

Safety and Feasibility of a Novel, Second-Generation Robotic-Assisted System for Percutaneous Coronary Intervention: First-in-Human Report
Abstract: Objectives. The goal of this study is to evaluate the safety and efficacy of the second-generation robotic-assisted system CorPath GRX (Corindus) for percutaneous coronary intervention (PCI). Background. The first-generation CorPath 200 robotic-assisted system for PCI is effective, but is limited by the lack of an active robotic guide-catheter control. The CorPath GRX device enables robotic guide-catheter manipulation, in addition to guidewire and balloon/stent delivery. However, there have been no clinical data reported with this device. Methods. Consecutive patients with demonstrated obstructive coronary artery disease (>70% stenosis) and clinical indications for PCI were treated with the CorPath GRX system and enrolled in the study. The two co-primary endpoints were clinical procedural success (final TIMI 3 flow, and <30% residual stenosis without in-hospital major adverse cardiac event) and device technical success (robotic clinical procedural success without the need for unplanned manual assistance/conversion). Results. The study enrolled 40 subjects (65.7 ± 11.9 years; 72.5% males; 54 lesions) with a high proportion of American College of Cardiology/American Heart Association type B2/C lesions (77.8%). Clinical procedural success and device technical success rates were 97.5% (n = 39 of 40) and 90.0% (n = 36 of 40), respectively. Conclusion. The second-generation CorPath GRX system for robotic-assisted PCI is safe and effective, and achieves high rates of clinical and technical success in a cohort of patients with complex coronary disease.
J INVASIVE CARDIOL 2018;30(4):152-156. Epub 2018 January 15.
Key words: robotics, percutaneous coronary intervention, coronary innovation, CorPath GRX
Percutaneous coronary intervention (PCI) is associated with well-known occupational and procedural risks to cardiologists and medical staff performing fluoroscopically guided cardiac procedures.1-3 Robotic-assisted PCI was developed to mitigate some of these occupational hazards, and studies have shown that use of the first-generation CorPath 200 (Corindus) robotic-assisted system for PCI is associated with lower radiation exposure for the interventional operator as compared to conventional PCI.4 Additionally, prior studies have established the first-generation robotic-assisted PCI system to be effective for the treatment of patients with simple to complex coronary and peripheral vascular disease.4-7 However, the first-generation system was limited by the lack of robotic guide-catheter control.
A second-generation robotic-assisted system, the CorPath GRX (Corindus), has been developed and received United States Food and Drug Administration approval. As compared to the first-generation device, it has improved functional control with faster guidewire rotation, simplified device exchanges, and the addition of a third joystick for guide-catheter manipulation. However, this device has not been assessed clinically. We undertook this study to evaluate the clinical and technical success of this novel, second-generation robotic-assisted system for PCI, and are reporting the first-in-human experience.
Methods
This is a single-arm, open-label, single-center investigation of a novel, robotic-assisted angioplasty system among patients undergoing PCI. The study protocol was approved by the University of California, San Diego Human Research Protections Program. In an analysis of our previous data,6 we observed a learning curve of 11-20 procedures with the CorPath 200 robotic system when utilized for complex coronary procedures. Hence, a sample size of 40 procedures to evaluate the initial experience with the CorPath GRX system was chosen.
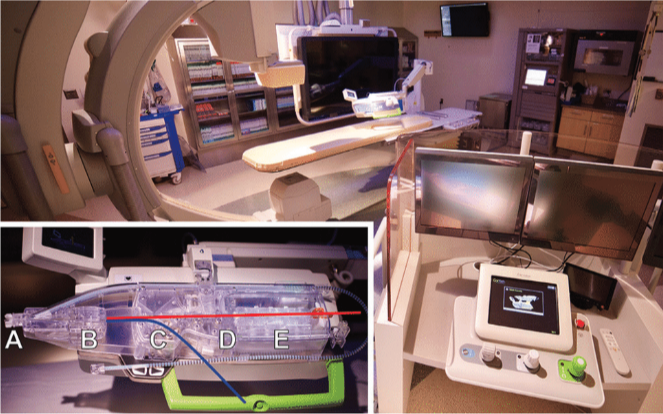
Robotic system. The CorPath GRX system includes two components: an interventional cockpit and a bedside unit (Figure 1). The interventional cockpit is a radiation-shielded mobile workstation that contains a console with joysticks and touchscreen controls used by the interventional cardiologist to control movement of the balloon/stent delivery system, guidewire, or guide catheter. The bedside unit consists of a single-use cassette, articulating arm, and robotic drive. During the PCI procedure, the single-use cassette is loaded with interventional equipment and is mounted on a robotic drive, which translates commands from the cockpit to independently manipulate each device. The system accepts all 0.014˝ guidewires and rapid-exchange balloon/stent catheters, in addition to standard coronary guide catheters of various sizes.
All operators had training on the system and previously demonstrated expertise with the CorPath 200 system. The PCI procedures were performed with commercially available coronary guidewires, balloons, and stents. Anticoagulation and antiplatelet therapy were administered per standard protocol.
Study population. Consecutive subjects undergoing robotically assisted PCI with the CorPath GRX system were enrolled in the study. All subjects had evidence of obstructive coronary artery disease (>70% stenosis by visual estimate) and clinical indication for PCI. Major exclusion criteria for robotic PCI included ST-elevation myocardial infarction (MI) or lesions not treatable due to known limitations of the robotic platform (eg, chronic total occlusion requiring hybrid approach, bifurcation lesions with planned two-stent approach, and planned rotational or orbital atherectomy).
Study endpoints. The two primary endpoints were clinical procedural success and technical success, similar to prior studies.4,6,8 Clinical procedural success was defined as <30% residual stenosis and final TIMI 3 flow after PCI, in the absence of an in-hospital major adverse cardiac event (MACE) during the index hospitalization following PCI. MACE included death, MI, urgent revascularization, and emergent cardiac surgery. The Society for Cardiovascular Angiography and Intervention definition of periprocedural MI was used, which requires clinical evidence of a myocardial injury pattern.9 Technical success was defined as clinical procedural success with robotic-assisted PCI without the need for unplanned manual assistance or conversion to manual PCI for procedural completion.6
Statistical analysis. Continuous variables were summarized using mean ± standard deviation. Categorical variables were summarized using percentages. All calculations were performed by Microsoft Excel (version 15.30).
Results
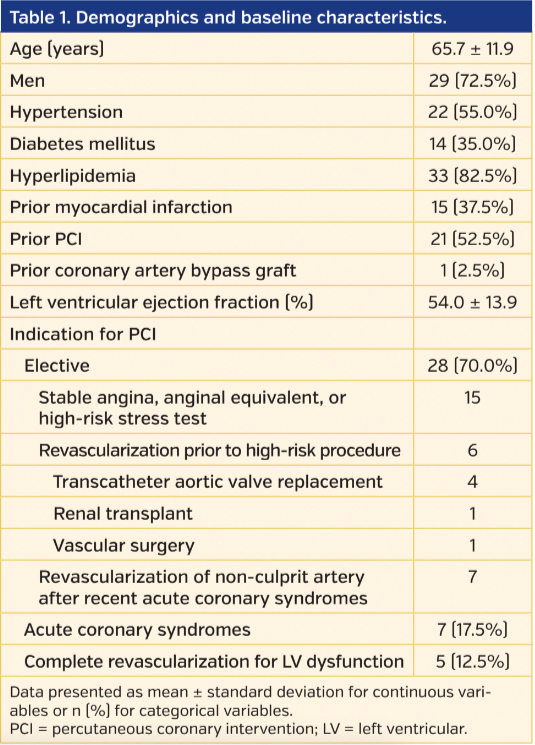
A total of 40 subjects were included (age, 65.7 ± 11.9 years; 72.5% males) with a high proportion of patients having cardiovascular disease risk factors and history of prior MI and PCI. Radial access was used for the majority of procedures (65%). Indications for PCI included elective procedures for stable ischemic heart disease (n = 28), urgent PCI for acute coronary syndromes (n = 7), or planned complete revascularization for left ventricular dysfunction (n = 5) (Table 1).
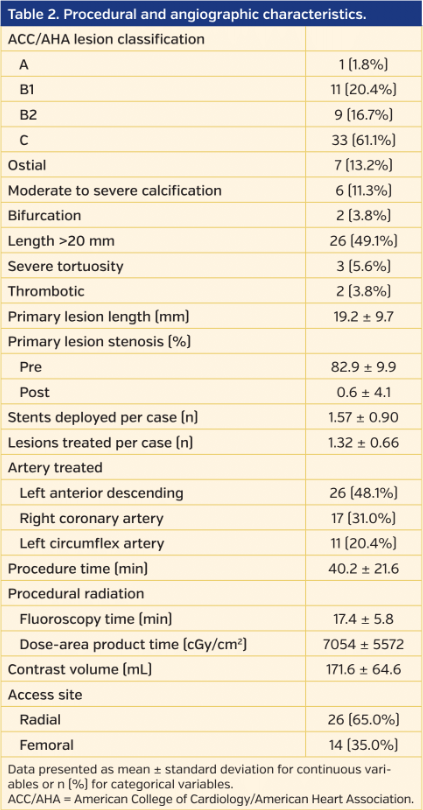
Overall, the 54 lesions treated in the study were complex, with 77.8% of the treated lesions being American College of Cardiology/American Heart Association type B2/C. Furthermore, 13.2% of lesions treated were ostial, 11.3% were moderately to severely calcified, 3.8% were bifurcation lesions, and 49.1% were long lesions (≥20 mm). The average lesion length was 19.2 ± 9.7 mm, with 1.57 ± 0.90 stents deployed per procedure (Table 2). Two severely calcified lesions were successfully treated with atherectomy (1 using robotic laser atherectomy [non-dilatable coronary stent in a calcified artery] and 1 with unplanned manual orbital atherectomy followed by robotic procedural completion).
In the study cohort, high rates of clinical procedural success and technical success of 97.5% and 90.0%. respectively, were achieved (Figure 2). Clinical failure in a single patient was due to an inability to cross a chronic total occlusion of the right coronary artery via both robotic assistance and the conventional manual approach. The intervention was successfully completed 2 weeks later with the assistance of a Turnpike Spiral catheter (Vascular Solutions) using an antegrade wire-escalation technique and an over-the-wire approach.
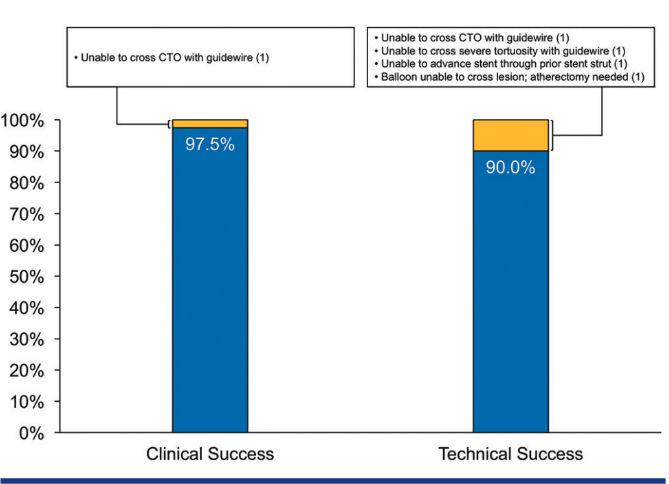
Technical failure occurred in 3 additional procedures. The first involved a lesion that required overlapping stents to be delivered through the side struts of a previously placed stent. Robotically, the first stent was passed through and deployed; however, the second stent could not be advanced enough to overlap the proximal edge of the initial stent. Ultimately, the procedure was converted to the manual approach and a buddy-wire technique was used to successfully deliver the second stent to the desired location. The second procedure requiring unplanned manual conversion was related to the guidewire tip control. The culprit lesion was a long (25 mm), highly stenotic (95%), type C lesion in the proximal right coronary artery that could not be crossed with the guidewire using robotic assistance despite multiple attempts. The reason for device failure was felt to be due to suboptimal robotic grip of the guidewire. The third procedure requiring unplanned manual assistance involved an eccentric, moderately calcified coronary lesion that was successfully wired robotically, but could not be crossed with a balloon. Clinical success was achieved after unplanned manual conversion and orbital atherectomy followed by completion of stent deployment robotically.
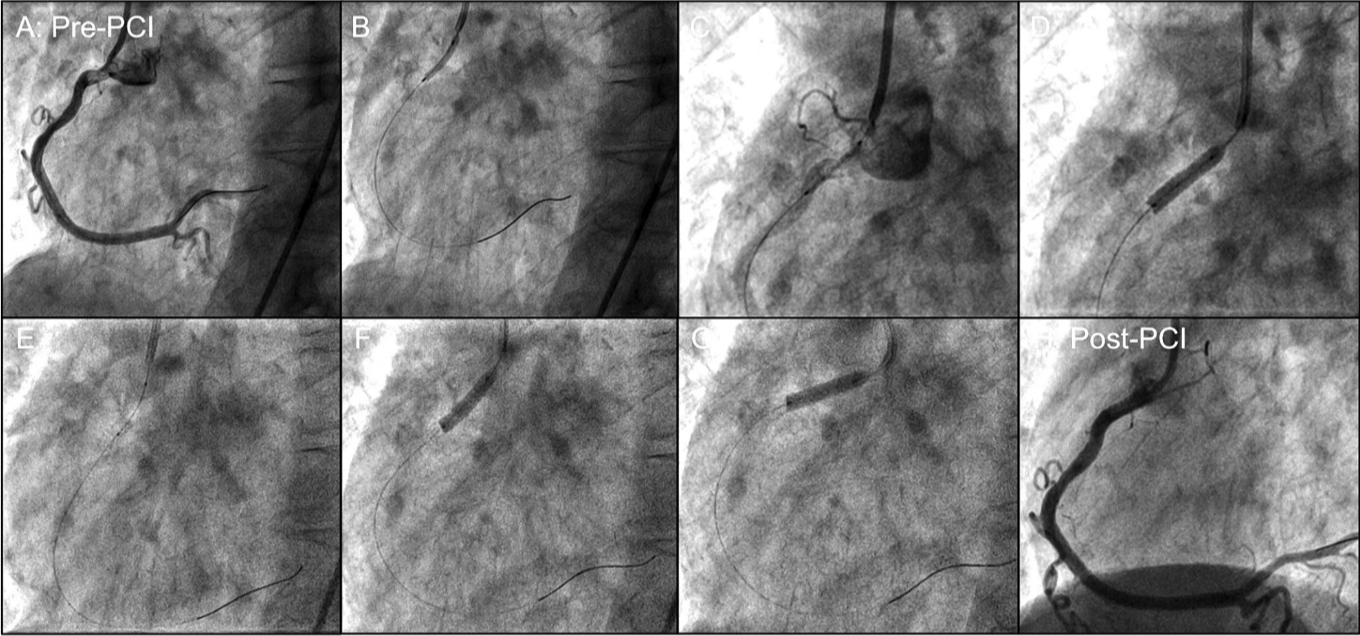
The third joystick for guide-catheter manipulation was used during multiple procedures, as it allowed for improved engagement of the target coronary, especially if it became disengaged during the intervention. It also enabled ostial coronary stenting and flaring of the stent robotically as necessary (Figure 3).
Discussion
We report the first-in-human experience of a novel second-generation robotically assisted PCI system, the CorPath GRX. Using this system in a cohort of patients with complex coronary anatomy achieved a clinical procedural success rate of 97.5% and device technical success rate of 90%.
Although the first-generation robotic system for PCI is effective for patient care, almost 1 in 5 patients with complex coronary anatomy required manual conversion or partial manual assistance for procedure completion.6 Almost half of the procedures requiring partial manual assistance were due to inadequate robotic guide-catheter control. The CorPath GRX system has active rather than passive guide-catheter control, and the current study shows that this iterative improvement resulted in eliminating guide-catheter related issues for robotic PCI even with the majority of procedures involving type B2/C lesions and being completed with radial access. Additional observations from the current study include the ability of the CorPath GRX system to be utilized for ostial lesions and its compatibility with laser atherectomy. Clinical procedural success, device technical success, procedural time, fluoroscopy time, and contrast volume were comparable to a previous study investigating robotic technology in a similar patient cohort.6
The CorPath GRX system added a third joystick to allow for robotic manipulation of the guide catheter in addition to the joysticks for guidewire and balloon/stent control. The intention of enabling guide-catheter manipulation was to decrease the rate of unplanned manual assistance or manual conversion, previously seen in 11.1% of procedures in the CORA-PCI study.6 Inadvertent guide-catheter disengagement can be corrected robotically and active guide-catheter support enhances support for device advancement. In the currently reported experience, the sample size is limited but 10% of the procedures still required unplanned manual assistance or conversion. This should be interpreted in the context of the limited overall sample size of 40 subjects, with all 4 of the conversion patients having complex anatomical disease (chronic total occlusion, balloon uncrossable lesion, advancing a stent through a strut of a previously deployed stent, and severe tortuosity). Importantly, not a single conversion was due to guide-catheter disengagement, and in multiple procedures, it enabled successful re-engagement of the coronary artery without requiring partial, unplanned manual assistance. In 1 of the 4 procedures, inadequate guidewire tip control was felt to be the reason for unplanned manual conversion.
This is the first study with robotically assisted PCI in which the majority of patients were treated utilizing the radial approach. As radial access is sometimes associated with ergonomic challenges and radiation exposure for the operator,10 the feasibility of radial robotic PCI with the CorPath GRX system is reassuring as active guide-catheter control is required more often with radial guide catheters. The successful use of this robotic system for ostial lesions, and in a single laser atherectomy procedure, demonstrates the potential future capabilities of robotic PCI.
Study limitations. Limitations of this study include its open-label, single-center design with a limited number of patients. However, as the purpose of this study was to evaluate initial safety and feasibility of this second-generation robotic PCI system, future trials and registry studies will continue to evaluate outcomes in larger populations and multiple centers.
Conclusion
The novel, second-generation CorPath GRX system for robotic-assisted PCI is safe and effective, and achieves high rates of clinical and technical success in a cohort of patients with complex coronary disease.
References
1. Goldstein JA, Balter S, Cowley M, Hodgson J, Klein LW. Occupational hazards of interventional cardiologists: prevalence of orthopedic health problems in contemporary practice. Catheter Cardiovasc Interv. 2004;63:407-411.
2. Reeves RR, Ang L, Bahadorani J, et al. Invasive cardiologists are exposed to greater left sided cranial radiation: the BRAIN study (Brain Radiation Exposure and Attenuation During Invasive Cardiology Procedures). JACC Cardiovasc Interv. 2015;8:1197-1206.
3. Andreassi MG, Piccaluga E, Guagliumi G, Greco MD, Gaita F, Picano E. Occupational health risks in cardiac catheterization laboratory workers. Circ Cardiovasc Interv. 2016;9:e003273.
4. Weisz G, Metzger DC, Caputo RP, et al. Safety and feasibility of robotic percutaneous coronary intervention: PRECISE (Percutaneous Robotically-Enhanced Coronary Intervention) study. J Am Coll Cardiol. 2013;61:1596-1600.
5. Mahmud E, Schmid F, Kalmar P, et al. Feasibility and safety of robotic peripheral vascular interventions: results of the RAPID trial. JACC Cardiovasc Interv. 2016;9:2058-2064.
6. Mahmud E, Naghi J, Ang L, et al. Demonstration of the safety and feasibility of robotically assisted percutaneous coronary intervention in complex coronary lesions. JACC Cardiovasc Interv. 2017;10:1320-1327.
7. Mahmud E, Dominguez A, Bahadorani J. First-in-human robotic percutaneous coronary intervention for unprotected left main stenosis. Catheter Cardiovasc Interv. 2016;88:565-570.
8. Granada JF, Delgado JA, Uribe MP, et al. First-in-human evaluation of a novel robotic-assisted coronary angioplasty system. JACC Cardiovasc Interv. 2011;4:460-465.
9. Moussa ID, Klein LW, Shah B, et al. Consideration of a new definition of clinically relevant myocardial infarction after coronary revascularization. J Am Coll Cardiol. 2013;62:1563-1570.
10. Sciahbasi A, Frigoli E, Sarandrea A, et al. Radiation exposure and vascular access in acute coronary syndromes: the RADMatrix trial. J Am Coll Cardiol. 2017;69:2530-2537. Epub 2017 Mar 18.
From the UC San Diego Sulpizio Cardiovascular Center, La Jolla, California.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Mahmud reports grant support and clinical trial support from Corindus, unrelated to the present study. The remaining authors report no conflicts of interest regarding the content herein.
Manuscript submitted August 23, 2017, provisional acceptance given August 27, 2017, final version accepted October 29, 2017.
Address for correspondence: Ehtisham Mahmud, MD, UC San Diego Sulpizio Cardiovascular Center, 9434 Medical Center Drive, La Jolla, CA 92037. Email: emahmud@ucsd.edu











