Head and Neck Wound Reconstruction Using Biodegradable Temporizing Matrix Versus Collagen-Chondroitin Silicone Bilayer
Abstract
Background. Head and neck reconstruction is challenging because of the functional requirements of movement, sensation, and cosmesis of this highly visible region. This study is the first to compare Novosorb biodegradable temporizing matrix (BTM) and Integra collagen-chondroitin silicone (CCS) skin substitutes for reconstruction of soft tissue head and neck wounds.
Methods. This retrospective review included adults who underwent wound reconstruction of the head/neck with either BTM or CCS between 2015 and 2020. Patient-level data, complications, and closure rates were compared.
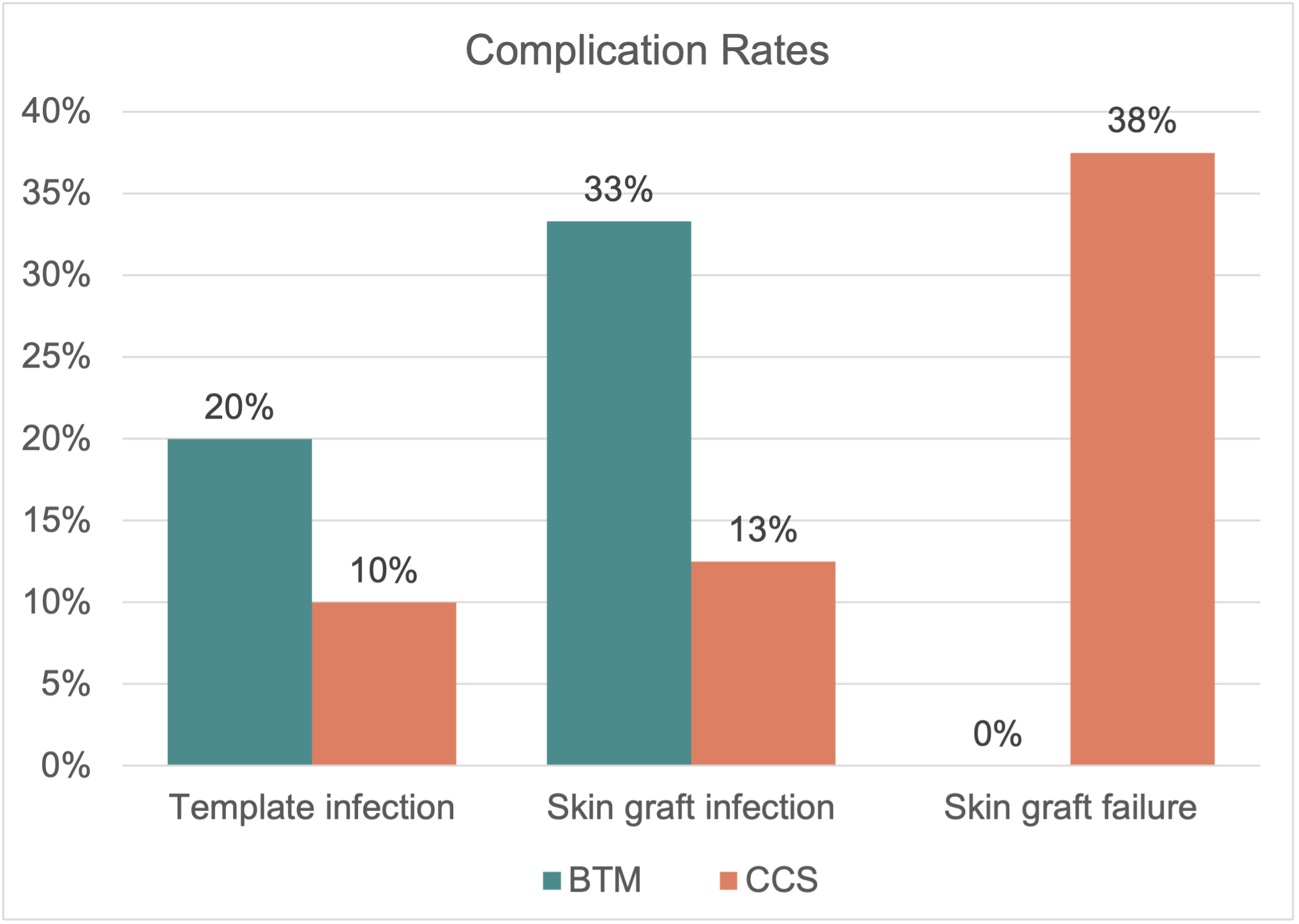
Results. The review identified 15 patients: 5 who received BTM and 10 who received CCS. Mean age at dermal template placement was 55 (range, 28-79) years. Race, sex, smoking status, medical comorbidities, defect size, radiation history, prior surgeries, and follow-up time were not significantly different between groups. Wound etiologies for BTM and CCS included burn (40% vs 60%), trauma (20% vs 20%), surgical wounds (20% vs 20%), and skin cancer (20% vs 0%), respectively (P = .026). Skin grafts were placed in 8 (80%) wounds after CCS placement, compared with 3 (60%) after BTM (P = .670). Template reapplication was required in 2 (40%) BTM wounds and 3 (30%) CCS wounds (P = 1.0). Infection, hematoma, and seroma were comparable between groups, although skin graft failure was higher in the CCS group at 3 (37.5%) compared with 0 for BTM (P = .506). More secondary procedures were required after CCS placement (CCS, 1.9 ± 2.2; BTM, 0.9 ± 0.8; P = .090). Definitive closure in patients not lost to follow-up occurred in 4 (100%) BTM and 6 (75%) CCS cases (P = 1.0).
Conclusions. Head and neck wounds treated with BTM had comparable closure and complication rates as CCS bilayer and required fewer secondary procedures and skin grafts. These findings suggest that BTM is safe and efficacious for application in head and neck wounds and may be considered as an economical alternative.
Introduction
Complex head and neck wounds can be difficult to reconstruct given the high functional and aesthetic requirements of this anatomic region. Wound reconstruction options include primary closure, skin grafting, local tissue rearrangement, or free tissue transfer. Wounds that are contaminated or lack a vascularized wound bed are not amenable to skin grafting and more complex reconstructive options, which can be complicated by longer operative times and may require patient comorbidities.1 Alternatively, these wounds can be covered with one of several commercially available skin substitutes that are often designed with biological and nonbiological components that act as scaffolding for wound regeneration and subsequent skin grafting. Integra collagen-chondroitin silicone (CCS) bilayer (Integra LifeSciences Corp) is the gold-standard skin substitute and has been widely used for decades,2–4 with reports demonstrating its success in head and neck wounds.5–7 However, its animal-derived components and slow production drive costliness and infection rates; therefore, other skin substitutes continue to be explored. Novosorb biodegradable temporizing matrix (BTM, PolyNovo Ltd) is a recently developed skin substitute comprising synthetic polyurethane foam and a temporary nonbiodegradable polyurethane seal.8 Histological studies have shown that new tissue integrates into the foam through vascularization to form a neodermis,9 and case series in humans have highlighted its successful wound healing properties.10–16 This is the first study to compare BTM and CCS in the reconstruction of soft tissue head and neck wounds.
Methods and Materials
This retrospective study included adults who underwent wound reconstruction of the head and/or neck, with either BTM or CCS bilayer between January 1, 2015, and August 31, 2020, at a level 1 trauma center. Patients were excluded if they were under 18 years of age at time of dermal template placement, received application of multiple or other skin substitutes, or if the wound was not in the head/neck region. Surgeon preference dictated selection of dermal template based on wound and patient features. Patients were identified by searching current procedure terminology codes for skin substitutes.
Demographics, comorbidities, wound characteristics, and operative details were recorded from the electronic medical record. The primary outcome was complete wound healing, defined as 100% re-epithelialization of the wound at any postoperative follow-up visit. Secondary outcomes included infection (ie, oral or intravenous antibiotic requirement, positive wound culture, or clinical signs such as purulence), graft or template failure, time to complete healing, number of skin grafts needed, and number of reoperations. Graft or template failure was defined by permanent removal and replacement. Time to complete healing was achieved if evidence of a healed wound was recorded at a postoperative follow-up visit.
Statistical Methods
Categorical factors were described with frequencies and percentages. Normality of continuous measures was determined by the Shapiro-Wilk test; parametric variables were summarized with means and SD, and nonparametric variables were summarized with median and interquartile range (IQR). Categorical variables were compared using the Fisher exact test and chi-square test where appropriate. Continuous variables (eg, age, body mass index, time to skin grafting, time to closure) were compared using 2-sample t tests. All analyses were performed on R software (v4.1.1) with P values < .05 considered statistically significant.
Results
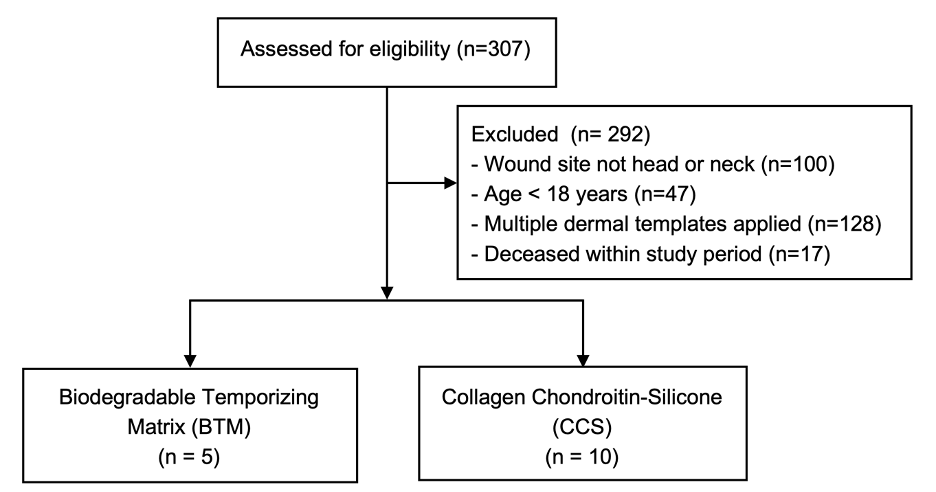
Of the 15 patients who met the inclusion criteria, 5 (33.3%) were treated with BTM and 10 (66.6%) with CCS (Figure 1). Table 1 summarizes the demographic and treatment characteristics. Mean (SD) age at template placement was 66.0 (12.8) years in the BTM group and 49.5 (11.7) years in the CCS group (P = .044); all other comorbidities were not significantly different. Among the 15 patients, 1 (7.1%) had prior radiation history to the surgical site. Median (IQR) follow-up time was 15.3 (3.8-26.8) months in the CCS group and 8.4 (6.8-8.4) months in the BTM group (P = .594). There were 2 (20.0%) CCS wounds and 1 (20.0%) BTM wound lost to follow-up (P = 1.0). All burns were full-thickness injuries, and most burns were treated with CCS (n = 6, 60.0%) rather than BTM (n = 2, 40.0%). All BTM cases were applied by plastic surgeons, whereas CCS wounds were applied by both plastic surgeons and burn surgeons. Median (IQR) wound area was 213 (190-369) cm2 for BTM and 193 (73-265) cm2 for CCS (P = .670). Exposed bone was present in 1 wound treated with CCS and skin grafting; the patient achieved wound healing on postoperative day 28.
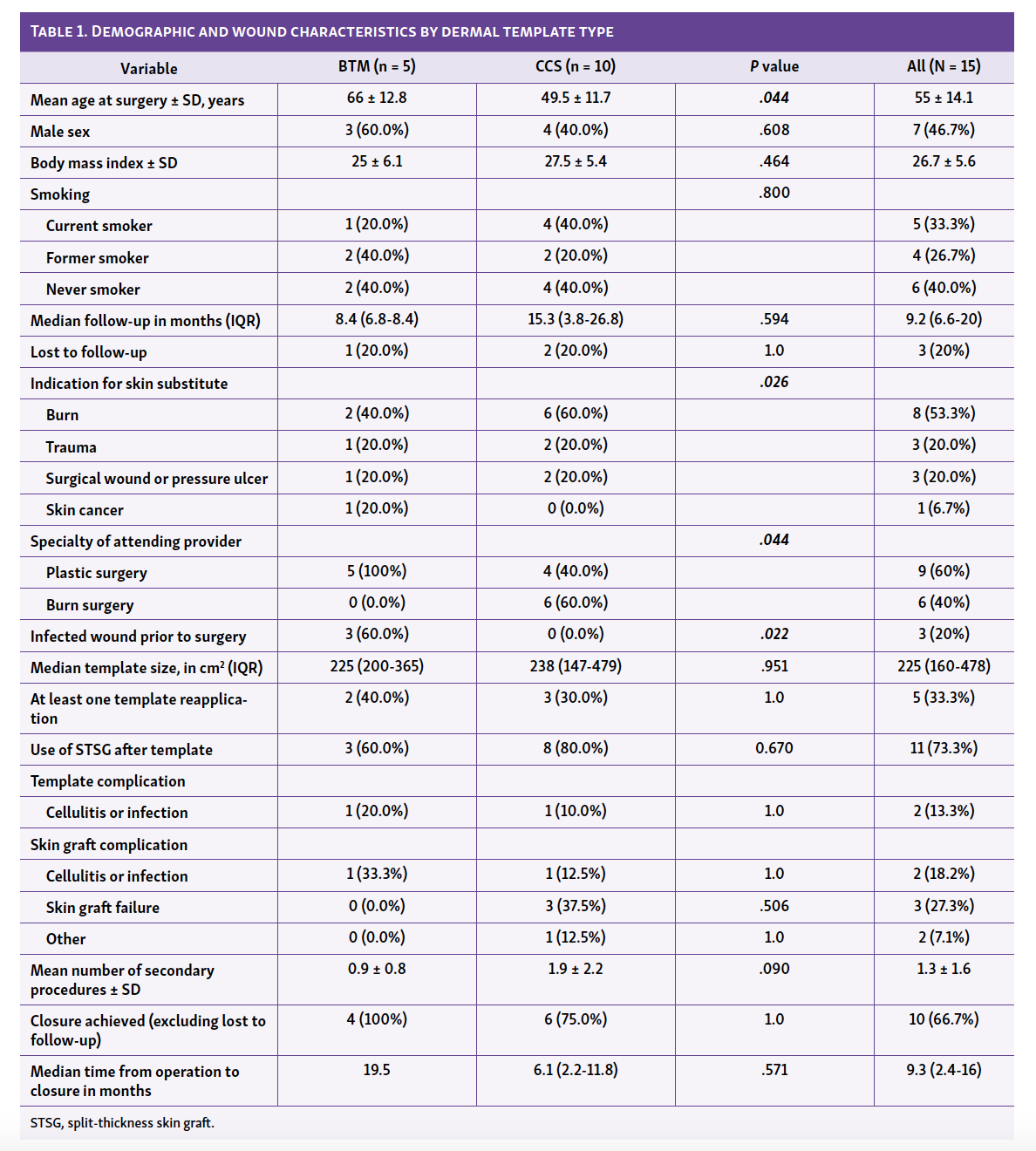
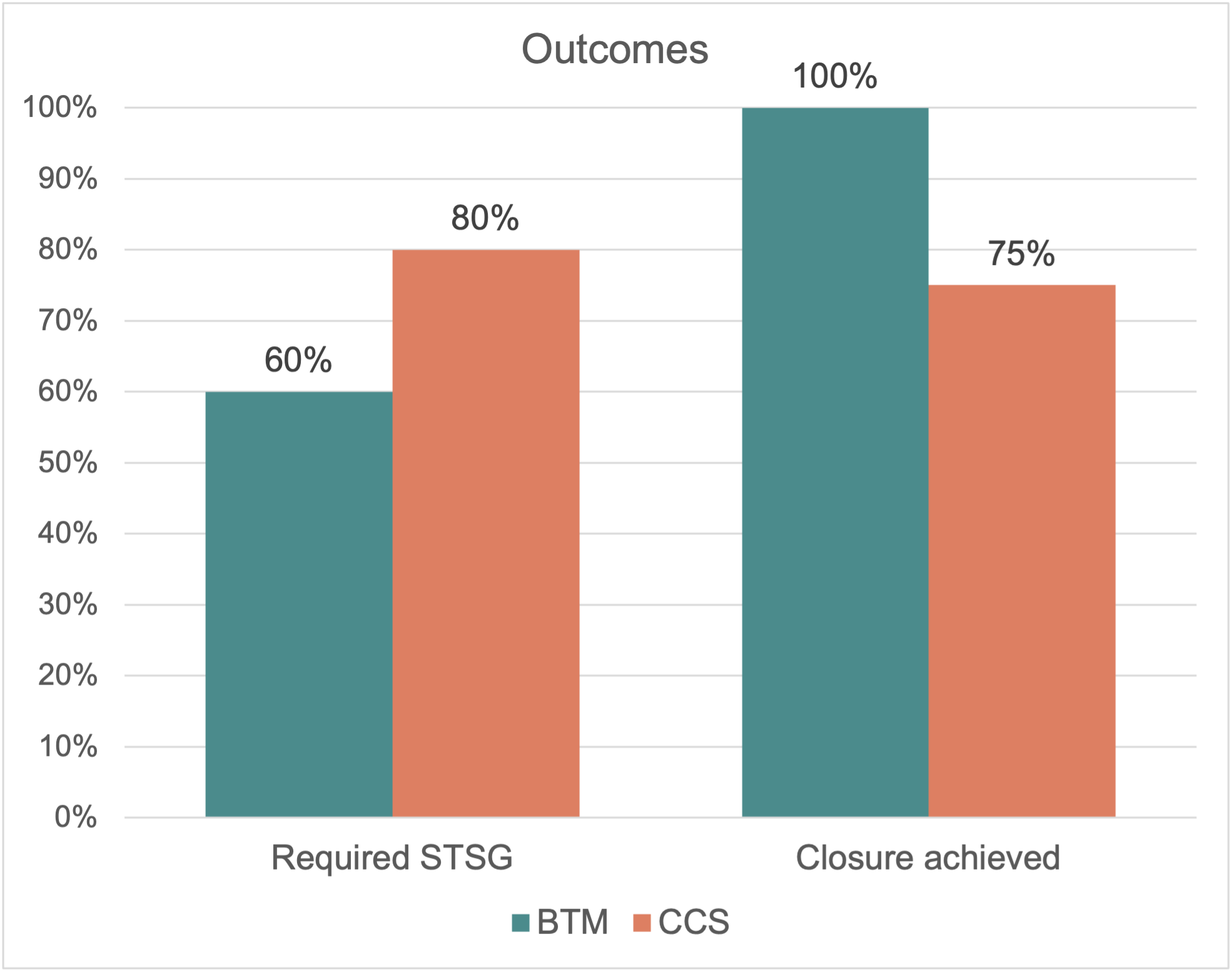
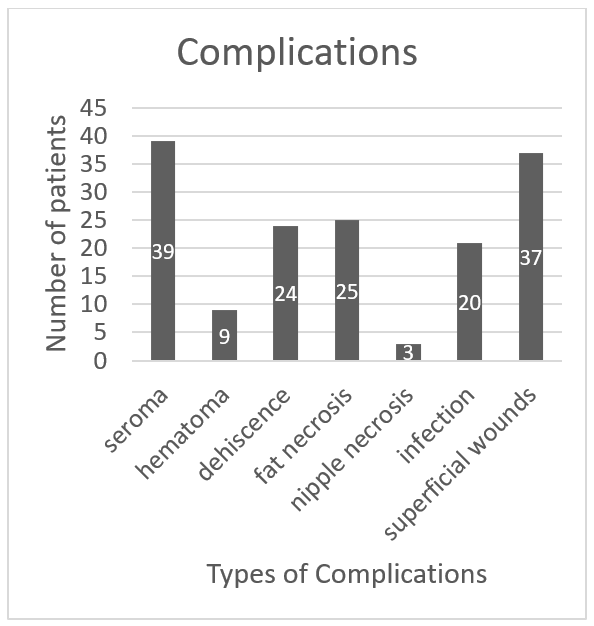
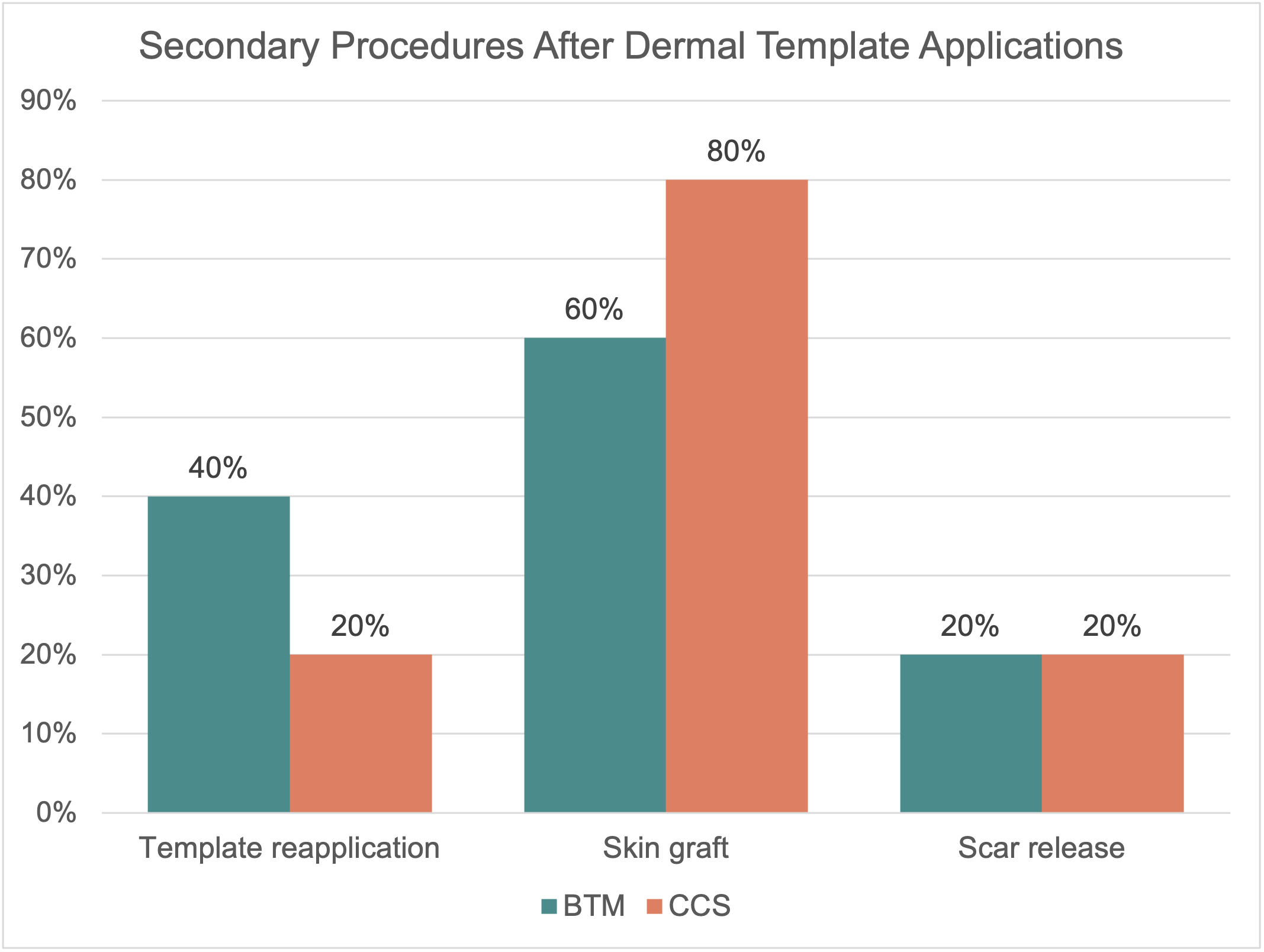
Median (IQR) template size was similar between groups, at 238 (147-479) cm2 for CCS and 225 (200-365) cm2 for BTM (P = .951). Template reapplication was required in 3 (30%) CCS and 2 (40%) BTM wounds (P = 1.0). Skin grafts were required in 3 (60%) BTM group patients compared with 8 (80%) CCS group patients (P = .560; Figure 2). Despite similar wound and template sizes, size of the skin graft was smaller for those in the BTM group (P = .776). Median (IQR) time to skin grafting was longer in the BTM group at 39 (30-72) days compared with 18 (14-21) days in the CCS group (P = .050). Mean number of skin grafts after template placement was lower in the BTM group than in the CCS group (0.3 vs 0.5, P = .724). There were 2 CCS-treated wounds (480 and 6 cm2) and 1 BTM-treated wound (200 cm2) that did not undergo skin grafting and healed secondarily, and the remaining BTM wound was lost to follow-up. Template complications occurred in 1 (10.0%) CCS and 2 (40.0%) BTM wounds (P = .242; Figure 3). Evidence of cellulitis or skin infection was present on 1 BTM wound and 1 CSS wound, and 1 BTM wound had inadequate coverage. Skin graft complications occurred in 5 (50.0%) of the CCS wounds and 1 (20.0%) of the BTM wounds (P = 1.0). These included 1 infection, 1 contracture, and 3 skin graft failures in the CCS group, we well as 1 infection in the BTM group.
CCS wounds required a mean of 0.9 (range, 0-6) secondary procedures, whereas BTM wounds required a mean of 1.9 (range, 0-4) secondary procedures following template placement (P = .090). Secondary procedures were most commonly subsequent skin grafting (Figure 4). Of the patients with adequate follow-up time, complete wound healing was attained in 6 of 8 (75.0%) CCS cases and 4 of 4 (100.0%) BTM cases (P = 1.0).
Discussion

Complex head and neck wounds pose a unique challenge to plastic and reconstructive surgeons due to the aesthetic and functional requirements, mechanism of injury, and reconstructive options available. Traditional reconstructive techniques, including use of primary closure, skin grafting, loco-regional flaps, and free tissue transfer, achieve varying degrees of functional and aesthetic results. However, they are all impacted by disadvantages including limited donor site availability,17,18 poor matching of skin tone or texture, or lengthy complex procedures and associated donor site morbidity.19 Therefore, dermal templates that can create a wound bed acceptable for skin grafting and achieve acceptable results in matching patient skin characteristics and positive outcomes can limit the disadvantages after other alternative reconstructive options.5 The Integra CCS bilayer is the current standard dermal substitute and has demonstrated well-established reliable outcomes for head and neck reconstructive surgeries.5–7 However, high cost and infection rates are known disadvantages of CCS. We compared CCS with a newly developed dermal substitute, Novosorb BTM. This is the first report to compare CCS with an alternate dermal substitute in the reconstruction of soft tissue head and neck wounds.
Compared with CCS, BTM is a completely synthetic skin substitute comprised of polyurethane that is ready for application directly from packaging and is easier to handle and secure to the surrounding soft tissue secondary to the tensile strength of the polyurethane component. In a preclinical burn model by Cheshire et al,20 BTM achieved superior vascularization and host cell infiltration than CCS. Early clinical studies of BTM have reported its successful outcomes in small case series for a variety of wound locations and indications, including burns, lower extremity trauma, necrotizing fasciitis, and surgical wounds.10,14-16, The potential advantages of BTM include its wider time window allowable for skin grafting15 and ability to salvage template infections without surgery.
This study comparing BTM treatment in 5 patients and CCS treatment in 10 patients demonstrates similar rates of complications and complete closure in head and neck wounds. The complication encountered most often was skin graft failure in the CCS group and skin graft infection in the BTM group. Furthermore, the number of patients needing at least 1 template reapplication were similar between groups. However, whereas 8 patients (80%) in the CCS group required a second surgery for skin grafting, only 3 patients (60%) in the BTM group required this. This discrepancy indicates an increased likelihood of requiring a secondary skin grafting procedure for patients receiving CCS treatment. Not only are the patients exposed to routine risks of a second surgery, but they are also exposed to a potential source for additional morbidities such as postoperative pain, infection, bleeding, and delayed healing.21–23 Although this study contains a relatively low number of patients, reducing the need for secondary surgery can reduce costs associated with use of one dermal template compared with another. Furthermore, surgeon specialty may reflect underlying differences in wound status as all BTM cases were applied by plastic surgeons, whereas CCS was applied by both plastic surgeons and burn surgeons.
Limitations
One primary study limitation is the small sample size of patients with head and neck injuries treated with either BTM or CCS dermal templates. This rendered the study underpowered to detect quantitative differences in characteristics and outcomes between the BTM and CCS groups. Furthermore, because the study examined outcomes retrospectively, it was not possible to minimize the impact of potential confounders through randomization. Therefore, a large-scale, prospective, randomized study is needed. Another limitation of this study is that outcomes such as the rate of complete healing were acquired through review of the electronic medical record. This likely resulted in an underestimation of the rate of complete healing in both groups as many patients who had healed wounds followed up by telephone visit or forwent their in-person visit. Finally, the lack of evaluation of important outcomes including patient satisfaction, scar appearance, mobility, and secondary contracture were not measured. Given the aesthetic and functional demands of the head and neck region, this information would provide insight into the relative benefits or drawbacks to using the BTM dermal template compared with the CCS dermal template.
Conclusions
Head and neck wounds treated with BTM demonstrated comparable closure rates; time to healing; and complication rates for infection, dehiscence, hematoma, and seroma compared with CCS bilayer. Wounds treated with BTM required fewer secondary procedures including skin grafting. These findings suggest that BTM is a safe and efficacious alternative dermal template for head and neck wound reconstruction.
Acknowledgments
Affiliations: 1Cleveland Clinic Lerner College of Medicine, Cleveland, OH; 2Case Western Reserve University School of Medicine, Cleveland, OH; 3Division of Plastic and Reconstructive Surgery, Department of Surgery, Northwestern University Feinberg School of Medicine, Chicago, IL; 4Division of Plastic Surgery, Department of Surgery, Cleveland Clinic Akron General, Akron, OH; 5Division of Plastic Surgery, Department of Surgery, MetroHealth Medical Center, Cleveland, OH
Correspondence: James Gatherwright, MD; gatherj@ccf.org
Presented at: Northeastern Society of Plastic Surgeons 38th Annual Meeting, September 10-12, 2021, Philadelphia, PA.
Ethics: All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5). This study received Institutional Review Board approval. For a retrospective study, formal consent is not required. Patient consent for photographs was obtained.
Disclosures: KC and JC are paid consultants for Polynovo Biomaterials but were not involved in data collection or analysis. None of the other authors have significant conflicts of interest with any companies or organizations whose products or services may be discussed in this article.
References
1. Brusselaers N, Pirayesh A, Hoeksema H, et al. Skin replacement in burn wounds. J Trauma. 2010;68(2):490-501. doi:10.1097/TA.0b013e3181c9c074
2. Chou TD, Chen SL, Lee TW, et al. Reconstruction of burn scar of the upper extremities with artificial skin. Plast Reconstr Surg. 2001;108(2). doi:10.1097/00006534-200108000-00015
3. Ryan CM, Schoenfeld DA, Malloy M, Schulz JT 3rd, Sheridan RL, Tompkins RG. Use of Integra artificial skin is associated with decreased length of stay for severely injured adult burn survivors. J Burn Care Rehabil. 2002;23(5):311-317. doi:10.1097/00004630-200209000-00002
4. Heimbach DM, Warden GD, Luterman A, et al. Multicenter postapproval clinical trial of Integra dermal regeneration template for burn treatment. J Burn Care Rehabil. 2003;24(1):42-48. doi:10.1097/00004630-200301000-00009
5. Schiavon M, Francescon M, Drigo D, et al. The use of integra dermal regeneration template versus flaps for reconstruction of full-thickness scalp defects involving the calvaria: a cost-benefit analysis. Aesthetic Plast Surg. 2016;40(6):901-907. doi:10.1007/s00266-016-0703-0
6. Johnson MB, Wong AK. Integra-based reconstruction of large scalp wounds: a case report and systematic review of the literature. Plast Reconstr Surg - Glob Open. 2016;4(10):e1074. doi:10.1097/GOX.0000000000001074
7. Burd A, Wong PSY. One-stage Integra reconstruction in head and neck defects. J Plast Reconstr Aesthet Surg. 2010;63(3):404-409. doi:10.1016/j.bjps.2008.11.105
8. Food and Drug Administration 510(k) S. Published 2015. Accessed January 28, 2021. https://www.accessdata.fda.gov/cdrh_docs/pdf14/K142879.pdf
9. Wagstaff MJ, Schmitt BJ, Caplash Y, Greenwood JE. Free flap donor site reconstruction: a prospective case series using an optimized polyurethane biodegradable temporizing matrix. Eplasty. 2015;15:e27. Published 2015 Jun 26.
10. Li A, Dearman BL, Crompton KE, Moore TG, Greenwood JE. Evaluation of a novel biodegradable polymer for the generation of a dermal matrix. J Burn Care Res. 2009;30(4):717-728. doi:10.1097/BCR.0b013e3181abffca
11. Greenwood JE. The evolution of acute burn care - retiring the split skin graft. Ann R Coll Surg Engl. 2017;99(6):432-438. doi:10.1308/rcsann.2017.0110
12. Tatai L, Moore TG, Adhikari R, et al. Thermoplastic biodegradable polyurethanes: the effect of chain extender structure on properties and in-vitro degradation. Biomaterials. 2007;28(36):5407-5417. doi:10.1016/j.biomaterials.2007.08.035
13. Damkat-Thomas L, Greenwood JE, Wagstaff MJD. A synthetic biodegradable temporising matrix in degloving lower extremity trauma reconstruction: a case report. Plast Reconstr Surg - Glob Ope.. 2019;7(4):e2110. doi:10.1097/GOX.0000000000002110
14. Greenwood JE, Schmitt BJ, Wagstaff MJD. Experience with a synthetic bilayer Biodegradable Temporising Matrix in significant burn injury. Burn Open. 2018;2(1):17-34. doi:10.1016/j.burnso.2017.08.001
15. Wagstaff MJD, Salna IM, Caplash Y, Greenwood JE. Biodegradable Temporising Matrix (BTM) for the reconstruction of defects following serial debridement for necrotising fasciitis: A case series. Burn Open. 2019;3(1):12-30. doi:10.1016/j.burnso.2018.10.002
16. Wu-Fienberg Y, Wu SS, Gatherwright J, Chepla KJ. An alternative dermal template for reconstruction of complex upper extremity wounds. Plast Reconstr Surg - Glob Open. 2021;9(7):e3674. doi:10.1097/GOX.0000000000003674
17. Hu X, Zeng G, Zhou Y, Sun C. Reconstruction of skin defects on the mid and lower face using expanded flap in the neck. J Craniofac Surg. 2017;28(2):e137-e141. doi:10.1097/SCS.0000000000003394
18. Agbara R, Obiadazie AC, Fomete B, Omeje KU. Orofacial soft tissue reconstruction with locoregional flaps in a health resource-depleted environment: experiences from Nigeria. Arch Plast Surg. 2016;43(3):265-271. doi:10.5999/aps.2016.43.3.265
19. Gabrysz-Forget F, Tabet P, Rahal A, Bissada E, Christopoulos A, Ayad T. Free versus pedicled flaps for reconstruction of head and neck cancer defects: a systematic review. J Otolaryngol Head Neck Surg. 2019;48(1):13. Published 2019 Mar 14. doi:10.1186/s40463-019-0334-y
20. Cheshire PA, Herson MR, Cleland H, Akbarzadeh S. Artificial dermal templates: A comparative study of NovoSorb™ Biodegradable Temporising Matrix (BTM) and Integra(®) Dermal Regeneration Template (DRT). Burns. 2016;42(5):1088-1096. doi:10.1016/j.burns.2016.01.028
21. Kim PD, Fleck T, Heffelfinger R, Blackwell KE. Avoiding secondary skin graft donor site morbidity in the fibula free flap harvest. Arch Otolaryngol Head Neck Surg. 2008;134(12):1324-1327. doi:10.1001/archotol.134.12.1324
22. Klein S, Hage JJ, Woerdeman LA. Donor-site necrosis following fibula free-flap transplantation: a report of three cases. Microsurgery. 2005;25(7):538-542. doi:10.1002/micr.20169
23. Shindo M, Fong BP, Funk GF, Karnell LH. The fibula osteocutaneous flap in head and neck reconstruction: a critical evaluation of donor site morbidity. Arch Otolaryngol Head Neck Surg. 2000;126(12):1467-1472. doi:10.1001/archotol.126.12.1467