Evaluation of a Human Keratin Wound Matrix as an Effective Wound Healing Therapy in Difficult-to-Heal Venous Leg Ulcers
© 2023 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of ePlasty or HMP Global, their employees, and affiliates.
Questions
1. When are biomaterial matrices used in wound healing?
2. Which wound types could benefit from treatment with the human keratin matrix?
3. What clinical factors might impact human keratin matrix efficacy?
4. What are potential mechanisms of action of human keratin in wound healing?
Case Description
Six patients, both male and female, ages 42 to 84, with venous leg ulcers (VLUs) were selected and evaluated for a single-arm, single-center prospective quality analysis program between June 2018 and June 2019. The patients had between 1 and 3 chronic VLUs, with wound ages ranging from 2 months to 3 years. All patients had been assessed as having venous disease—obstructive or refluxing of the deep system—and had previously received ongoing standard wound care. In this investigation, we studied patient tolerance of an applied human keratin matrix (HKM) biomaterial (ProgenaMatrix, ProgenaCare Global LLC) and incidence of wound infection (or other adverse events) from the application of the HKM, as well as percent area wound closure at 4 weeks. At the initiation of the study period, HKM was applied to the wound bed, followed by a non-adherent dressing, Adaptic (Acelity), followed by a Biatain foam dressing (Coloplast), secured with a multilayered compression wrap. Wound characteristics were observed over 4 weekly follow-up visits: wound dimensions, wound bed appearance, and presence of periwound maceration. At each follow-up visit, HKM and multilayer compression wraps were reapplied to the targeted wound bed.
Q1. When are biomaterial matrices used in wound healing?
Wound care is a complex and varied practice that spans multiple medical specialties across multiple care settings. This is largely due to the numerous and varied causes of wounds. Wounds may arise from traumatic injury, surgical procedures, or secondary to conditions such as diabetes and vascular disease. In cases where wounds do not close even under clinical care, it can be thought the wound is “missing something” necessary for the healing process. To this end, therapies intended to assist and accelerate difficult wound healing commonly include the application of exogenous biomaterial protein matrices. The primary role of these products is to deliver materials theorized to be missing from the chronic wound—both physical and chemical. These materials can include various extracellular matrix (ECM) proteins, growth factors, or other molecules that may be dysregulated in wound healing.1
One previously understudied biomaterial to supply exogenously is keratin, a protein which is abundant in the epidermis. Keratin filaments in epidermal keratinocytes accumulate as a protective outer layer on the skin surface that is missing in wounds of any depth. Keratin provides mechanical strength to tissues due to its molecular structure, and is reported to play important roles in skin and wound biology.2 In addition to its structural properties, recent research found keratin also regulates epidermal keratinocyte growth and augments the innate immunity via antimicrobial peptides, both critical in chronically open wounds.3-4 It is also thought the human keratin in human keratin matrices (HKMs) may have more homology with the native skin structure than an animal-derived ECM such as decellularized submucosal tissues and could be more beneficial for human wound healing. Because of these reports, we sought to test the benefit of a novel HKM product in the treatment of chronic VLUs that otherwise would have received an ECM product.
Q2: Which wound types could benefit from treatment with the human keratin matrix?
Previous studies suggest venous ulcers that do not close by 40% after 4 weeks of compression are good candidates for the application of exogenous constructs to help them close.5 Wound closure can be delayed by many factors, including comorbid conditions that exacerbate wound etiology. In addition to chronic venous insufficiency, the 6 patients in this series suffered from comorbidities such as hypertension, hyperlipidemia, history of thromboses, and inflammatory conditions such as hepatitis C and asthma. One patient who was treated in this study had 2 recurrent wounds on the same leg.

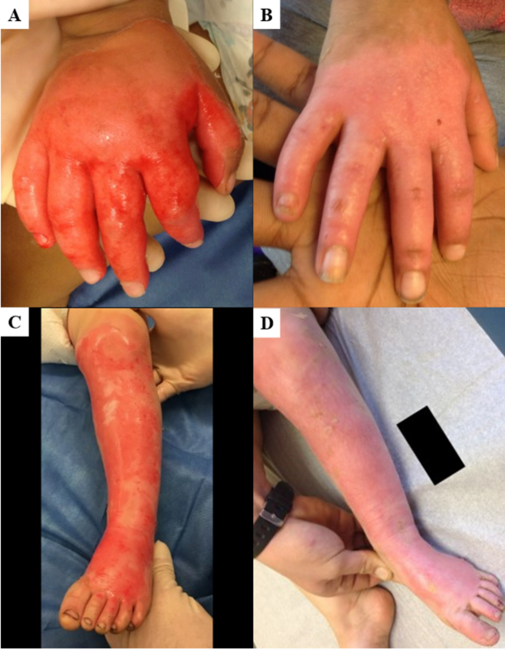
HKM, human keratin matrix; VLU, venous leg ulcer. Image contrast has been minimally manipulated to improve visualization.
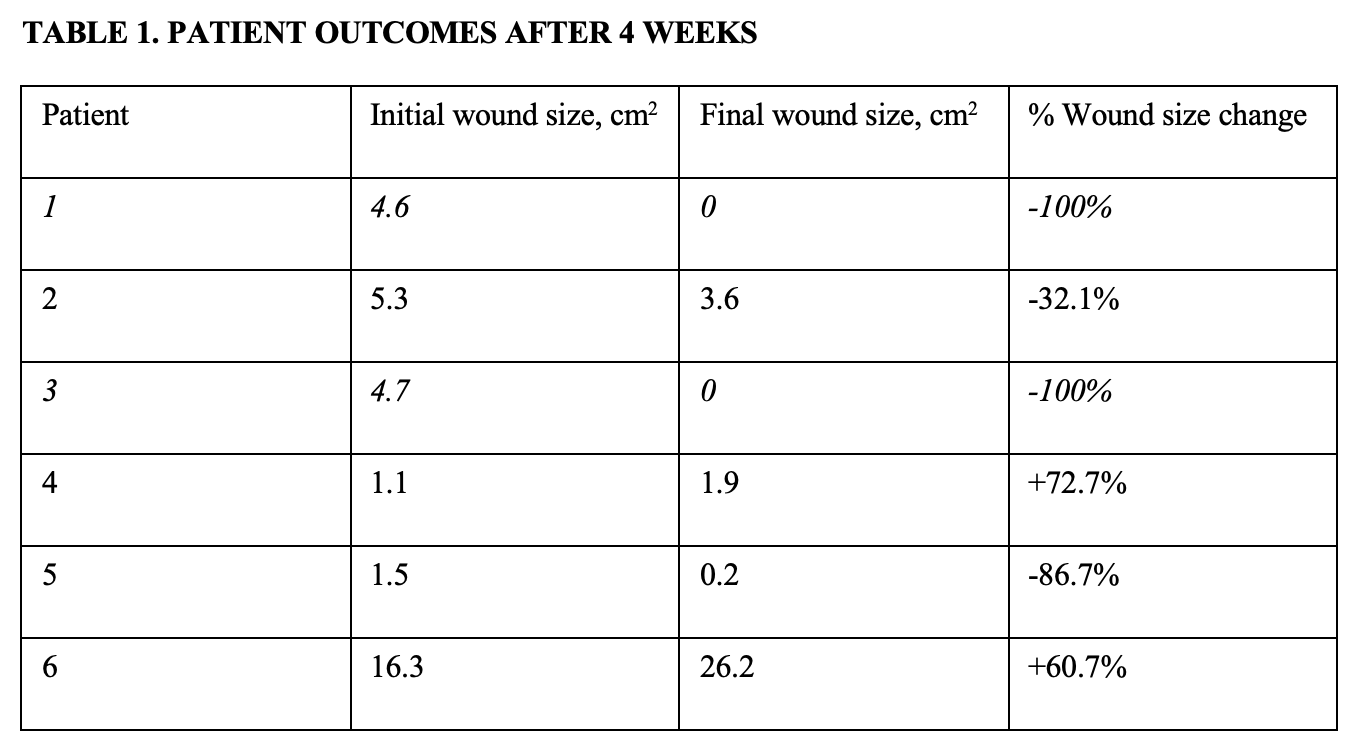
Two patients (33%) in our chronic VLU series, including the patient with multiple recurrent wounds, experienced 100% wound closure by the end of the 4-week treatment period (Figure 1). Overall, the median change in wound area after 4 weeks of HKM treatment was -59%, demonstrating an overall decrease in wound size (Table 1). No serious adverse events and no infections were observed during the treatment period. No maceration was observed in these patients, suggesting the moist HKM material is not detrimental to the periwound area. Indeed, HKM is designed to dry and elevate off the healed, non-exudative margins as the wound shrinks. One patient in this series found this material drying to be uncomfortable compared with other prior treatments: the only adverse event reported in this study.

Interestingly, 3 of the 6 patients presented with a wound bed with uniquely nodular characteristics (Figure 2) and increased granularity after HKM treatment. These patients had the highest rates of wound closure and healing, perhaps signaling a clinically relevant indicator of wound bed response to HKM. While our study was limited to 6 patients in a single center with chronic venous leg ulcers, other wound types such as diabetic foot ulcers, inflammatory ulcers, surgical dehiscences, and pressure ulcers may also benefit from HKM treatment.
Q3: What clinical factors might impact HKM efficacy?
All wounds were prepared with betadine, treated with local anesthetic, and sharply debrided prior to HKM application. Wounds were monitored during treatment for infection, but none was observed and no antibiotics were prescribed. Four wounds showed a reduction in wound size with HKM, including 2 fully healed patients (33%) (Figure 3). The mean VLU healing rate is 40% at 12 weeks.6 These preliminary results, including complete healing observed after only 4 weeks, suggest HKM is a promising novel treatment for VLUs.
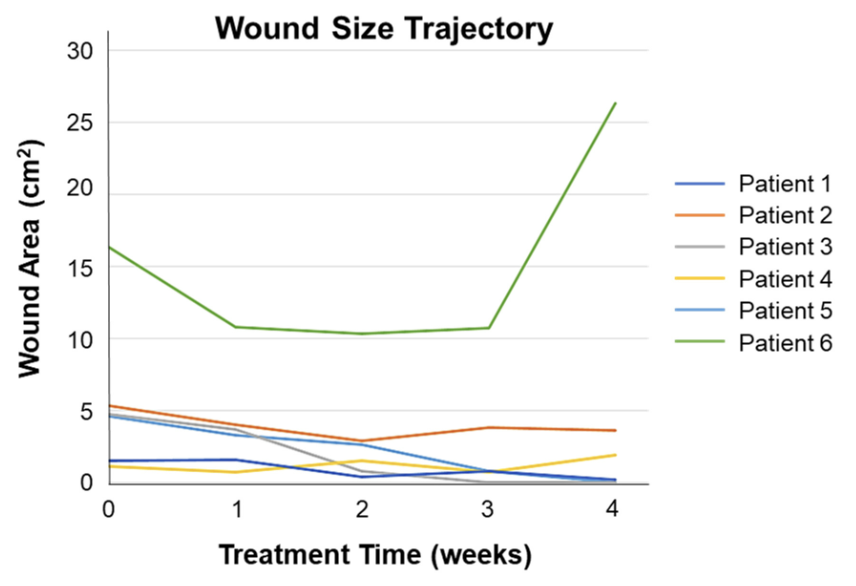
Two wounds increased in size during the 4-week follow up (Figure 3). However, both wounds were open >2 years and had very fibrotic wound beds. These 2 patients required additional surgical debridement. Lack of progress toward closure with HKM treatment in these patients may have been due to inadequate wound bed preparation. Debridement at the initiation of therapy was critical but was not routinely carried out after the first week. A recent study found proper debridement is the most important factor in wound closure at 12 weeks, followed by treatment with exogenous matrices.7 Future studies and use of HKM should include regular debridement to better evaluate the efficacy of keratin in chronic wound healing.

Handling of HKM was unique and less malleable than collagen-based materials, making it challenging to apply in deeper wounds and capable of fracture during wear (Figure 4). This is notable since direct physical contact with the wound is thought to be important to HKM efficacy. Additionally, insufficient wound moisture may cause HKM to become brittle and may negatively affect wound healing in general. Refinements to application techniques, such as the use of a bolstered dressing to ensure product contact and the application of moisture-managing hydrogels or secondary dressings, may help mitigate the impact of this product characteristic.
Q4: What are potential mechanisms of action of human keratin in wound healing?
There are a variety of possible mechanisms by which keratin may accelerate wound closure. Keratin proteins have demonstrated an ability to increase proliferation of fibroblasts, which are important for the formation of granulation tissue.8 Keratin has also been shown to stimulate keratinocyte activation and extracellular matrix production, both critical to wound closure.9
Other work has demonstrated that human keratin encourages the accumulation of a pro-regenerative subset of myeloid immune cells that promote cutaneous healing and inflammation resolution. Among other properties, keratin upregulates depleted inflammatory M1 macrophages and enriches the activated M2 phenotype with associated anti-inflammatory activity.10 A dysregulated inflammatory response is thought to be a key component in wound chronicity,11 and future work could investigate the role of HKM in the wound healing immune response.
Summary
In this first clinical assessment of a novel human keratin advanced wound care product, we applied HKM to patients with complex medical issues and difficult-to-heal venous leg wounds. These initial results, while from a small number of patients, include 2 patients achieving complete wound closure in 4 weeks and an overall average wound size decrease of over 30%. A good predictor of wound healing in VLUs is the wound size change within 4 weeks12—in this evaluation 3 of the 6 patients reached >50% wound healing in 4 weeks. These results suggest HKM may warrant further investigation as a novel treatment of VLUs and other chronic lower extremity wounds. In the wounds that did not show progress toward closure in this short study, we found that proper debridement is critical to support HKM wound healing. We hypothesize management of overall patient health as well as underlying comorbidities, such as vascular insufficiency, may also support healing in HKM-treated wounds. These factors will be incorporated into future randomized clinical trial protocols to evaluate the efficacy of HKM in treating these wounds.
Acknowledgments
Affiliations: 1Mount Sinai, Morningside Hospital, New York, New York; 2ProgenaCare Global, LLC, Marietta, Georgia
Correspondence: John Lantis II, MD; John.Lantis@mountsinai.org
Funding: No direct funding was received for this research; the human keratin matrix was provided free of charge.
Disclosures: Dr John Lantis has historically received fair market compensation for consulting projects related to keratin-based products. Dr Allison Ramey-Ward is a paid employee of ProgenaCare Global, LLC. The other authors disclose no relevant financial or nonfinancial interests.
References
1. Murphy PS, Evans GRD. Advances in wound healing: a review of current wound healing products. Plast Surg Int. 2012;2012:190436. doi:10.1155/2012/190436
2. Kelly R. Keratins in wound healing. In: Agren MS, ed. Wound Healing Biomaterials Vol. 2: Functional Biomaterials. Woodhead Publishing, 2016:353-365. doi:10.1016/b978-1-78242-456-7.00017-9
3. Kim S, Wong P, Coulombe PA. A keratin cytoskeletal protein regulates protein synthesis and epithelial cell growth. Nature. 2006;441:362-365. doi:10.1038/nature04659.
4. Lee JTY, Wang G, Tam YT, Tam C. Membrane-active epithelial keratin 6A fragments (KAMPs) are unique human antimicrobial peptides with a non-αβ structure. Front Microbiol. 2016;7:1799. doi:10.3389/fmicb.2016.01799
5. Kimmel HM, Robin AL. An evidence-based algorithm for treating venous leg ulcers utilizing the Cochrane database of systematic reviews. Wounds. 2013;25(9):242-250.
6. Fife CE, Eckert KA, Carter MJ. Publicly reported wound healing rates: the fantasy and the reality. Adv Wound Care. 2018;7(3):77-94. doi:10.1089/wound.2017.0743
7. Tettelbach WH, Cazzell SM, Hubbs B, De Jong JL, Forsyth RA, Reyzelman AM. The influence of adequate debridement and placental-derived allografts on diabetic foot ulcers. J Wound Care. 2022;31(9):S16-S26.
8. Werner S, Krieg T, Smola H. Keratinocyte–fibroblast interactions in wound healing. J Invest Derm. 2007;127(5):998-1008. doi:10.1038/sj.jid.5700786
9. Tang J, Sierra JO, Kelly R, Kirsner RS, Li J. Wool-derived keratin stimulates human keratinocyte migration and types IV and VII collagen expression. Exp Dermatol. 2012;21(6):458-460.
10. Fearing BV, Van Dyke ME. In vitro response of macrophage polarization to a keratin biomaterial. Acta Biomater. 2014;10(7):3136-3144. doi:10.1016/j.actbio.2014.04.003
11. Pastar I, Balukoff NC, Marjanovic J, Chen VY, Stone RC, Tomic-Canic M. Molecular pathophysiology of chronic wounds: current state and future directions. Cold Spring Harb Perpect Biol. 2022:a041243. doi:10.1101/cshperspect.a041243
12. Kurd SK, Hoffstad OJ, Bilker WB, Margolis DJ. Evaluation of the use of prognostic information for the care of individuals with venous leg ulcers or diabetic neuropathic foot ulcers. Wound Repair Regen. 2009;17(3):318-325.