

Improved Algorithm for Ostium Size Assessment in Watchman Left Atrial Appendage Occlusion Using Three-Dimensional Echocardiography
Abstract: Aims. Correct sizing of the ostium is a crucial step in left atrial appendage (LAA) occlusion procedures. However, unfavorable anatomy of the ostium often complicates the assessment of the true ostium diameter. We hypothesized that area-derived diameter (ADD) and perimeter-derived diameter (PDD) from three-dimensional transesophageal echocardiogram (3D-TEE) can facilitate this step of the procedure as compared with two-dimensional (2D) measurements. Methods and Results. For 55 patients within the ALSTER-LAA registry, retrospective analysis of PDD and ADD was correlated with 2D measurements used during the procedure to ascertain correct size of the Watchman device (Boston Scientific). The observed data were put into relation to the calculated area of the device with 10%-30% compression and the clinical outcome after 30 days. 3D area and perimeter measurements of the LAA ostium matched the calculated range of the different device sizes. Recapture during implantation, gaps <5 mm, and device size changes were more often observed when ADDs would also have suggested the use of a larger device. Conclusion. 3D ADDs and PDDs are feasible to use in device size decisions. Employing these measurements may allow operators to further reduce intraprocedural recapture maneuvers, peridevice leakage, and device size changes.
J INVASIVE CARDIOL 2017;29(7):232-238.
Key words: LAA occlusion, TEE, stroke prevention
Ischemic stroke due to atrial fibrillation is a major contributor to morbidity and mortality in Western societies and its importance is expected to grow with aging populations.1-3 Oral anticoagulation (OAC) with either warfarin or direct oral anticoagulants (DOAC), as recommended by current American Heart Association (AHA) and European Society of Cardiology (ESC) guidelines, comes with an inherent bleeding risk that makes these drugs non-ideal for stroke prevention in all patients; platelet inhibition alone though is inefficient in stroke prevention.4-9 Interventional closure of the left atrial appendage (LAA) employing the Watchman device (Boston Scientific) was shown to be non-inferior to OAC in randomized trials and has since been approved in the United States and Europe.10
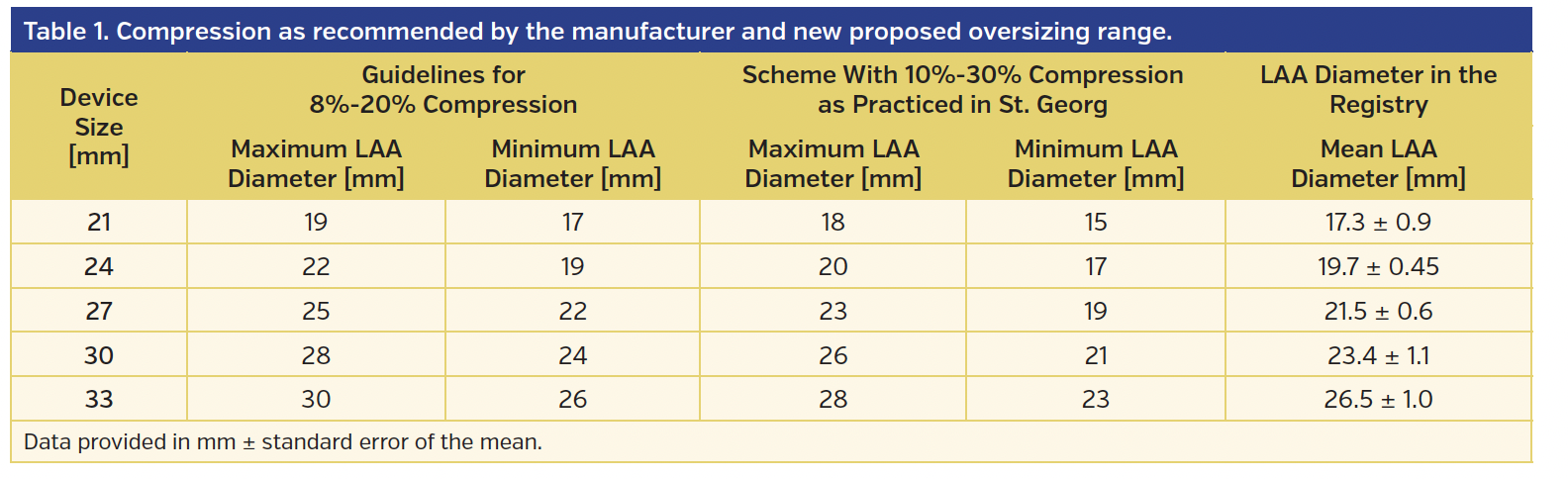
The Watchman device consists of a nitinol frame, with 50% of the device covered by a polyethylene terephthalate (PET) membrane. It is deployed in the LAA ostium following access to the left atrium via transseptal puncture. The PET membrane is later covered with endothelium, which leads to complete LAA occlusion without leaving an artificial orifice open to the bloodstream.11,12 The device is available in 5 different sizes (21-33 mm) to accommodate different LAA ostium sizes. The manufacturer recommends choosing the device size to achieve a compression of 8%-20%, whereas registry data suggest that a greater compression (15%-30%) is as safe and might lead to less peridevice leakage as well as a reduced need for repositioning the device after first deployment.13
LAA morphology, including size and shape of the ostium, differs greatly between patients and is in many cases not round but oval shaped.14,15 The ostium diameter is usually measured by angiography (right anterior oblique caudal or cranial) and two-dimensional transesophageal echocardiography (2D-TEE) in different angles (0°, 45°, 90°, 135°). Unfortunately, in an oval-shaped ostium, these measurements provide differing values and lead to difficulties in choosing the adequate device size, especially in the early phase of establishing the procedure (during the learning curve).16
In the field of transcatheter aortic valve replacement (TAVR), a similar problem was encountered with assessment of the aortic annulus size, where in addition to an often not strictly round annulus, different sizing modalities like TEE, computed tomography (CT), or angiography often led to differing results, making it difficult to choose the correct valve size.16 In this context, the acquisition of area-derived diameter (ADD) and perimeter-derived diameter (PDD) have been proposed to improve the correct selection of valve size.17-19 It could be demonstrated that PDDs might be less prone to interobserver variability than direct diameter measurements.20 In addition, some authors suggested that for the LAA occlusion, three-dimensional (3D) imaging techniques might provide additional value as well.21,22
We hypothesized that 3D-derived diameters based on ADD and PDD would lead to accurate results regarding device sizing in LAA procedures as well and therefore developed a sizing algorithm that enabled the user to choose a device size according to ADD and PDD values as assessed by 3D-TEE. In order to further validate this approach, we retrospectively identified a group of consecutive patients for whom 3D datasets were available and determined whether the good clinical results achieved by very experienced physicians based on 2D images would have been possible by simply applying our proposed algorithm.
Methods
Study design. All patients treated with LAA occlusion in our center are included in an open-label, single-center registry. Baseline characteristics, procedural details, and follow-up data are collected prospectively; the analyses of the 3D datasets were performed retrospectively.
Patient population. A total of 55 consecutive patients who underwent LAA occlusion using the Watchman device between November 2012 and August 2014 were selected for analysis. LAA occlusion was performed according to institutional standards based on ESC guidelines focusing on OAC-ineligible (absolute or relative) patients; increased risk for bleeding (HAS-BLED score ≥3) and an annual stroke risk >2% (CHA2DS2-VASc score ≥2) were the most common indications. Only patients with 3D datasets available for retrospective analysis were included. Hence, our study collective represents a real-world, all-comers population.
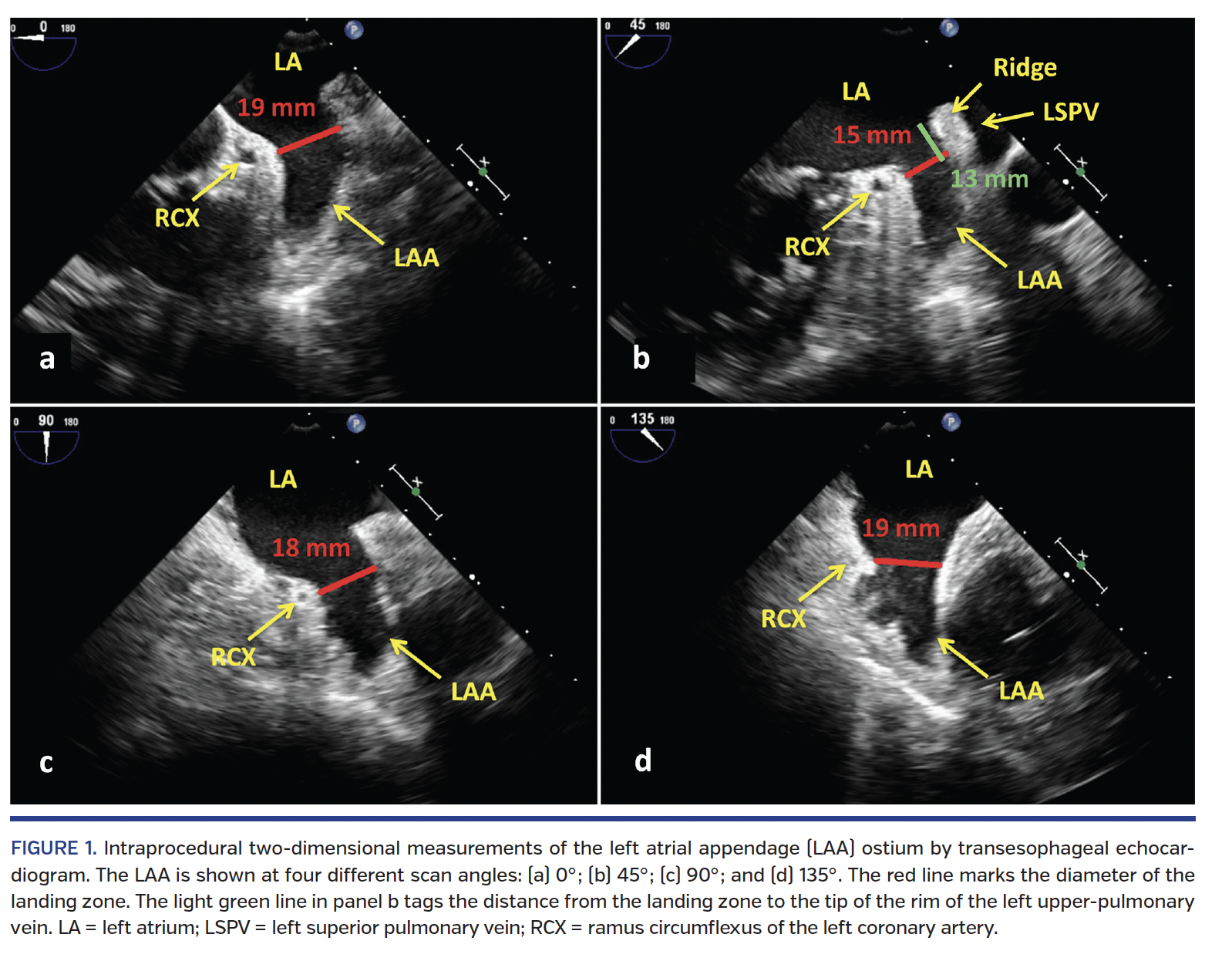
Peri-interventional echocardiography. During the LAA occlusion procedure, 2D-TEE and 3D-TEE were performed by an experienced echocardiographer with a commercially available echocardiographic system (iE33; Philips Medical Systems). In order to determine the maximal diameter of the occluder landing zone, the LAA was scanned at four different 2D views (search angles 0°, 45°, 90°, and 135°) (Figure 1). In all four views, measurements of the ostial diameter were performed from the inferior aspect of the ostium at the level of the circumflex artery to the opposing edge approximately 1-2 cm distally to the tip of the rim to the left upper-pulmonary vein (Figure 1).15 Care was taken to undergo measurements when the diameter appeared largest (ventricular systole for patients in sinus rhythm). The maximal diameter of the four measurements was used for device sizing.
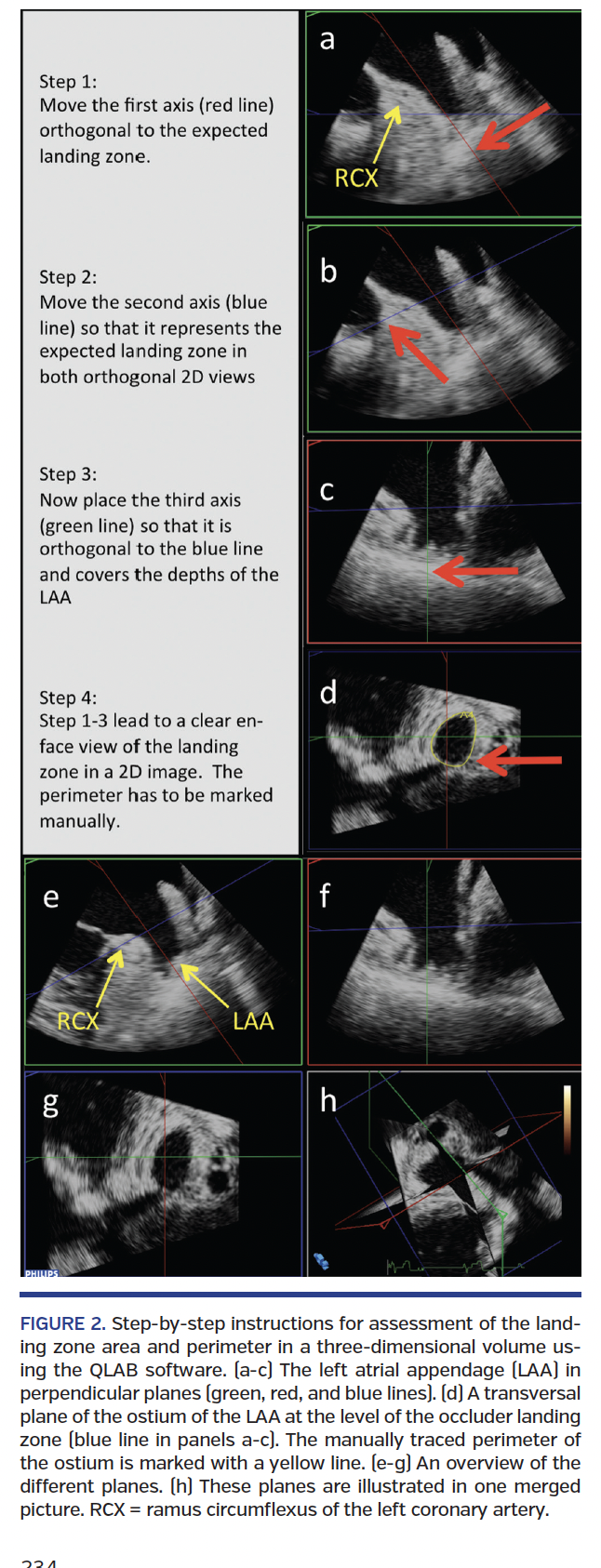
Single-beat 3D-Zoom volumes of the complete LAA acquired intraprocedurally were analyzed after the procedure for measurement of the area and the perimeter of the LAA ostium at the landing zone of the occluder device. The 3D volumes had a medium volume rate of 8 volumes/sec, and image gain was kept at factory settings. Analysis was performed using a dedicated software (QLAB, v. 10.2; Philips Medical Systems). In order to optimally display the ostial area of the LAA, two perpendicular planes were first oriented along the main axis of the LAA (Figure 2, green and red lines). Then, the third plane (Figure 2, blue line) was positioned exactly at the level of the landing zone by applying the same anatomical criteria as for the 2D measurements. This allowed measurements of both the ADD and PDD.
Procedural details. CT imaging was not performed routinely prior to LAA occlusion. All procedures were performed under conscious sedation with simultaneous fluoroscopic and TEE guidance. Presence of thrombus within the LAA was ruled out prior to transseptal puncture in all patients; most of the patients had not undergone TEE prior to the periprocedural echo analysis in order to minimize the risk of esophageal bleeding and to avoid patient discomfort associated with repeated TEE exams. After visualizing the LAA in fluoroscopy (right anterior oblique caudal view) and TEE (0°, 45°, 90°, 135°, and 3D) (Figure 1), the device size was chosen according to our local algorithm aiming for 15%-30% compression (“2 sizes up”) (Table 1).13 After deployment, a tug-test was performed and sealing as well as compression of the device were assessed by TEE. In case these implantation criteria were not met, the device was either recaptured and repositioned, or another device size was chosen. During the procedure, unfractionated heparin was administered in order to maintain an activated clotting time >250 sec. The patients were discharged on dual-antiplatelet therapy until TEE follow-up approximately 3 months after the implantation documented permanent sealing of the LAA and no thrombus on the device. Patients were then switched to aspirin monotherapy until 1 year after the procedure.
Results
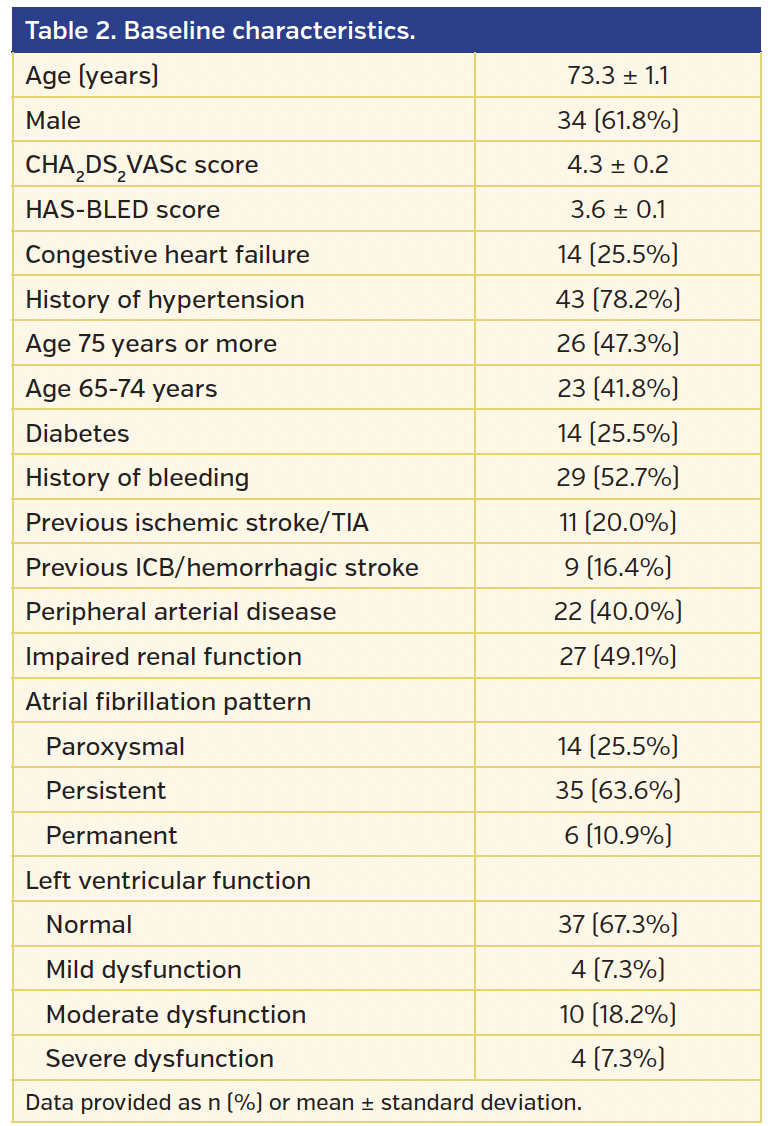
Patient characteristics and procedural details. A total of 55 patients were included in the analysis. The mean age was 73.3 ±1.1 years and 34 (61.8%) were male. The CHA2DS2-VASc and HAS-BLED scores were 4.3 ± 0.2 and 3.6 ± 0.1, respectively (Table 2). No major procedure-associated adverse events occurred, and the LAA was occluded successfully in all cases. None of the patients had a relevant peridevice leakage at the end of the procedure. All patients were discharged on the day after the procedure on dual-antiplatelet therapy. Follow-up including TEE was available for 35 patients (63.6%) at 3 months. There was no device embolization, but 2 thrombus formations were detected on the device during follow-up; both resolved completely under low-molecular-weight heparin for 4 weeks.
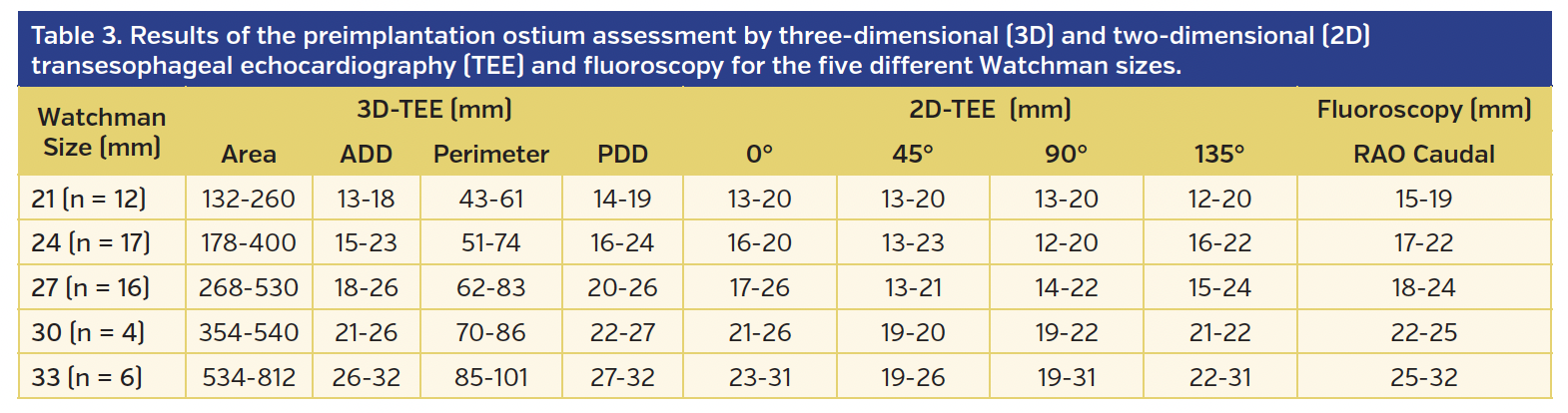
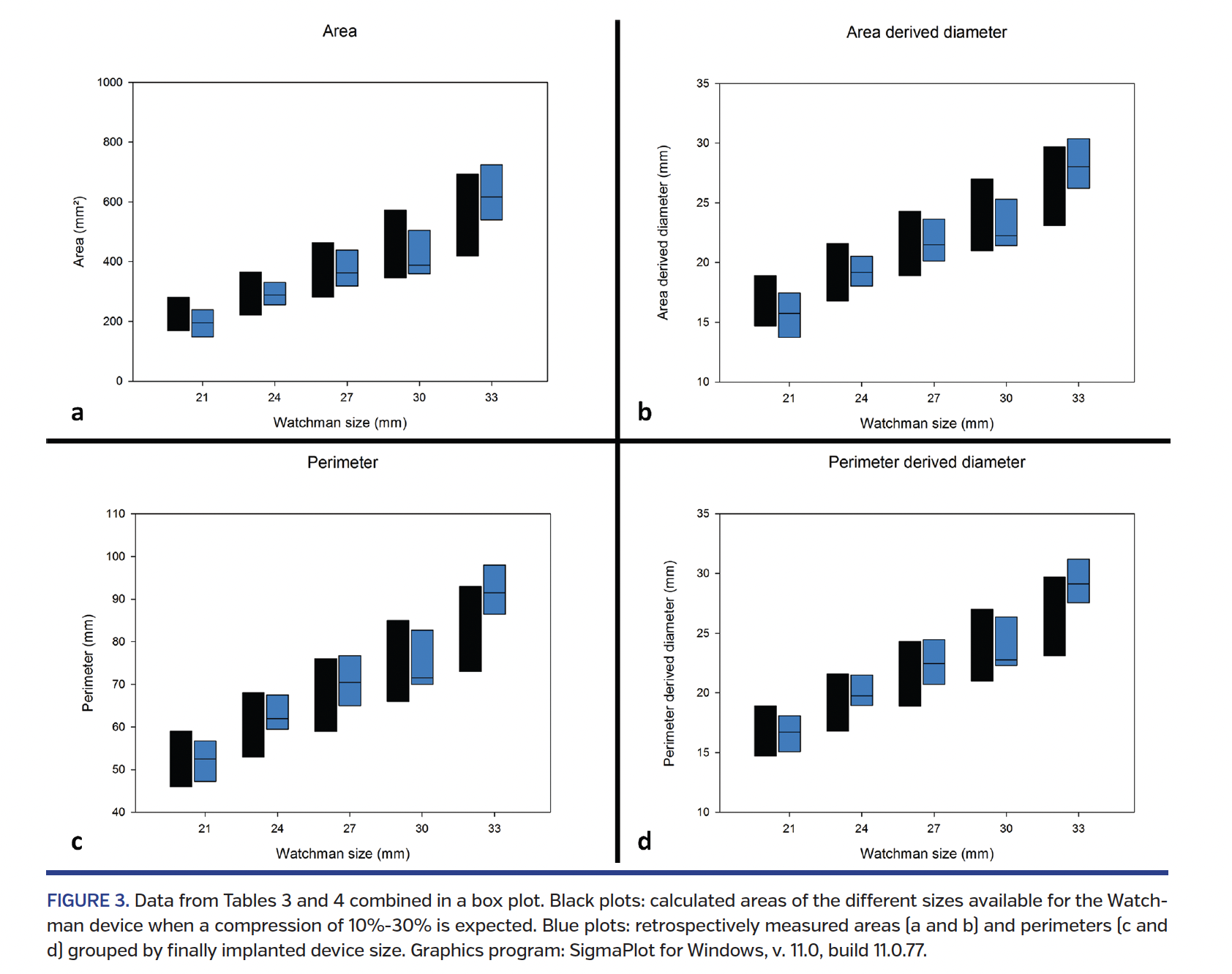
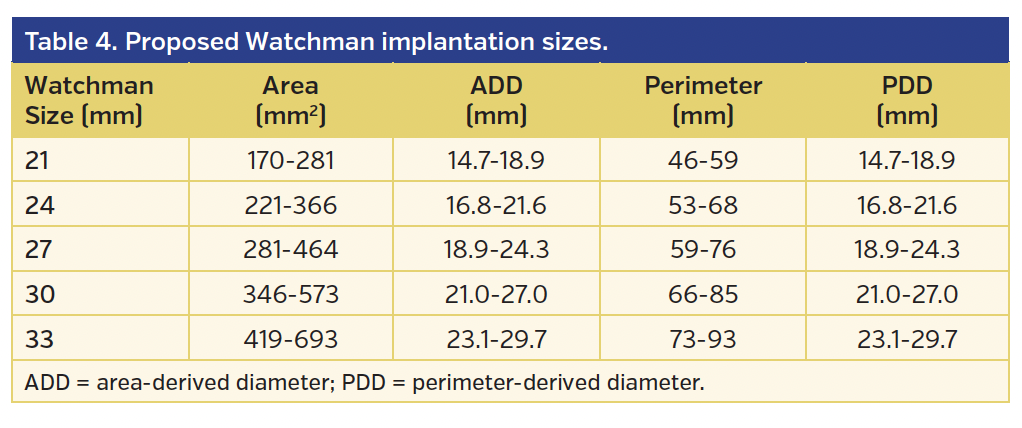
Ostium measurements. Table 3 and Figure 3 show the results as measured in our 3D datasets. In addition, Table 4 illustrates calculated values for ADD (x = 2(√area)/π) and PDD (x = perimeter/π) to yield a compression of 10%-30%. Figure 3 compares the calculated and measured values for each device size, with 43 of the measured values (78.2%) lying within the  calculated range. The figure demonstrates that the diameters measured in 3D-TEE fit the actually implanted device sizes, which were determined by 2D-TEE.
calculated range. The figure demonstrates that the diameters measured in 3D-TEE fit the actually implanted device sizes, which were determined by 2D-TEE.
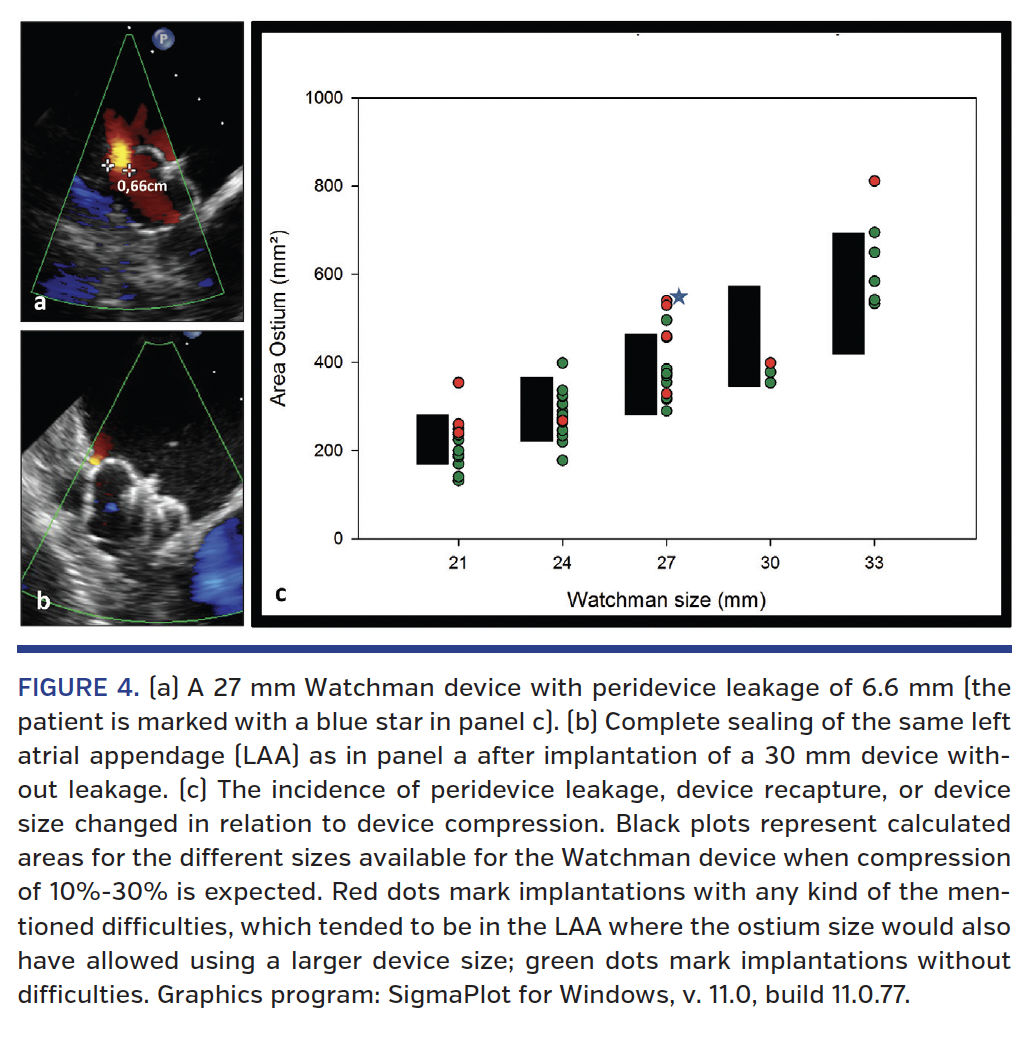
We also analyzed the incidence of peridevice leakage, device recapture, or device size change (Figure 4) as related to the calculated device size. These difficulties tended to occur in LAAs where ostium sizes in 3D-TEE would also have allowed using one device size larger. An example for this finding is demonstrated in Figure 4, which illustrates a patient in whom the device size had to be changed during the procedure. This could have been avoided in this patient and in several other cases if the ostium area had been used for sizing.
Development of the proposed implantation scheme. As previously mentioned, registry data have shown device compression up to 30% to be safe. Therefore, we propose to aim for a compression of 10%-30% during implantation. In order to provide a standardized algorithm for device sizing including the ADD and PDD, we calculated the ranges of ADD and PDD for each device size, leading to the aforementioned compression range.
Using this calculation, we created an implantation scheme that combines all available sizing variables (Table 4) and allows for the implanting physician to easily choose a proper device size according to measured diameters in 2D and the area measurements in 3D. In case the calculated ostium diameter allows for the implantation of two device sizes, we recommend choosing the larger device.
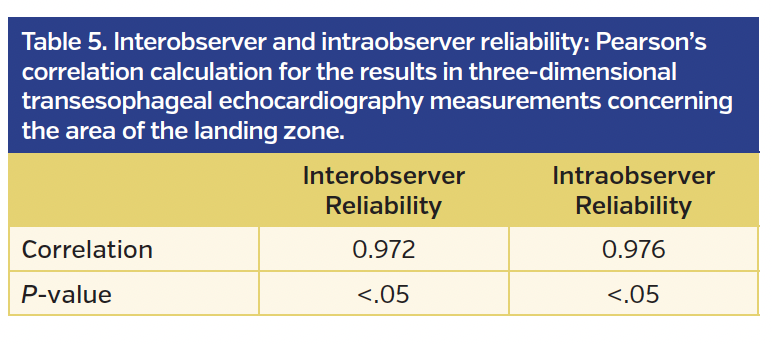
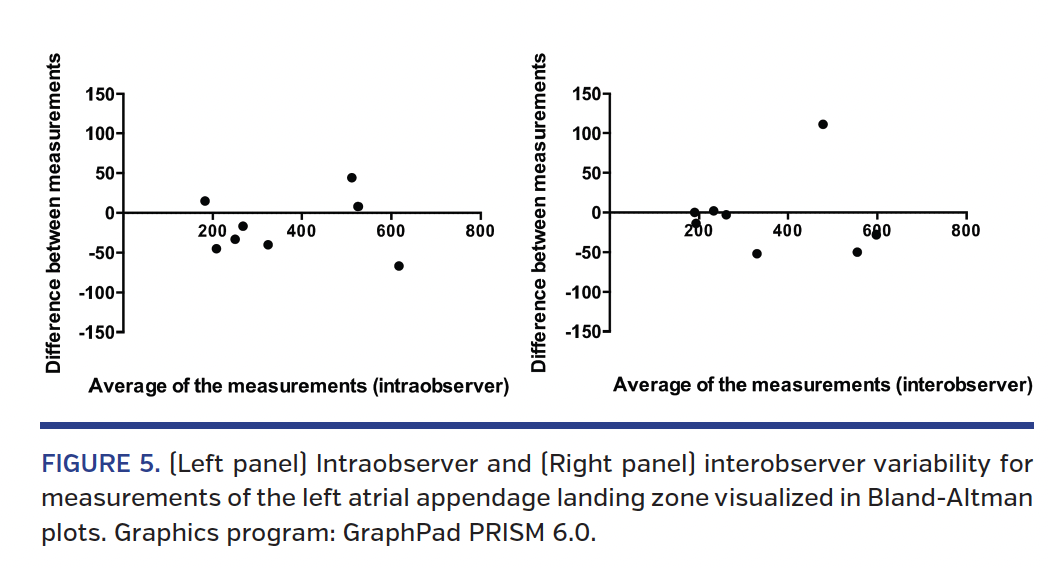
Interobserver/intraobserver variabilities. Interobserver and intraobserver variabilities for assessing the area and perimeter of the LAA landing zone were performed for 8 randomly selected patients and calculated by Pearson’s correlation. The results are displayed in Table 5 and Figure 5, and demonstrate excellent correlation.
Discussion
For the first time, we report data on the use of the ADD and PDD to facilitate the process of ostium sizing for implantation of the Watchman device. After developing a sizing algorithm based in these measurements, we validated this in a retrospective cohort of patients and correlated imaging data with clinical outcomes, including periprocedural observations regarding peridevice leakage, device recapture, and device size changes.
During implantation of the Watchman device, ascertainment of the device size is a crucial step that often leads to uncertainty, especially in centers not yet experienced with the procedure. In addition, some LAA anatomies are difficult to interpret even for experienced operators. A device that is too small compared with the ostium size might have a negative tug test, resulting in device size changes, peridevice leakage, and several recaptures necessary before obtaining an acceptable result.23 These increase the risk for pericardial tamponade, periprocedural stroke, and other issues. On the other hand, a larger device than necessary may encounter problems regarding the required LAA depth; it may also increase the risk for pericardial effusion. Unfortunately, the decision on device size is extremely complex, because the LAA anatomy is quite variable and the ostium is often oval rather than round. The 2D measurements recommended by the manufacturer have limited ability to provide the implanting physician with a proper understanding of the complexity of the LAA anatomy. However, there is no standardized algorithm for how to incorporate 3D measurements into the ostium sizing. As with TAVR, the use of PDD and ADD could provide a way to introduce 3D information into LAA occlusion in a standardized fashion that is easy to adopt even for inexperienced physicians. Our analysis shows a collective of patients who underwent LAA occlusion with very good procedural results in terms of pericardial tamponade (none) or peridevice leakages. Our retrospective analyses of this cohort shows that ADD and PDD correlate well with the device sizes chosen to yield these good results. In addition, some peri-interventional difficulties, such as device repositioning and changes to a different device size, could have been avoided using ADD or PDD for device size selection.
The use of 3D imaging techniques might also provide a tool that is easy to adopt, especially for less experienced implanting physicians and echocardiographers, as this method is most likely more reproducible than other sizing options, as demonstrated by the small interobserver and intraobserver variability on our data.
In our series, no CT imaging was performed before the procedures. On one hand, CT is capable of providing high-quality images of the LAA landing zone in most patients. On the other hand, performing CT scan before every implantation leads to higher radiation and contrast exposure, higher costs, and possibly even longer hospital stay. Therefore, in our opinion, CT should not be regarded mandatory before LAA occlusion. In addition, prior studies have demonstrated a significant variability of LAA sizes depending on the volume status of the patient.24 Therefore, assessment of the landing zone diameter and implantation of the device should be performed at the same time as volume status.
We therefore suggest a standardized algorithm for determining the Watchman device size that includes 3D measurements to assess ADD and PDD (Table 4). This issue grows even more important because of the increasing importance of LAA occlusion in guidelines and the recent approval of the Watchman device by the United States Food and Drug Administration, which will lead to a significant increase in procedures worldwide meaning that many less-experienced physicians will start an LAA program.
Conclusion
Using ADD or PDD for LAA ostium sizing and decision on the size of the particular Watchman device is feasible; our data suggest this approach to be easy, reliable, and reproducible. In addition, 3D landing zone measurement leads to a higher reproducibility compared with 2D measurements in several planes, as currently believed to be necessary to decide upon device size.
References
1. Go AS, Hylek EM, Phillips KA, et al. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA. 2001;285:2370-2375.
2. Roger VL, Go AS, Lloyd-Jones DM, et al. Heart disease and stroke statistics – 2012 update: a report from the American Heart Association. Circulation. 2012;125:e2-e220.
3. Stewart S, Hart CL, Hole DJ, McMurray JJ. Population prevalence, incidence, and predictors of atrial fibrillation in the Renfrew/Paisley study. Heart. 2001;86:516-521.
4. January CT, Wann LS, Alpert JS, et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol. 2014;64:e1-e76.
5. Camm AJ, Kirchhof P, Lip GY, et al. Guidelines for the management of atrial fibrillation: the Task Force for the Management of Atrial Fibrillation of the European Society of Cardiology (ESC). Eur Heart J. 2010;31:2369-2429.
6. Brass LM, Krumholz HM, Scinto JM, Radford M. Warfarin use among patients with atrial fibrillation. Stroke. 1997;28:2382-2389.
7. Bungard TJ, Ackman ML, Ho G, Tsuyuki RT. Adequacy of anticoagulation in patients with atrial fibrillation coming to a hospital. Pharmacotherapy. 2000;20:1060-1065.
8. Bungard TJ, Ghali WA, Teo KK, McAlister FA, Tsuyuki RT. Why do patients with atrial fibrillation not receive warfarin? Arch Intern Med. 2000;160:41-46.
9. Gladstone DJ, Bui E, Fang J, et al. Potentially preventable strokes in high-risk patients with atrial fibrillation who are not adequately anticoagulated. Stroke. 2009;40:235-240.
10. Holmes DR, Reddy VY, Turi ZG, et al. Percutaneous closure of the left atrial appendage versus warfarin therapy for prevention of stroke in patients with atrial fibrillation: a randomised non-inferiority trial. Lancet. 2009;374:534-542.
11. Schwartz RS, Holmes DR, Van Tassel RA, et al. Left atrial appendage obliteration: mechanisms of healing and intracardiac integration. JACC Cardiovasc Interv. 2010;3:870-877.
12. Bergmann MW, Landmesser U. Left atrial appendage closure for stroke prevention in non-valvular atrial fibrillation: rationale, devices in clinical development and insights into implantation techniques. EuroIntervention. 2014;10:497-504.
13. Meincke F, Schmidt-Salzmann M, Kreidel F, Kuck KH, Bergmann MW. New technical and anticoagulation aspects for left atrial appendage closure using the WATCHMAN(R) device in patients not taking warfarin. EuroIntervention. 2013;9:463-468.
14. Beigel R, Wunderlich NC, Ho SY, Arsanjani R, Siegel RJ. The left atrial appendage: anatomy, function, and non-invasive evaluation. JACC Cardiovasc Imaging. 2014;7:1251-1265.
15. Wunderlich NC, Beigel R, Swaans MJ, Ho SY, Siegel RJ. Percutaneous interventions for left atrial appendage exclusion: options, assessment, and imaging using 2D and 3D echocardiography. JACC Cardiovasc Imaging. 2015;8:472-488.
16. Zamorano J, Gonçalves A, Lancellotti P, et al. The use of imaging in new transcatheter interventions: an EACVI review paper. Eur Heart J Cardiovasc Imaging. 2016;17:835-835af.
17. Binder RK, Webb JG, Willson AB, et al. The impact of integration of a multidetector computed tomography annulus area sizing algorithm on outcomes of transcatheter aortic valve replacement: a prospective, multicenter, controlled trial. J Am Coll Cardiol. 2013;62:431-438.
18. Hansson NC, Thuesen L, Hjortdal VE, et al. Three-dimensional multidetector computed tomography versus conventional 2-dimensional transesophageal echocardiography for annular sizing in transcatheter aortic valve replacement: Influence on postprocedural paravalvular aortic regurgitation. Catheter Cardiovasc Interv. 2013;82:977-986.
19. Jilaihawi H, Kashif M, Fontana G, et al. Cross-sectional computed tomographic assessment improves accuracy of aortic annular sizing for transcatheter aortic valve replacement and reduces the incidence of paravalvular aortic regurgitation. J Am Coll Cardiol. 2012;59:1275-1286.
20. Schmidkonz C, Marwan M, Klinghammer L, et al. Interobserver variability of CT angiography for evaluation of aortic annulus dimensions prior to transcatheter aortic valve implantation (TAVI). Eur J Radiol. 2014;83:1672-1678.
21. Goebel B, Wieg S, Hamadanchi A, et al. Interventional left atrial appendage occlusion: added value of 3D transesophageal echocardiography for device sizing. Int J Cardiovasc Imaging. 2016;32:1363-1370.
22. Yosefy C, Laish-Farkash A, Azhibekov Y, Khalameizer V, Brodkin B, Katz A. A new method for direct three-dimensional measurement of left atrial appendage dimensions during transesophageal echocardiography. Echocardiography. 2016;33:69-76.
23. Viles-Gonzalez JF, Kar S, Douglas P, et al. The clinical impact of incomplete left atrial appendage closure with the Watchman device in patients with atrial fibrillation: a PROTECT AF (Percutaneous Closure of the Left Atrial Appendage Versus Warfarin Therapy for Prevention of Stroke in Patients With Atrial Fibrillation) substudy. J Am Coll Cardiol. 2012;59:923-929.
24. Spencer RJ, DeJong P, Fahmy P, et al. Changes in left atrial appendage dimensions following volume loading during percutaneous left atrial appendage closure. JACC Cardiovasc Interv. 2015;8:1935-1941.
*Joint first authors.
From the 1Department for Cardiology, Asklepios Klinik St. Georg, Hamburg, Germany; 2Medizinische Klinik II, Universitaetsklinik Bonn, Germany; and 3Cardiologicum, Hamburg, Germany.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Meincke, Dr Ghanem, and Dr Bergmann report personal fees from Boston Scientific. The remaining authors report no conflicts of interest regarding the content herein.
Manuscript submitted January 29, 2017 and accepted February 7, 2017.
Address for correspondence: Prof Martin W. Bergmann, Cardiologicum Hamburg, Schloßgarten 3, 22041 Hamburg, Germany. Email: docbergmann@me.com













