


ACE-PROTAVI: Safety and Efficacy of Protamine in TAVI for Prevention of Bleeding Complications
On Monday, October 23, at the TCT 2023 meeting in San Francisco, California, Prof. Tony Walton presented “Routine versus selective protamine administration to reduce bleeding in transcatheter aortic valve implantation.” ACE-PROTAVI is an investigator-initiated, randomized, double-blind, placebo-controlled trial conducted by the ACE group, which includes the Alfred, Cabrini, and Epworth Hospitals in northern Australia.
The study was conducted to evaluate whether protamine, routinely used in cardiac surgery, could help in the reduction of procedural complications related to vascular access sites during TAVI. Risks around bleeding complications at vascular access sites include an increased length of stay, morbidity, and associated mortality. The trial sought to evaluate the safety and efficacy of protamine use on sheath removal in TAVI to reduce the risk of bleeding and vascular complications, where data have been limited thus far.
The trial was conducted at 3 large tertiary centers in Melbourne, Australia, with a 1:1 ratio between 2 groups. Exclusion criteria included a documented protamine allergy or anaphylaxis, a recent percutaneous coronary intervention (less than 3 months), and planned arterial access via a surgical cut-down. Patients were randomized to protamine versus placebo, and the operator was blinded as to what they were going to receive. Just prior to sheath removal, the protamine group received 1 mg/100 IU heparin to a maximum of 100 mg. Time to hemostasis after sheath removal was documented; if hemostasis was not achieved within 10 minutes, the operator could give the alternative agent from what the patient received (placebo if they had received protamine, and vice versa), remaining blinded. Hemostasis times were then documented.
The primary study endpoints were procedural hemostasis failure (failure to achieve hemostasis at the arterial access site, leading to alternative treatment, including FemoStop, endovascular balloon or stenting, or needing a surgical cut-down to repair the artery) and time to hemostasis (from large sheath removal to first observed and confirmed hemostasis, usually by digital subtraction angiography of the femoral artery). Secondary outcomes include a composite of all-cause death, major and minor bleeding and vascular complications at 30 days (VARC-2 criteria), transfusion for access-site related bleeding, major adverse cardiac events, length of stay post procedure, and delayed hemostasis failure.
ACE-PROTAVI enrolled 410 patients starting in December 2021, with no significant differences based on age or sex. There was a similar amount of peripheral arterial disease, sheath size was the same for both groups, heparin dosing was the same between both groups, and there was no difference between the peak activated clotting time (ACT) and the ACT prior to sheath removal.
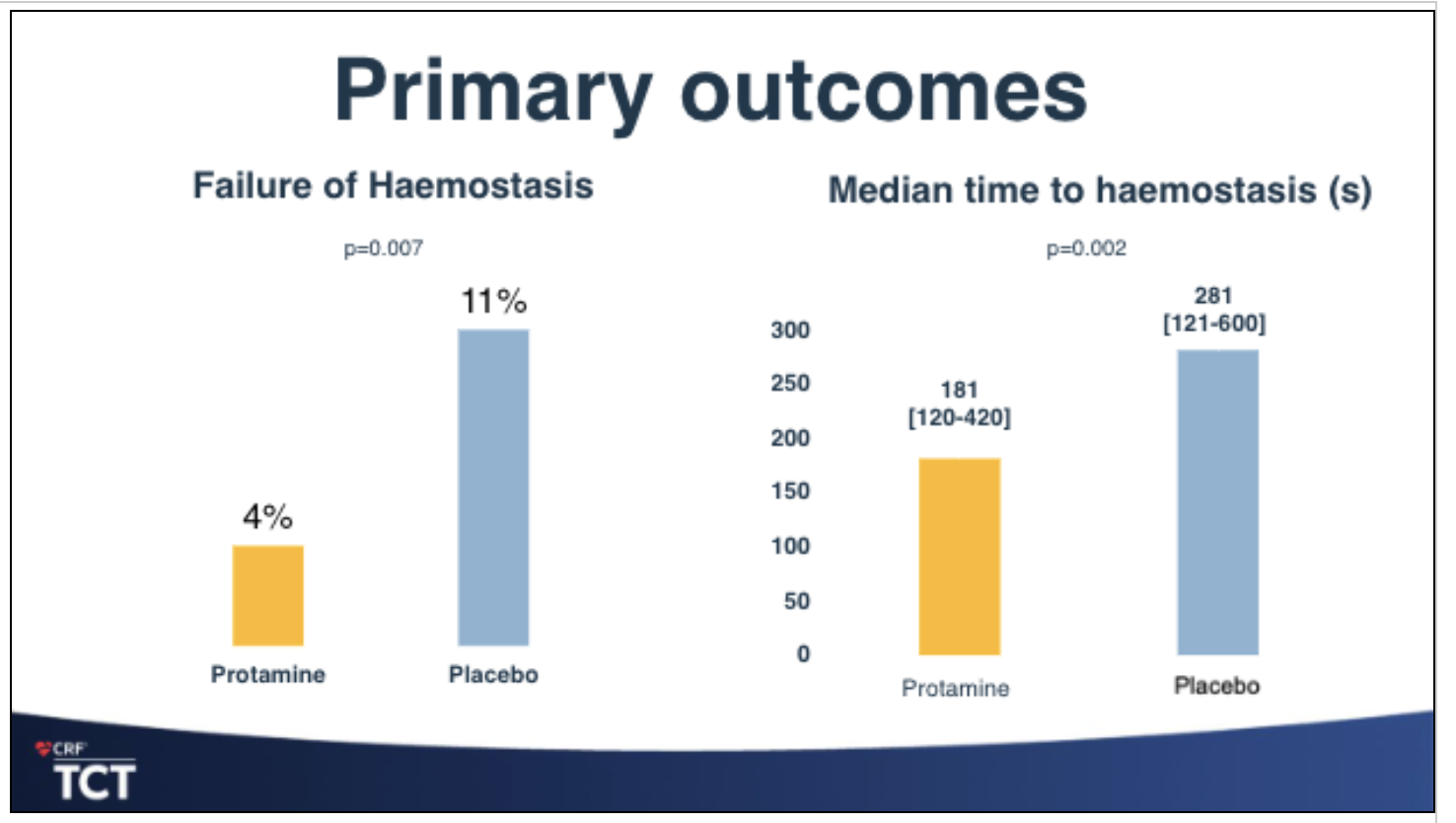 The primary outcomes of the study show “a substantial difference in the protamine group in terms of the failure of hemostasis,” said Prof. Walton. The protamine group had a 4% rate of failure versus the placebo group at 11%, and time to hemostasis “was also substantially reduced,” he noted, with a median 281 seconds for the placebo group versus a median reduction of 100 seconds less in the protamine group. For the secondary outcomes, the composite outcome was 5.2% with the protamine group versus 13% with placebo. “This was mostly driven by minor vascular complications,” said Prof. Walton. No difference was shown for major bleeding and major vascular complications. Hospital length of stay was slightly less for the protamine group. Failed delayed hemostasis was significantly lower for protamine (0.5% versus 6.5% with placebo, P<0.001). The administration of the second agent was also markedly reduced in the protamine group (5.2% versus 16.8% with placebo, P<0.001).
The primary outcomes of the study show “a substantial difference in the protamine group in terms of the failure of hemostasis,” said Prof. Walton. The protamine group had a 4% rate of failure versus the placebo group at 11%, and time to hemostasis “was also substantially reduced,” he noted, with a median 281 seconds for the placebo group versus a median reduction of 100 seconds less in the protamine group. For the secondary outcomes, the composite outcome was 5.2% with the protamine group versus 13% with placebo. “This was mostly driven by minor vascular complications,” said Prof. Walton. No difference was shown for major bleeding and major vascular complications. Hospital length of stay was slightly less for the protamine group. Failed delayed hemostasis was significantly lower for protamine (0.5% versus 6.5% with placebo, P<0.001). The administration of the second agent was also markedly reduced in the protamine group (5.2% versus 16.8% with placebo, P<0.001).
Key takeaways from the ACE-TAVI trial findings include: (1) protamine increases the rate of hemostasis success and offers a shorter time to hemostasis; (2) the trial showed a significant reduction in minor vascular complications; (3) protamine resulted in a slightly lower length of stay; (4) no adverse events were observed. “Our conclusion,” said Prof. Walton, “was that routine protamine administration should be considered in all patients undergoing TAVI, unless a recent coronary intervention has been performed.”
During the post-presentation discussion, it was noted that patients with a contraindication to protamine and heparin are usually considered as having a relative contraindication for cardiac surgery, likely to be similar for TAVI as well. From the surgical experience, a few tips for protamine were suggested, including if the ACT is on the higher side, do not give additional protamine, give the protamine only in the dosage of the baseline or the index heparin. Second, anaphylactic reactions are rare and can be fatal, but usually only occur in patients with recurrent administration of protamine. These patients usually require extracorporeal mechanical oxygenation (ECMO).
Prof. Anthony Walton, MBBS, FRACP, FCSANZ, presented “Routine versus selective protamine administration to reduce bleeding in transcatheter aortic valve implantation: ACE-PROTAVI” on Monday, October 23. His slides are available online here.
Keep reading about the latest in TAVR research:


