

Frequency and Evolution of Thin-Capped Fibroatheromas in Left Main Coronary Artery as Assessed by Serial Virtual Histology Intravascular Ultrasound Analysis
Abstract: Background. The objective of the current study was to assess thin-capped fibroatheroma (TCFA) of the left main coronary artery (LMCA) and its changes after statin therapy. Methods. We assessed the frequency and distribution of virtual histology intravascular ultrasound (VH-IVUS) thin-capped fibroatheroma (VH-TCFA) in the LMCA in 500 patients. Serial VH-IVUS examinations were available in 50 patients at 12-month follow-up. Results. The incidence of LM-TCFA was 8.8% (44/500). IVUS LMCA length was longer in patients with VH-TCFA vs without VH-TCFA. Reference external elastic membrane (EEM) area was similar, but reference lumen area and minimal lumen area were smaller in LMCA with VH-TCFA vs without VH-TCFA (P<.001). LMCA with VH-TCFA had a higher plaque burden (P<.001), a larger necrotic core area (P<.001), and more dense calcium (P<.001) at the maximum necrotic core (NC) site vs LMCA without VH-TCFA. In patients with an LMCA length greater than the median, 62% were located in the distal half of the LMCA. After 12 months of statin therapy, only 44.4% (4/9) of VH-TCFA had evolved to a non-VH-TCFA phenotype and 3 new VH-TCFA had appeared. Conclusion. VH-TCFAs are clustered in the distal half of the LMCA with infrequent positive remodeling. It might persist despite the usual dose of statin therapy. Further study should confirm the changes in large vessels like the LMCA.
J INVASIVE CARDIOL 2014;26(4):175-179
Key words: left main coronary artery disease, vulnerable plaque, virtual histology intravascular ultrasound
_______________________________
Occlusion of the left main coronary artery (LMCA) following plaque rupture can be disastrous because it’s the major source of blood supply to the myocardium.1-10 The importance of intravascular ultrasound (IVUS) examination in assessing LMCA disease has been reported in numerous studies.4,11-13 These studies showed that LMCA atherosclerosis and its progression are often underestimated by coronary angiography.3,14
Thin-capped fibroatheroma (TCFA) is the most common type of vulnerable plaque, the precursor of plaque rupture and thrombosis.15-17 In one study of stable patients, new virtual histology (VH)-TCFAs developed and most existing VH-TCFAs healed during 12-month follow-up;18 however, this study did not include LMCA lesions. Thus, because the characteristics and natural history of LMCA TCFAs have not been well studied, the objective of the current study was to use VH-IVUS to assess LMCA TCFAs and their changes after statin therapy.
Methods
Study population. We used VH-IVUS to assess mild to moderate LMCA disease (angiographic diameter stenosis, 20%-60%) in 500 consecutive patients and identified 44 patients with VH-TCFA. Serial VH-IVUS examinations were available in 50/500 patients (10%) at 12 months of follow-up. Of the 50 patients, 39 were statin naïve and all were subsequently treated with the usual dose of statins during follow-up: pitavastatin 2 mg (Kowa Pharmaceuticals) in 28 patients who were part of LAMIS (Livalo Acute Myocardial Infarction Study) trial,19 atorvastatin 10 mg (Pfizer) in 14 patients, and simvastatin 10 mg (Merck) in 8 patients.
We excluded patients with a large LMCA that exceeded the diameter of the IVUS image (10 mm; n = 32), patients with a short LMCA (<3 mm; n = 48), and patients without adequate grayscale or VH-IVUS data (n = 28). The protocol was approved by the Institutional Review Board, and written informed consent was obtained from all patients.
Hypertension was defined as systolic blood pressure ≥140 mm Hg, diastolic blood pressure ≥90 mm Hg, or use of an antihypertensive drug. Patients with diabetes mellitus had a confirmed diagnosis or were using antidiabetic medications. A lipid disorder was defined as total cholesterol level ≥240 mg/dL, low-density lipoprotein cholesterol ≥100 mg/dL, triglycerides ≥150 mg/dL, or medication use. Current smoking was defined as tobacco use within past 12 months. A family history of coronary artery disease was defined as myocardial infarction of a first-degree relative <60 years of age.
Quantitative coronary angiography analysis. Coronary angiography was performed after 200 µg of intracoronary nitroglycerin. All angiograms were analyzed independently with an automated edge-detection algorithm (AI-1000 Century; GE Medical Systems) using standard protocols. For each LMCA lesion, lesion length, minimal luminal diameter, reference vessel diameter, and percent diameter stenosis were measured using end-diastolic frames.
IVUS imaging and analysis. A commercially available VH-IVUS system (Volcano Therapeutics) and 20 MHz transducers were used for all IVUS examinations. All IVUS studies were performed after intracoronary administration of 200 µg nitroglycerin using an automatic pullback device (R-100; Volcano Therapeutics). The distal end of the LMCA was the first image slice in which the contralateral vessel was no longer seen (ie, the left circumflex [LCX] if the IVUS catheter was positioned in the left anterior descending [LAD] artery). The proximal end of the LMCA was the last image slice in which the entire circumference of the LMCA was seen just before entering the aorta. Studies were recorded onto electronic media for off-line analysis. Two experienced analysts (SWK and WSL) reviewed the VH-IVUS pullbacks to assess lesion phenotype and make precise measurements by defining the two standard IVUS regions of interest: the inner border (lumen, excluding IVUS-detectable thrombus) and outer border (EEM). Qualitative analysis was performed according to criteria of the American College of Cardiology clinical expert consensus document on IVUS to include external elastic membrane (EEM), lumen, and plaque and media (EEM minus lumen) areas.20 Volumes were calculated using Simpson’s rule. VH-IVUS analyses were reported in absolute amounts and as percentages (relative amounts) of plaque area. LMCA lesion phenotype was classified as pathologic intimal thickening (PIT), VH-TCFA, thick-capped fibroatheroma (ThCFA), and fibrotic or fibrocalcific plaque as defined before.21 Positive remodeling was defined as remodeling index (lesion/reference EEM area) greater than 1.05. Subjects were divided into two groups depending on median LMCA length: less than or greater than the median. LMCAs greater than the median were divided into three segments: ostial (3 mm distal to the LMCA ostium), mid-body, and distal bifurcation (3 mm proximal to the polygon of confluence).
than the median were divided into three segments: ostial (3 mm distal to the LMCA ostium), mid-body, and distal bifurcation (3 mm proximal to the polygon of confluence).
Statistical analysis. Statistical analysis was performed with SAS version 9.2 (SAS Institute, Inc). Continuous variables are presented as mean ± 1 standard deviation and compared using student’s t-test. Chi-Square test was used to assess the categorical variable. A P-value <.05 was considered statistically significant.
Results
Patient characteristics and angiographic findings. Baseline clinical characteristics and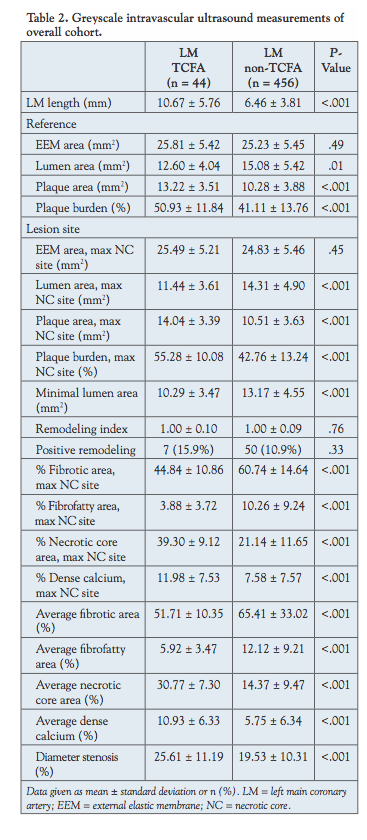 procedural details are shown in Table 1. The angiographic length of the LMCA was longer (P<.01); however, the angiographic minimal lumen diameter and reference vessel diameter were smaller in LMCA with VH-TCFA vs LMCA without VH-TCFA (P<.001 and P=.01, respectively).
procedural details are shown in Table 1. The angiographic length of the LMCA was longer (P<.01); however, the angiographic minimal lumen diameter and reference vessel diameter were smaller in LMCA with VH-TCFA vs LMCA without VH-TCFA (P<.001 and P=.01, respectively).
IVUS and VH-IVUS findings. The incidence of LMCA VH-TCFAs was 8.8% (44/500). IVUS LMCA length was longer in patients with VH-TCFA vs without VH-TCFA. Reference EEM area was similar, but reference lumen area and minimal lumen area were smaller in LMCA with VH-TCFA vs without VH-TCFA (P<.001). LMCA with VH-TCFA had a greater plaque burden (P<.001), a larger necrotic core area (P<.001), and more dense calcium (P<.001) at the maximum NC site compared to LMCA without VH-TCFA (Table 2).
Comparing LMCAs that were longer than the median vs LMCAs that were shorter than the median length, longer LMCAs had a larger EEM CSA (P<.001), a smaller minimum lumen area (P=.01),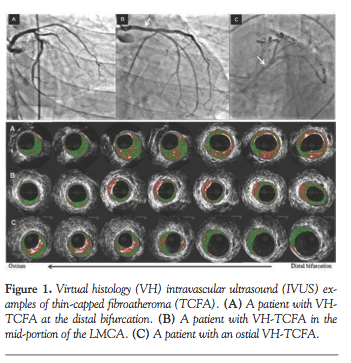 and a larger plaque burden (P=.01); however, plaque composition was similar, as was the frequency of positive remodeling (data not shown). In LMCAs longer than the median in length, 63.6% of VH-TCFAs were located in the mid-body and the rest at the distal bifurcation; however, 62% were located in the distal half of the LMCA (Figure 1).
and a larger plaque burden (P=.01); however, plaque composition was similar, as was the frequency of positive remodeling (data not shown). In LMCAs longer than the median in length, 63.6% of VH-TCFAs were located in the mid-body and the rest at the distal bifurcation; however, 62% were located in the distal half of the LMCA (Figure 1).
Serial IVUS and VH-IVUS LMCA changes. In the 50 patients with serial VH-IVUS examinations at baseline and 12-month follow-up, LDL levels decreased from 121 ± 42 mg/dL to 89 ± 18 mg/dL (P<.001). After 12 months of statin therapy, the lumen area at the maximum NC site decreased (P=.01) while the plaque burden increased (P=.03) (Table 3).
Of the 9 patients with a VH-TCFA at baseline, 4 evolved to a non-VH-TCFA phenotype during follow-up, while 3 new VH-TCFAs appeared from fibrotic plaque even though LDL levels decreased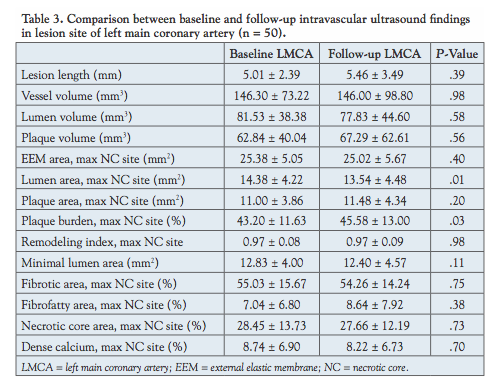 in all patients (9/9), with 7/9 having an LDL <100 mg/dL. The follow-up level of LDL was <90 mg/dL in 2/3 patients with a newly developed VH-TCFA (Table 4).
in all patients (9/9), with 7/9 having an LDL <100 mg/dL. The follow-up level of LDL was <90 mg/dL in 2/3 patients with a newly developed VH-TCFA (Table 4).
Discussion
The main findings of the present study are as follows: (1) VH-TCFAs are present in 9% of LMCAs with mild to moderate disease; (2) when present, VH-TCFAs are located more frequently in the distal half of the LMCA; and (3) VH-TCFAs in the LMCA can persist despite statin therapy and reduction of LDL cholesterol. In patients undergoing primary percutaneous coronary intervention, the culprit lesion is located in the LMCA in 0.8%-7.0%. These patients have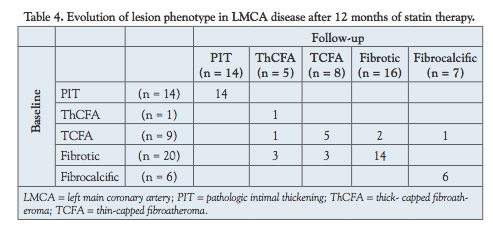 high rates of mortality because of frequent cardiogenic shock and malignant tachyarrhythmias.6-9 When present, ruptured plaques almost exclusively involve the distal part of the LMCA and/or its bifurcation and occur opposite the distal flow divider.22,23 In the current study, 72.7% of VH-TCFAs occurred opposite the flow divider and in the mid-portion of the LMCA. In addition, only 3 of the 44 VH-TCFAs in this study also showed plaque rupture.
high rates of mortality because of frequent cardiogenic shock and malignant tachyarrhythmias.6-9 When present, ruptured plaques almost exclusively involve the distal part of the LMCA and/or its bifurcation and occur opposite the distal flow divider.22,23 In the current study, 72.7% of VH-TCFAs occurred opposite the flow divider and in the mid-portion of the LMCA. In addition, only 3 of the 44 VH-TCFAs in this study also showed plaque rupture.
Three previous studies have used VH-IVUS to assess LMCA disease. Valmigli et al compared the LMCA and its carina to six consecutive non-overlapping 6 mm segments in the LAD or LCX; the NC was minimal in the LMCA, peaked in the first 6-mm long coronary segment in the LAD or LCX, and then decreased more distally.24 In a global VH registry, dense calcium and NC were less in the LMCA compared to the LAD, and the frequency of VH-TCFA was lower in the LMCA than in the LAD (0% vs 16.9%; P<.001).25 Using data from PROSPECT, the LMCA had a smaller percentage of NC and dense calcium than the proximal segments of the other three epicardial arteries and only 1.8% of 496 LMCA segments contained a lesion that was classified as a VH-TCFA compared to 18.9% of the proximal 30-mm long segments of the LAD, LCX, and RCA.26 The frequency of VH-TCFA is higher compared to previous studies; however, the current study was performed in a difference racial population compared to either the global VH registry or PROSPECT.27 In one previous study of non-LMCA lesions, most VH-TCFAs healed during 12-month follow-up. However, proximal VH-TCFAs in larger vessels with more plaque appeared to heal less often,18 similar to the current study of LMCA lesions that are located in a large proximal artery with a low wall shear stress, which might be one of the factors to cause a different nature of the LMCA.28 There might be cultural differences of LMCA lesions in the Asian population.29 In one serial grayscale IVUS study, LDL values <75 mg/dL were not associated with plaque progression.30 This is in distinct contrast to the current study. However, the frequency of LMCA-TCFA was infrequent and sample size was relatively small for the conclusion.
were less in the LMCA compared to the LAD, and the frequency of VH-TCFA was lower in the LMCA than in the LAD (0% vs 16.9%; P<.001).25 Using data from PROSPECT, the LMCA had a smaller percentage of NC and dense calcium than the proximal segments of the other three epicardial arteries and only 1.8% of 496 LMCA segments contained a lesion that was classified as a VH-TCFA compared to 18.9% of the proximal 30-mm long segments of the LAD, LCX, and RCA.26 The frequency of VH-TCFA is higher compared to previous studies; however, the current study was performed in a difference racial population compared to either the global VH registry or PROSPECT.27 In one previous study of non-LMCA lesions, most VH-TCFAs healed during 12-month follow-up. However, proximal VH-TCFAs in larger vessels with more plaque appeared to heal less often,18 similar to the current study of LMCA lesions that are located in a large proximal artery with a low wall shear stress, which might be one of the factors to cause a different nature of the LMCA.28 There might be cultural differences of LMCA lesions in the Asian population.29 In one serial grayscale IVUS study, LDL values <75 mg/dL were not associated with plaque progression.30 This is in distinct contrast to the current study. However, the frequency of LMCA-TCFA was infrequent and sample size was relatively small for the conclusion.
Study limitations. First, this study was a small observational registry. Second, most of the patients had mild to moderate LMCA disease. The inclusion of severe LMCA stenosis was limited because the IVUS catheter could not cross the severe stenotic lesion of the LMCA, and IVUS follow-up was impossible after stent implantation. Third, large diameter or very short LMCAs were excluded because of the difficulty in taking IVUS measurements. Fourth, we did not analyze or compare the LMCA to non-LMCA locations. Fifth, an LDL level <70 mg/dL was achieved in only 9/50 patients (18%) in the current study. We still do not know the adequate doses of statin in this study population. Finally, although the pathophysiologic mechanism of TCFA is similar, there might be racial differences contributing to the primary finding.
Conclusion
VH-TCFAs are clustered in the distal half of the LMCA with infrequent positive remodeling. It might persist through the usual dose of statin therapy and reduction of LDL cholesterol. Further studies should identify the additional factors causing persistent TCFA in the LMCA.
References
- Gerber TC, Erbel R, Gorge G, Ge J, Rupprecht HJ, Meyer J. Extent of atherosclerosis and remodeling of the left main coronary artery determined by intravascular ultrasound. Am J Cardiol. 1994;73(9):666-671.
- Hermiller JB, Buller CE, Tenaglia AN, et al. Unrecognized left main coronary artery disease in patients undergoing interventional procedures. Am J Cardiol. 1993;71(2):173-176.
- Bergelson BA, Tommaso CL. Left main coronary artery disease: assessment, diagnosis, and therapy. Am Heart J. 1995;129(2):350-359.
- Abizaid AS, Mintz GS, Abizaid A, et al. One-year follow-up after intravascular ultrasound assessment of moderate left main coronary artery disease in patients with ambiguous angiograms. J Am Coll Cardiol. 1999;34(3):707-715.
- Ricciardi MJ, Meyers S, Choi K, Pang JL, Goodreau L, Davidson CJ. Angiographically silent left main disease detected by intravascular ultrasound: a marker for future adverse cardiac events. Am J Heart. 2003;146(3):507-512.
- Yip HK, Wu CJ, Chen MC, et al. Effect of primary angioplasty on total or subtotal left main occlusion: Analysis of incidence, clinical features, outcomes, and prognostic determinants. Chest. 2001;120(4):1212-1217.
- De Luca G, Suryapranata H, Thomas K, et al. Outcome in patients treated with primary angioplasty for acute myocardial infarction due to left main coronary artery occlusion. Am J Cardiol. 2003;91(2):235-238.
- Lee SW, Hong MK, Lee CW, et al. Early and late clinical outcomes after primary stenting of the unprotected left main coronary artery stenosis in the setting of acute myocardial infarction. Int J Cardiol. 2004;97(1):73-76.
- Spiecker M, Erbel R, Rupprecht HJ, Meyer J. Emergency angioplasty of totally occluded left main coronary artery in acute myocardial infarction and unstable angina pectoris-institutional experience and literature review. Eur Heart J. 1994;15(5):602-607.
- Seo SM, Kim TH, Kim CJ, et al; Korean Acute Myocardial Infarction Registry Investigators. Prognostic impact of significant non-infarct-related left main coronary artery disease in patients with acute myocardial infarction who receive a culprit-lesion percutaneous coronary intervention. Coron Artery Dis. 2012;23(5):307-314.
- Kang SJ, Lee JY, Ahn JM, et al. Intravascular ultrasound-derived predictors for fractional flow reserve in intermediate left main disease. JACC Cardiovasc Interv. 2011;4(11):1168-1174.
- Fassa AA, Wagatsuma K, Higano ST, et al. Intravascular ultrasound-guided treatment for angiographically indeterminate left main coronary artery disease: a long-term follow-up study. J Am Coll Cardiol. 2005;45(2):204-211.
- Jasti V, Ivan E, Yalamanchili V, Wongpraparut N, Leesar MA. Correlations between fractional flow reserve and intravascular ultrasound in patients with an ambiguous left main coronary artery stenosis. Circulation. 2004;110(18):2831-2836.
- Topol EJ, Nissen SE. Our preoccupation with coronary luminology. The dissociation between clinical and angiographic findings in ischemic heart disease. Circulation. 1995;92(8):2333-2342.
- Virmani R, Burke AP, Farb A, Kolodgie FD. Pathology of the vulnerable plaque. J Am Coll Cardiol. 2006;47(8 Suppl):C13-C18.
- Farb A, Burke AP, Tang AL, et al. Coronary plaque erosion without rupture into a lipid core. A frequent cause of coronary thrombosis in sudden coronary death. Circulation. 1996;93(7):1354-1363.
- Burke AP, Kolodgie FD, Farb A, et al. Healed plaque ruptures and sudden coronary death. Evidence that subclinical rupture has a role in plaque progression. Circulation. 2001;103(7):934-940.
- Kubo T, Maehara A, Mintz GS, et al. The dynamic nature of coronary artery lesion morphology assessed by serial virtual histology intravascular ultrasound tissue characterization. J Am Coll Cardiol. 2010;55(15):1590-1597.
- Suh SY, Rha SW, Ahn TH, et al. Long-term safety and efficacy of Pitavastatin in patients with acute myocardial infarction (from the Livalo Acute Myocardial Infarction Study [LAMIS]), Am J Cardiol. 2011;108(11):1530-1535.
- Mintz GS, Nissen SE, Anderson WD, et al. American College of Cardiology clinical expert consensus document on standards for acquisition, measurement and reporting of intravascular ultrasound studies (IVUS). J Am Coll Cardiol. 2001;37(5):1478-1492.
- Nair A, Margolis MP, Kuban BD, Vince DG. Automated coronary plaque characterisation with intravascular ultrasound backscatter: ex vivo validation. EuroIntervention. 2007;3(1):113-120.
- Tyczynski P, Pregowski J, Mintz GS, et al. Intravascular ultrasound assessment of ruptured atherosclerotic plaques in left main coronary arteries. Am J Cardiol. 2005;96(6):794-798.
- Pappalardo A, Mamas MA, Imola F, et al. Percutaneous coronary intervention of unprotected left main coronary artery disease as culprit lesion in patients with acute myocardial infarction. JACC Cardiovasc Interv. 2011:4(6):618-626.
- Valgimigli M, Rodriguez-Granillo GA, Garcia-Garcia HM, et al. Plaque composition in the left main stem mimics the distal but not the proximal tract of the left coronary artery: influence of clinical presentation, length of the left main trunk, lipid profile, and systemic levels of C-reactive protein. J Am Coll Cardiol. 2007;49(1):23-31.
- Mercado N, Moe TG, Pieper M, et al. Tissue characterization of atherosclerotic plaque in the left main: an in vivo intravascular ultrasound radiofrequency data analysis. EuroIntervention. 2011;7(3):347-352.
- Wykrzykowska JJ, Mintz GS, Garcia-Garcia HM, et al. Longitudinal distribution of plaque burden and necrotic core-rich plaques in nonculprit lesions of patients presenting with acute coronary syndromes. JACC Cardiovasc Imaging. 2012;5:(3 Suppl)S10-S18.
- Stone GW, Maehara A, Lansky AJ, et al; PROSPECT Investigators. A prospective natural-history study of coronary atherosclerosis. N Engl J Med. 2011;364(3):226-235.
- Soulis JV, Farmakis TM, Giannoglou GD, Louridas GE. Wall shear stress in normal left coronary artery tree. J Biomech. 2006;39(4):742-749.
- Rusinova RP, Mintz GS, Choi SY, et al. Intravascular ultrasound comparison of left main coronary artery disease between white and Asian patients. Am J Cardiol. 2013;111(7):979-984.
- von Birgelen C, Hartmann M, Mintz GS, Baumgart D, Schmermund A, Erbel R. Relation between progression and regression of atherosclerotic left main coronary artery disease and serum cholesterol levels as assessed with serial long-term (> or = 12 months) follow-up intravascular ultrasound. Circulation. 2003;108(22):2757-2762.
From the 1Heart Research Institute, Chung-Ang University Hospital, Seoul, Korea, 2Cardiovascular Research Foundation, New York, New York, and 3Washington Hospital Center, Washington DC.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted September 3, 2013, provisional acceptance given September 20, 2013, final version accepted December 4, 2013.
Address for correspondence; Sang-Wook Kim, MD, PhD, Professor of Medicine, Head of Heart Center, Director of Cardiovascular Research Core Lab, Heart Research Institute, Chung-Ang University Medical Center, 224-1 Heukseok Dong, Dongjak Gu Seoul, Korea, 156-755. Email: swivus@gmail.com













