Education Survey Finds Providers Feel Unprepared

It turns out that EMS providers do not feel prepared. This article discusses the results of an effort to explore whether we are setting our providers up for success or failure and how we may need to reevaluate our teaching.
It was driven by a survey that looked at gaps in education and training and found our education may not be preparing EMS providers in ways that actually help them. As members of the Congress of Mobile
Medical Professionals,1 we created this national survey to look at the experiences of EMS and fire service providers, administrators, and educators to learn what is going well and what needs work.
The survey, approved by Marquette University’s Institutional Review Board, was shared on email lists and social media accounts and by directly contacting departments. Data collection spanned January 20, 2021 to March 6, 2021. More than 700 participants from 48 states, ranging from new providers to seasoned providers with more than 25 years’ experience, took the full survey. They represented nonprofit and for-profit agencies, fire-based and hospital-based systems, and government-operated and privately owned services.
Although the full survey had 56 questions, this article focuses on answers to one question: How prepared did participants feel after their initial training in 13 areas of prehospital medicine: chronic disease management, clinical reasoning, conflict resolution, cultural competencies, empathetic communication, implicit bias, independent thinking, medication adherence, medication reconciliation, report writing, social determinants of health, technical skills, and treatment planning?
These areas were identified as gaps in training and national standards by way of the recent NAEMSP statement that EMS should be teaching beyond technical skills.2 Paramedicine research confirms the need for nontechnical competencies,3 especially in the wake of the pandemic and public health emergencies. Other healthcare professions require proof of competency in “soft skills,” including communication, cultural competencies, and critical thinking. Yet these are absent from the National Model EMS Clinical Guidelines, which are focused on critical patient care and specific clinical scenario competencies and are not yet fully integrated into the National EMS Education Standards.
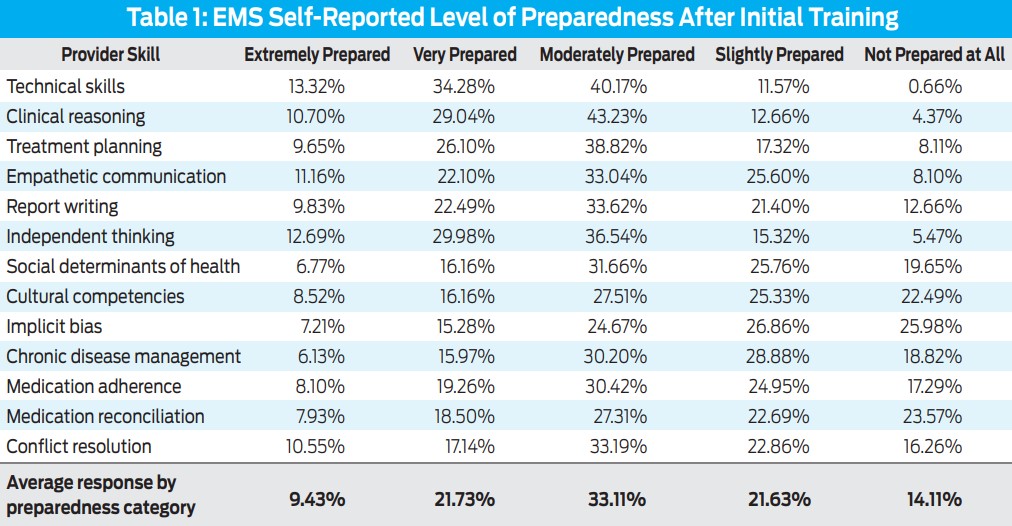
Participants ranked how prepared they felt in each area on a scale of 1–5, with 1 being “extremely prepared” and 5 being “not prepared at all.” A total of 458 participants answered this question, and their results are summarized in Table 1.
The More You Learn…
While 48% of all respondents felt prepared for technical skills, 69% reported feeling only moderately, slightly, or not at all prepared across the 13 areas of our question of interest.
As respondents’ level of education increased, their level of reported preparedness after initial training declined. Providers with secondary degrees reflected the epiphany that the more you learn, the more you realize you still have to learn. For example, 29% of respondents with high school diplomas felt unprepared for chronic disease management and social determinants of health, compared to 64% of medical directors, nurse practitioners, and other doctoral degree personnel.
Furthermore, 48% felt they were slightly or not prepared when surveyed about cultural competency, and 53% were slightly or not prepared in awareness of implicit bias. Evidence shows social determinants of health (SDOH),4 cultural competency,5 and implicit bias6 to be factors relevant to quality of care for the underserved that impact treatment options, health and lifestyle choices, and methods of communicating health information to patients.
We also found gaps and disconnects in areas where providers felt prepared but administrators and educators sometimes disagreed. For example, poorly written reports were a common pain point for administrators and educators, but 35% of street providers reported they were extremely or very prepared to write reports.
Less-experienced personnel reported higher levels of preparation than those with decades of service under their belts. Of respondents with more than 25 years of experience, 29% reported being very or extremely prepared for treatment planning, whereas 52% of those with 0–5 years’ experience reported the same. We identified the same trend in empathetic communication, independent thinking, clinical reasoning, and other areas.
Participants holding higher positions also said they felt slightly or not at all prepared in specific areas. This was evident in responses from leaders, including CEOs and chiefs. Of that group 85% reported feeling unprepared in chronic disease management, and 78% reported low levels of preparation in cultural competency. Educators also felt more unprepared than other participants, especially compared to street providers, in key areas.
Enough to Keep Up?
With the launch of Emergency Triage, Treat, and Transport (ET3),7 mobile integrated health (MIH), and community paramedicine (CP), the role of prehospital providers and the education they receive should be expanding. Nearly every MIH and CP program nationwide conducts medication reconciliation, but providers reported they aren’t being prepared to do so. Data shows that up to 87% of patients will have a medication discrepancy after hospital discharge.8 We need to get medication reconciliation right, yet 46% of MIH-CP respondents said they were only slightly or not at all prepared to handle this task.
Community paramedics reported feeling more prepared in empathetic communication. With 10% more CPs than other respondents reporting being at least moderately prepared in empathetic communication, this feels like a win. However, CPs also reported being no better trained or minimally more prepared than the general workforce in other areas highly relevant to their daily work, such as SDOH, treatment planning, cultural competencies, chronic disease management, and medication adherence.
As MIH-CP grows, patient care and accreditation standards are being developed, but is our current education enough?
7 Solutions to Try Today
1. Check in on your team and conduct your own internal assessment.
See how your own providers’ experiences align with our takeaways. Do your providers know what SDOH are? Some participants in this survey did not. Does your assessment of your providers’ preparedness align with how prepared they feel? Some participants reported feeling very prepared to write reports, while administrators disagreed based on the reports they read. Consider surveying your providers to see how their responses match up.
2. Use findings to inform training efforts.
For the industry as a whole, our findings raise big questions. Look at MIH-CP as an example. Does everyone in EMS need to be trained on medication reconciliation, or should that be specialized education for CPs? Do we need more buy-in from our providers to remove gaps in training, especially related to MIH-CP? What else are CPs excelling at that we can apply to the industry? Is empathetic communication the only skill set a CP uses in the field? What else needs to be changed in MIH and paramedicine education?
3. Look outside EMS, fire, and MIH-CP for teaching and training models.
Other industries can teach us how to improve training and education, including secondary and postsecondary education, educational and curricular policy, technical communication, and nursing and physician training. How do those and other industries teach? To what other industries can we look? What can we learn from them?
4. Bring in subject matter experts (SMEs) to teach where your educators lack experience, expertise, or training.
Historically EMS education comes from providers with varying degrees of experience. Especially in areas of cultural competency, these experiences can be very different based on geography and location. Agencies that bring in SMEs to augment the knowledge and skill sets of paramedics have demonstrated significant success in health outcomes and cost savings.9
5. Find the funding and resources necessary.
Empower your educators with resources and funding to bring training to the level you expect while focusing on what your community needs. Determine your team’s weaknesses, especially in the areas of writing and communication, disease management, medications, cultural competencies, and public health. Evidence shows MIH teams that have reallocated funding toward interprofessional personnel and advanced training skills6 had lower overall operating costs, reduced on-scene task costs, and reduced costs per minute.8 If we fail to allocate expertise and additional resources into EMS training curricula outside of technical skills, what does that cost us?
6. Teach the teachers.
In addition to bringing in SMEs to teach providers, curricular experts can teach your educators how to teach. For example, writing professors can show us how to teach writing effectively to adults,10 and education professors can teach us how to build curricula, lesson plans, and testing and evaluation, regardless of subject matter. Contact your local university’s colleges of education, nursing, health sciences, or arts and sciences to learn about training on curriculum development, which may even be available virtually.
7. Incorporate a culture of lifelong learning.
Who says you can’t teach an old dog new tricks? People can—and want to—learn; our survey confirms that. EMS is an evolving industry, and one way to keep providers prepared and confident is to teach them to expect to train continually and on more than technical skills. It’s not enough to learn new intubation methods; we need to train on new pharmacology, social and cultural competencies, and written communication skills too.5 Our providers deserve the best that education and training have to offer.
It’s time to align education with not just the technical skills but all the competencies we need and use every day. To that end, follow this study as we continue to dive further into findings and publish what we learn. Visit commp.org.
Authors’ note: This research and article were developed in collaboration with EMS industry experts Eric Chase, Anthony Correia, Mark A. Deavers, Stephen Norcup, and Michael Touchstone.
References
1. Congress of Mobile Medical Professionals. About the Congress of Mobile Medical Professionals (CoMMP). Congress of Mobile Medical Professionals. Accessed February 17, 2022. http://www.commp.org
2. Leggio WJ, Grawey T, Stilley J, Dorsett M. EMS curriculum should educate beyond a technical scope of practice: Position statement and resource document. Prehosp Emerg Care. 2021; 25(5): 724–9. doi: 10.1080/10903127.2021.1925793
3. Bennett R, Mehmed N, Williams B. Non-technical skills in paramedicine: A scoping review. Nursing and Health Sciences. 2021; 23(1): 40–52. doi: 10.1111/nhs.12765
4. Johnson RE, Cravens S. EMS improves community health by addressing social determinants. EMS World. Published June 19, 2020. www.hmpgloballearningnetwork.com/site/emsworld/article/1224499/ems-improves-community-health-addressing-social-determinants
5. Amato V. Cultural competence in EMS. EMS World. Published February 1, 2020. www.hmpgloballearningnetwork.com/site/emsworld/article/1223777/cultural-competence-ems
6. Taigman M. What EMS leaders need to know about unconscious bias. EMS1. Published January 5, 2019. https://www.ems1.com/paramedic-chief/articles/what-ems-leaders-need-to-know-about-unconscious-bias-EDdQljxvSCkZ9cVe/
7. Centers for Medicare & Medicaid Services. Emergency Triage, Treat, and Transport (ET3) Model. CMS.gov. Accessed February 17, 2022. https://innovation.cms.gov/innovation-models/et3
8. Graabæk T, Terkildsen BG, Lauritsen KE, Almarsdóttir AB. Frequency of undocumented medication discrepancies in discharge letters after hospitalization of older patients: a clinical record review study. Ther Adv Drug Saf. 2019; 10:2042098619858049. doi: 10.1177/2042098619858049
9. Reinhartz V, Sandoval I, Chagoya D, Peshek S. Incorporating pharmacists into mobile integrated health teams: A cost-benefit analysis. JEMS. Published August 11, 2020. https://www.jems.com/administration-and-leadership/community-paramedicine-and-mobile-health/incorporating-pharmacists-into-mobile-integrated-health-teams/
10. Angeli EL. Rhetorical Work in Emergency Medical Services: Communicating in the Unpredictable Workplace. Routledge; 2019
Elizabeth L. Angeli, PhD, is an associate professor of technical communication in the Department of English at Marquette University, Milwaukee, WI. Reach her at elizabeth.angeli@marquette.edu.
Victoria Reinhartz, PharmD, CPH, is a consultant pharmacist and chief executive officer for Mobile Health Consultants, Inc., Bradenton, Florida.
Sabrina Alahmad, MS, is a PharmD candidate in the class of 2023 at the Lake Erie College of Osteopathic Medicine School of Pharmacy, Bradenton, Florida.
Julia Jezykowski, BS, EMT, is a research assistant at Marquette University, Milwaukee, Wisconsin.