.
At our institution, the RCD is applied in the cardiac catheterization lab, then the patient is immediately transferred to a nursing floor (outpatient or inpatient, based on patient need) for RCD removal by trained nursing staff.
Prior to the practice change, a RCD alone was applied to the transradial site after TRA (Figure 1A). The RCD was removed 1-2 hours post procedure with varying success rates on first attempt. At the ordered removal time, the band was removed over 10-25 minutes based on the amount of air in the RCD. The nurse/cardiac procedure tech remained with the patient throughout the whole removal process.
The new practice standard, as prescribed by the RAVE trial,8 combines a hemostasis pad (SoftSeal-STF [Chitogen]) with short-term use of a RCD to achieve hemostasis in a shorter period of time (Figure 1B). The RCD remains in place for 30 minutes and then all the air in the RCD is gradually removed over 5 minutes, with the nurse/cardiac procedure tech staying with the patient throughout the process.

The current literature supports the clinical benefits of utilizing a hemostasis pad and RCD from the medical perspective,1,8 but a gap exists on how this change impacts post-procedure care outcomes, particularly RCD removal time, length of time to hemostasis, and time from procedure end to discharge (LOS). Our study, in addition to evaluating the above metrics, evaluated the documentation of site assessments and complications between groups.
Study Methods
Design. A retrospective observational cohort design was utilized to compare post-procedure outcomes for patients treated with a RCD alone (designated as Time 1[T1]) to patients treated with the RCD and SoftSeal-STF (designated as Time 2 [T2]). The study was approved and deemed exempt by the organization Institutional Review Board.
Setting and Sample. The sample included post radial access cardiac catheterization patients discharged the same day within a 40-bed same-day interventional procedure unit at a 938-bed quaternary medical center. During T1 (07/01/2021 – 12/31/2021), the radial band remained on the patient 1-2 hours, based on physician order. The RCD air was then removed at a rate of 5 cc every 5 minutes. When all the air was removed, the band remained on for an additional 5 minutes, followed by application of gauze and a transparent dressing. In the T2 period (01/01/2022 – 06/30/22), a SoftSeal-STF was applied with the radial band when the sheath was removed in the cath lab, with patients participating based on provider selection. The RCD remained on the patient for 30 minutes. All air was then removed gradually over 5 minutes. The band remained on without air for an additional 5 minutes, followed by application of gauze and a transparent dressing over the hemostasis pad.
Routine clinical standards of care were provided to both groups. Patient data was collected passively once care had been completed, with no additional interventions or screenings. Patients were excluded if they were admitted to an inpatient unit, had a femoral approach, had utilization of SoftSeal-STF and a radial band for other cardiac procedures, or required additional testing that prolonged normal discharge (ie, transesophageal echo, open heart surgery workup).
Procedures. Data were collected retrospectively from an electronic health record cardiac report that identified TRA patients who had cardiac catheterization/possible angioplasty during the designated time frames. Additional care and demographic variables were manually extracted from the electronic health record by members of the research team and included age, gender, body mass index, successful radial band removal on first attempt, access site assessment, reverse Barbeau at discharge, blood pressure, and sheath size. For clinical care variables manually abstracted, interrater reliability between data collectors was Cohen Kappa = 1.
Data management and analysis. Descriptive and inferential statistics were used to analyze the data using SPSS (Version 27). Sample characteristics were compared using independent sample t-tests for continuous variables and chi-square tests for categorical variables to evaluate if the samples were comparable. Mann-Whitney U, non-parametric testing, was used to test for differences between the T1 and T2 periods for radial band removal, time to hemostasis, and length of stay.
Results
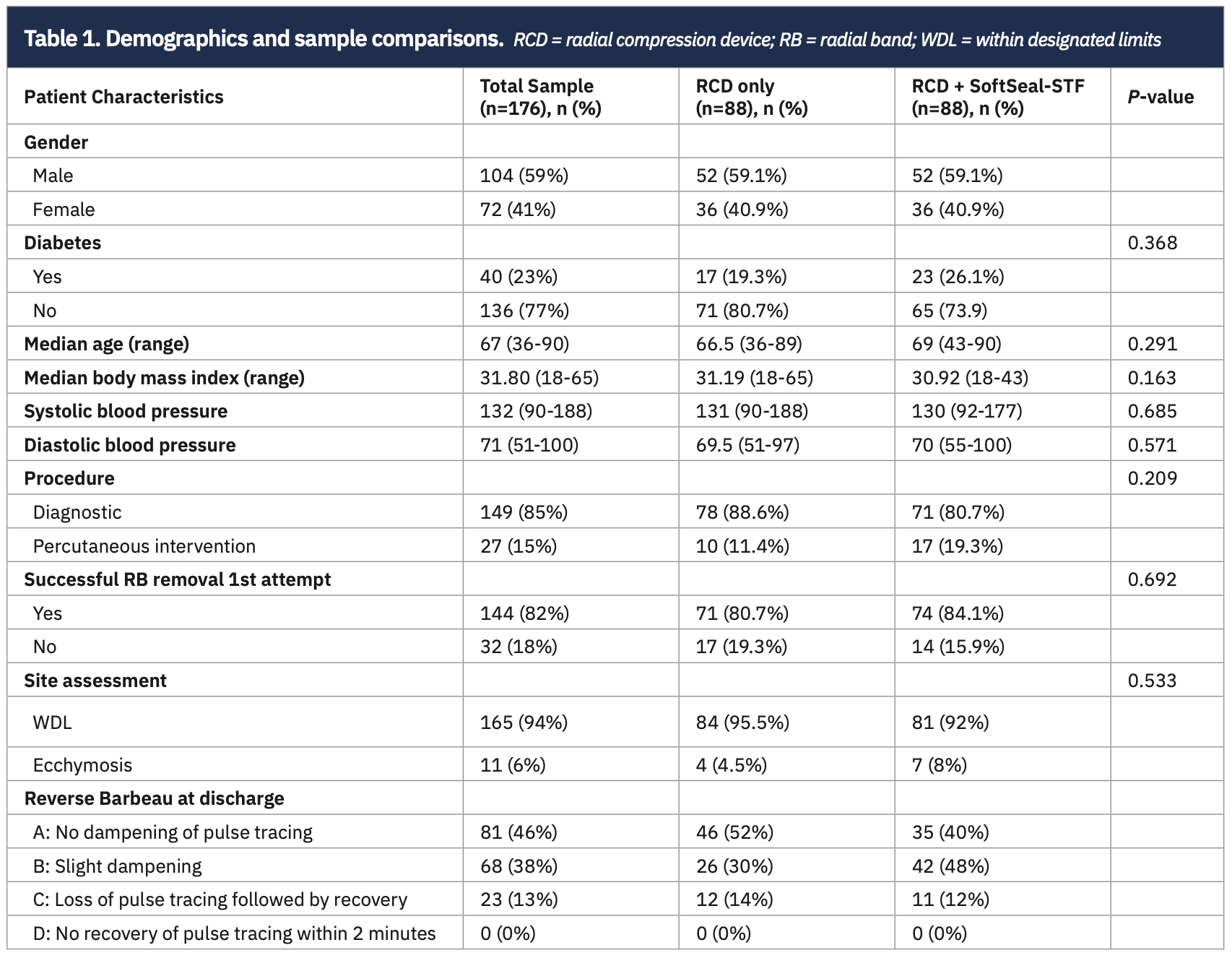
Demographics for total sample and comparison by group are shown in Table 1. All patients had a 6 French sheath and the TR Band (Terumo Interventional Systems) for their RCD. There were no differences between T1 and T2 period groups for all demographic variables. In T1, 88.6% (n=78) of cases were diagnostic catheterizations and 11.4% (n=10) were percutaneous intervention, with 79.5% (n=70) of the T1 group experiencing successful removal of the radial band on first attempt and 4.5% (n=4) with ecchymosis at the access site. In the T2 period, 80.7% (n=71) were diagnostic procedures and 19.3% (n=17) were percutaneous interventions, with 84.1% (n=74) experiencing successful removal of the radial band on first attempt and 8% (n=7) with ecchymosis at the access site.
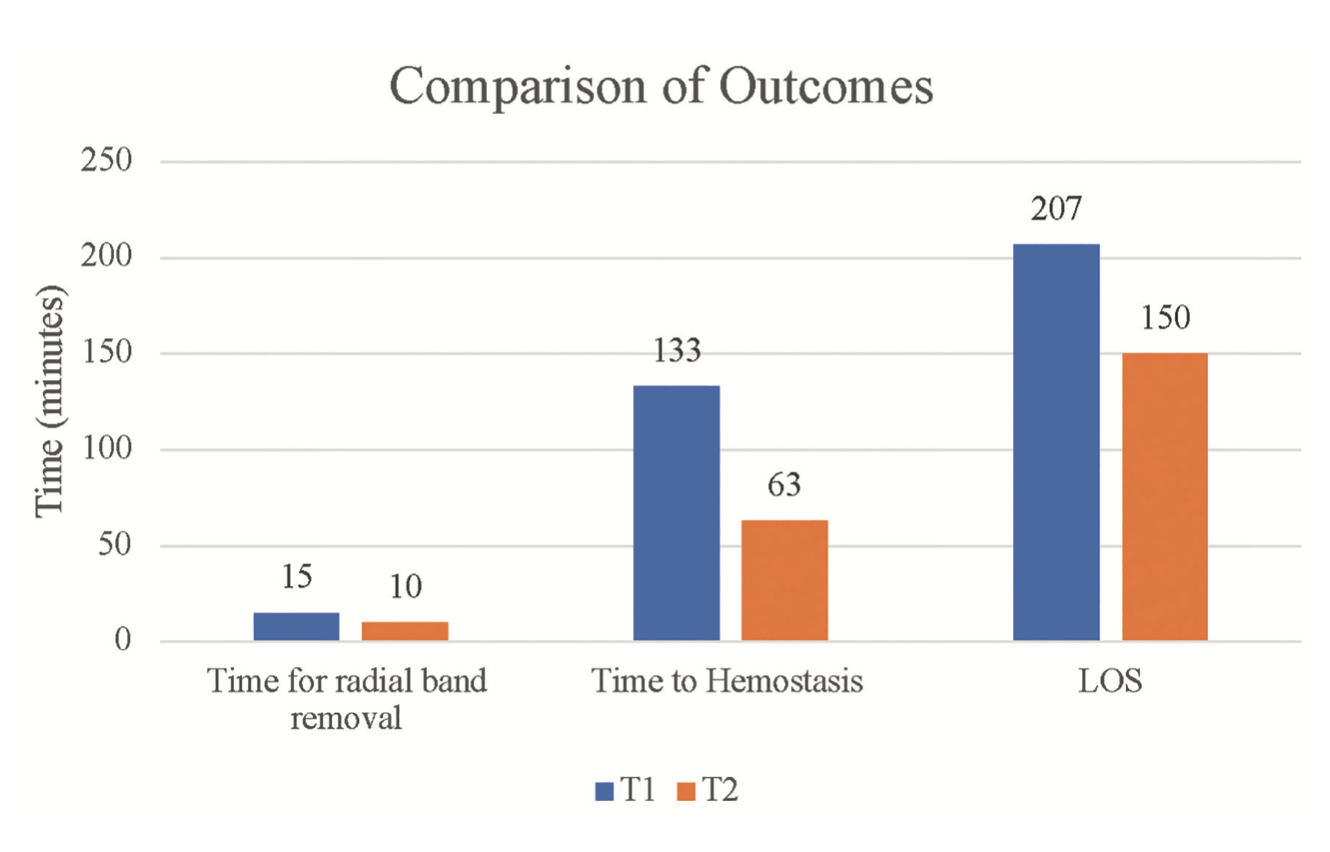
Mann-Whitney U test revealed a significant difference in the amount of time spent for radial band removal between groups (P<.001), length of stay (P<.001), and time to hemostasis (P<.01) (Figure 2). In the T2 group where post-procedure patients had a RCD and SoftSeal-STF the overall median times for patients were lower, including for nursing time with patient during radial band removal, time to hemostasis, and length of stay. A chi-square test for independence with Yates’ continuity correction (X2 [1, n=176]=.388, P=.533) indicated no significant association between group and access site complications.
The median time difference between groups was shorter in the T2 group (RCD and SoftSeal-STF) patients for radial band removal time (5 minutes), time to hemostasis (70 minutes), and length of stay (57 minutes) (Figure 2).
Discussion
While this is not the first study to demonstrate the positive impact of adding a hemostasis pad in addition to the use of a RCD,1,10 it has provided additional data to support a consistent method of RCD removal for our large, high-volume pre/post cardiac catheterization procedure care unit. Our study documented the value in time saved for both nursing staff and patients while maintaining patient safety. Time saved has been attributed to a potential nurse workload reduction, increased workflow efficiency, and bed flow availability. With our unit’s success, the method of adding a hemostasis pad in addition to the use of a RCD is also being used across the hospital on inpatient units. As the study results have been shared at cardiac-related meetings, future opportunities have been identified to support potential expansion of this technique to additional sites within our system.
Consistent use since implementation has continued to demonstrate favorable outcomes for our patient population. However, as Naranjo et al11 highlights, there is practice pattern variation in adoption of new percutaneous intervention techniques that can be affected by the patient, hospital, and operator. After the conclusion of the study, we extended the RCD plus SoftSeal-STF time to 60 minutes versus the study’s original 30 minutes, based on physician feedback and recommendations.
Like most practice changes, adherence did not happen overnight. It is pertinent to mention that the Same Day Interventional Services (SDIS) CNS and the Cath Lab Educator played instrumental roles as experts to impact clinical practice change across all the units and disciplines. Together, they continually assessed implementation strategies to ensure key stakeholders had the education, data, and resources necessary to ensure success. Information about the new process was presented at multiple venues and in multiple formats at the site to encourage buy-in from key physician and nursing stakeholders, and continued throughout the implementation period. Collaboration and teamwork across all units and disciplines was required to make this practice change a success.
Limitations include the fact that this study took place at a single site and had a retrospective design. There was potential for selection bias based on providers’ adoption of a practice change. Lastly, data are based on electronic health record documentation.
Conclusions and Implications
Post-procedure care for TRA with a RCD and SoftSeal-STF equates to post-procedure workload reduction, faster time to hemostasis, increased workflow efficiency, and decreased patient length of stay. This practice change has potential to positively influence both nurse and patient satisfaction. Future work is needed, with larger samples separating diagnostic and interventional TRA cases in order to determine if further differences exist. Additional opportunities to expand adoption of TRA also need to be explored.
Disclosures: The authors have no conflicts of interest to disclose regarding the content herein.
Jane Meitler, MSN, RN, ACNS-BC, CV-BC, can be contacted at jane.meitler@aah.org
References
1. Van Meter C, Vasudevan A, Cuccerre JM, et al. Time to discharge following diagnostic coronary procedures via transradial artery approach: a comparison of Terumo band and StatSeal hemostasis. Cardiovasc Revasc Med. 2018 Oct;19(7 Pt A):759-761. doi:10.1016/j.carrev.2018.03.009
2. Magee K. Radial access usage 2021 Q2. National Cardiovascular Data Registry Cath PCI registry. 2022; Advocate Aurora Health, Milwaukee, WI.
3. Mason PJ, Shah B, Tamis-Holland JE, et al. An update on radial artery access and best practices for transradial coronary angiography and intervention in acute coronary syndrome: a scientific statement from the American Heart Association. Circ Cardiovasc Interv. 2018;11(9):e000035. doi:10.1161/HCV.0000000000000035
4. Schussler JM, Vasudevan A, von Bose LJ, et al. Comparative efficacy of transradial versus transfemoral approach for coronary angiography and percutaneous coronary intervention. Am J Cardiol. 2016 Aug;118(4):482-488. doi:10.1016/j.amjcard.2016.05.038
5. Rashid M, Kwok CS, Pancholy S, et al. Radial artery occlusion after transradial interventions: a systematic review and meta-analysis. J Am Heart Assoc. 2016 Jan;5(1):e002686. doi:10.1161/JAHA.115.002686
6. Lavi S, Cheema A, Yadegari A, et al. Randomized trial of compression duration after transradial cardiac catheterization and intervention. J Am Heart Assoc. 2017 Feb 3;6(2):e005029. doi:10.1161/JAHA.116.005029
7. Pancholy SB, Bernat I, Bertrand OF, et al. Prevention of radial artery occlusion after transradial catheterization: the PROPHET-II randomized trial. JACC Cardiovasc Interv. 2016;9(19):1992-1999. doi:10.1016/j.jcin.2016.07.020
8. Jan MF, Walczak S, Dunaj W, et al. Radial artery vascular complications and resource utilization in subjects undergoing an angiogram/percutaneous coronary intervention: The RAVE trial. J Am Coll Cardiol. 2022 Mar, 79 (9_Supplement) 613. https://doi.org/10.1016/S0735-1097(22)01604-7
9. Maqsood MH, Pancholy S, Tuozzo KA, et al. Optimal hemostatic band duration after transradial angiography or intervention: insights from a mixed treatment comparison meta-analysis of randomized trials. Circ Cardiovasc Interv 2023;16(2):e012781 doi:10.1161/CIRCINTERVENTIONS.122.012781
10. Safirstein JG, Tehrani DM, Schussler JM, et al. Radial hemostasis is facilitated with a potassium ferrate hemostatic patch: the STAT2 trial. JACC Cardiovasc Interv. 2022;15(8):810-819. doi:10.1016/j.jcin.2021.12.030
11. Naranjo D, Doll J, Maynard C, et al. Practice pattern variation in adoption of new and evolving percutaneous coronary intervention procedures. J Interv Cardiol. 2023:2023:2488045. doi:10.1155/2023/2488045
Find More:
The Latest Clinical & Industry News
Grand Rounds With Morton Kern, MD


