Transcatheter Aortic Valve Replacement Without the Use of Contrast Medium: An Alternative Safe Implantation Technique
Abstract: Background. New transcatheter equipment and accumulated experience have stimulated further refinements in implantation techniques. We aimed to compare the outcomes of transfemoral transcatheter aortic valve replacement (TF-TAVR) with and without the use of contrast medium (CM) in patients with glomerular filtration rate (GFR) <30 mL/min/1.73 m2. Methods. This single-center, retrospective study included all patients who underwent TF-TAVR procedure with Edwards Sapien balloon-expandable bioprostheses between September 2017 and September 2018 at the Zentralklinik Bad Berka Germany, and compared outcomes of TF-TAVR with and without the use of CM. Results. A total of 98 consecutive patients were included in this study; 25 patients underwent TF-TAVR without the use of CM and 73 patients underwent TF-TAVR with the use of CM. Acute kidney injury was significantly higher in patients who received CM (15 patients [20.5%] in the control group vs 1 patient [4%] in the study group; P=.04). Other procedure-related complications were equally distributed between both groups. Conclusion. TF-TAVR without the use of CM can be considered a safe and reproducible alternative technique. Furthermore, it reduced the incidence of postoperative acute kidney injury in patients with GFR <30 mL/min/1.73 m2.
Key words: acute renal injury, contrast solution, kidney disease, nephropathy, TAVI
Recently, transcatheter aortic valve implantation (TAVI) has advanced in the treatment of severe symptomatic aortic valve stenosis in not only high-risk, but also intermediate surgical risk patients.1 Fortunately, the incidence of TAVI-related complications has decreased significantly over recent years, mainly due to progressive improvements in interventional skills, additional experience with the heart team, and advancements in catheter-based equipment. However, acute renal failure (ARF) remains one of the most relevant complications and, despite being rare, is associated with increased postprocedural morbidity and mortality.2,3 The risk of ARF is less common in TAVI patients than in those who undergo surgical aortic valve replacement (SAVR).4 However, ARF is most likely a multifactorial event that is not only related to the use of contrast solution but also to the presence of pre-existing renal disease, congestive heart failure, age, anemia, diabetes, and profound hypotension.5 Notably, contrast-medium induced renal failure is the third most common cause of in-hospital acquired renal failure. The prevalence of contrast-medium induced renal failure peaks at 48 hours post operation and then gradually declines until normalizing during the second postprocedural week.6 Herein, we describe our new protocol for performing TAVI procedures without contrast solution. This strategy has significant potential for decreasing the incidence of contrast-induced ARF following TAVI.
Methods
Study population and data collection. The decisions regarding the method of aortic valve replacement (SAVR vs TAVI), the choice of TAVI prosthesis (balloon expandable vs self expandable), and the access route (transfemoral vs transapical) were made by the institutional heart team, which comprised cardiologists, cardiac surgeons, and anesthesiologists. The specific decision to use a contrast-free procedure was made following a multidisciplinary discussion within the institutional heart team. A total of 25 patients with pre-existing severe nephropathy were included in the study group. During the same study period (September 2017 to September 2018), a total of 187 patients underwent a TAVI procedure with Sapien balloon-expandable bioprostheses (Edwards Lifesciences) at our hospital. From those patients, we identified 73 matched patients with glomerular filtration rates <30 mL/min/1.73 m2. All data were collected retrospectively from our institutional records. Preoperative parameters were obtained from the following: heart catheterization, to perform coronary and iliofemoral angiography; femoral duplex, to exclude femoral atherosclerosis and pseudoaneurysm; three-dimensional (3D) transesophageal echocardiography (TEE), to describe the size and morphology of the valve together with coronary ostia distances; and native computed tomography (CT), to roughly illustrate the valve annular size, coronary ostia distances, and iliofemoral tree gross anatomy.
Statistical analysis. Continuous variables are expressed as means and standard deviations. Categorical data are expressed as percentages. All analyses were done using SPSS statistical software (2013, IBM Corporation; IBM SPSS Statistics for Windows, version 22.0).
Technical aspects of the intervention. The primary goal of the preoperative and intraoperative protocol was to avoid intraoperative complications, such as annular rupture or valve migration, and to implant the transcatheter valve in the most appropriate position without any compromises. Our aim was to implement a precise, complete, investigatory protocol for these patients. The major research question during the preoperative work-up was “how can we gain the same information that contrast-enhanced multislice CT scans preoperatively provide by other investigations, without using contrast solution?” For this purpose, we performed preoperative heart catheterization to perform coronary and iliofemoral angiography (Figure 1) and femoral duplex sonography to exclude femoral atherosclerosis and pseudoaneurysm (Figure 2). Coronary angiography was mandatory as a preoperative investigation. We simultaneously performed iliofemoral angiography with only 10 mL contrast medium, which is a smaller volume than would be used during CT.
Additionally, we used preoperative 3D-TEE to obtain aortic valve (AV) annular size measurements and to obtain a detailed description of the valve morphology as well as the coronary ostia distances. A native CT scan was performed to measure the AV annular size, coronary ostia distances, left ventricular outflow tract morphology, and iliofemoral vessel anatomy (Figure 3).
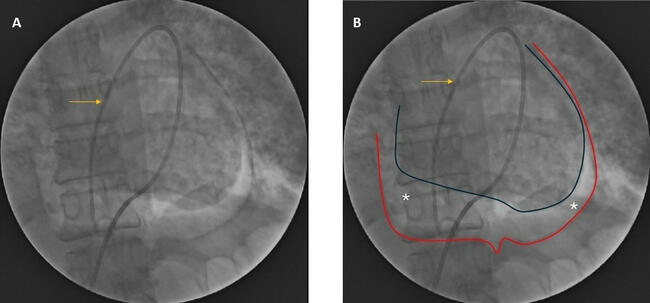
Intraoperatively, we aimed to puncture a well-palpable femoral artery after the anesthesiologist administered a minimal bolus of catecholamines. We performed all of the procedures through the transfemoral approach using two pigtail catheters. One pigtail catheter was positioned in the deepest point of the non-coronary cusp, and the second catheter was positioned in the left coronary cusp through the right radial approach and the contralateral femoral artery (Figure 4).
To position and implant the balloon-expandable valve prostheses, we used TEE combined with radiological images of two pigtail catheters in the aortic root as intraoperative guidance. Valve implantation was systematically performed in a two-step approach. During step 1, the balloon-expandable valve was positioned in the landing zone of the AV annulus under fluoroscopic and echocardiographic guidance and was slowly inflated under fast pacing (130 beats/minute) until we were able to see the inflated balloon under TEE. The position of the valve was re-evaluated by TEE, which presented an opportunity to reposition the valve using the fine-tuning knob on the Edwards Sapien 3 delivery system. The repositioning process was guided by TEE in the long-axis view, which ensured full visualization of the left ventricular outflow tract (LVOT)-aortic annulus-ascending aorta axis, as well as by radiological images of the two pigtail catheters in the aortic root. Step 2 was a rapid pacing phase, which was followed by the full balloon inflation and complete deployment of the valve prosthesis in the selected position (Figure 5).
Intraoperatively, coronary malperfusion was ruled out if the TEE showed no new regional wall-motion abnormalities and if the electrocardiogram was free of any new ischemic changes. Notably, intraoperative TEE was performed by the same anesthesiologist who performed the procedure preoperatively. Femoral access-site complications were ruled out if the clinical examination of the groin was unremarkable and no femoral bruit was heard on auscultation.
Results
The demographic and preoperative data of the entire study cohort are displayed in Table 1. The logistic EuroScore I was 35.4 ± 13.3% in the study group vs 36 ± 12 in the control group, while the Society of Thoracic Surgeons (STS) score was 8.3 ± 2.1% in the study group vs 8.5 ± 2.6% in the control group. All preoperative characteristics were equally distributed in both groups.
Table 2 displays all relevant intraoperative parameters. Most patients in both groups received a 26 mm Edwards Sapien 3 valve. The TEE measurements were the cornerstone of the valve size decision. All implantation procedures were uneventful, without major complications including valve embolization, severe paravalvular leakage, pericardial effusion, and aortic annulus rupture. Intraoperative and early postoperative TEE was extensively used to rule out these complications. Notably, the implantation times recorded in this series ranged between 35-60 minutes, which are very comparable to the standard contrast-guided transcatheter aortic valve replacement (TAVR) procedure.
Post operation, 1 patient (4%) required a pacemaker in the study group due to a total atrioventricular block vs 3 patients (4.1%) in the control group. There was no in-hospital mortality; however, 3 patients died during the 30-day follow-up period (1 patient [4%] in the study group vs 2 patients [2.7%]in the control group; P=.50). The patient in the study group was a multimorbid 83-year-old male with recurrent episodes of cardiac decompensation and pneumonia in addition to aortic stenosis. Furthermore, his surgery was postponed by 3 weeks until he reached a better compensatory state without pneumonia. There were no periprocedural strokes or major vascular complications. All postoperative results are summarized in Table 2.
Discussion
In the present study, we analyzed the procedural outcomes of 25 consecutive transfemoral (TF)-TAVI patients who underwent the procedure without receiving a single dose of contrast medium. All TF-TAVI procedures were performed by the same experienced and institutional TAVI team. Furthermore, we compared the outcomes in the study patients with those of matched patients who underwent TAVI with the use of contrast media.
This study is limited to balloon-expandable TAVR valves because of the opportunity to visualize balloon inflation under TEE guidance. A similar procedure was initially described by Ferrari et al7 in 2010. However, there is a very limited number of case series that report the same “contrast-free” TAVR implantation technique. For instance, Bruschi et al8 and Arigo et al9 published case reports on a contrast-free TAVI with the CoreValve (Medtronic); Latib et al10 published a series of 3 patients who underwent implantation of a Direct Flow valve (Direct Flow Medical) and the use of a single contrast shot to check the femoral closure site; and Leroux et al11 published 1 TAVR case with a balloon-expandable Sapien valve without the use of contrast medium. To the best of our knowledge, the present series represents the largest cohort to date with the TAVR procedure performed without any use of contrast media.
The major difference between our cohort and the study by Ferrari et al7 is the implantation approach; all implantations in our study were performed using the TF approach, whereas the Ferrari study established transapical access. Ferrari et al7 published a series of 30 TAVR patients who underwent the procedure without the use of contrast media in 2010, but all of the procedures were performed with a transapical approach.
During the preoperative work-up, we tried to minimize the amount of contrast medium employed during coronary and iliofemoral angiography before TAVI (mean amount 25 mL, ranging from 23-36 mL) by performing coronary angiogram in a biplane C-arm setting. Another alternative approach to reducing the burden from iodinated contrast medium during coronary angiography is the use of gadolinium; because of their different chemical structures, gadolinium and iodinated contrast have no cross-reactivity in patients with iodine allergies, and gadolinium has a lower nephrotoxicity at the recommended doses than iodinated contrast media.12
At 30-day follow-up, the composite endpoint of death from any cause, valve embolization, vascular complications, cerebrovascular complications, pacemaker implantation, and postoperative myocardial infarction was equally distributed between both groups, and was comparable with previous studies.1,3 Our initial focus was to monitor renal function during the postoperative follow-up period. One patient in the study group developed a postoperative acute kidney injury, which could potentially be explained by the use of general anesthesia and the hemodynamic effect of the implantation procedure in very high-risk patients. However, contrast-induced nephropathy was significantly higher in patients who received contrast media (15 patients [20.5%] in control group vs 1 patient [4%] in the study group; P=.04).
The 30-day mortality rate of this high-risk study cohort that underwent TF-TAVI without CM was 4.0%, which compares well with other contemporary studies on TAVI patients.1-3
In our study protocol, accurately performing annular sizing was another challenge. For this purpose, our anesthesiology team was specifically trained to obtain the TEE measurements needed to follow the method of Bleakely et al.13 An additional native CT scan was used as a second imaging tool for reference. Furthermore, before starting this program, we performed an internal validation of our AV annular measurements by comparing the TEE measurements with those obtained with “contrast-enhanced” CT scans in a retrospective cohort from our institution. Based on this retrospective analysis, we decided to completely abandon the contrast-enhanced CT examination in this specific patient cohort and performed only TEE-based annular measurements.
Chaturvedi et al reported that magnetic resonance imaging (MRI)-based AV annular measurements were superior to the CT-based measurements.12 In the future, MRI could be a useful diagnostic tool for contrast-free TAVI programs if this modality can successfully replace multislice CT measurements.12
In the contrast-free TAVI technique, the use of TEE is mandatory, which limits the TAVR procedure to being performed under general anesthesia and, unfortunately, completely precludes the possibility of adapting TAVI to being performed under local anesthesia.
Future prospects. Admittedly, a valuable piece of information was always missing when performing this implantation technique. The angulation of the TAVR implantation plane could only be obtained through contrast CT, which this study aimed to avoid. For this purpose, we reviewed all relevant published literature and consulted radiology experts to learn how to obtain the angulation of the implantation plane from the native multislice CTs. According to the protocol published by Bruschi et al in 2015,8 this measurement could be obtained from native electrocardiography-gated multislice CT. From the double-oblique transverse images, three points are positioned at the most inferior aspects of the severely calcified valve cusps. The implantation projection was determined when the triangle that connected all three points was not evident and was replaced by a single line, with the point of the right cusp equidistant from the left and non-coronary cusps. Carbon dioxide and digital subtraction angiography can be safely used in patients with nephropathy to assess the femoral artery anatomy; in this technique, carbon dioxide is used instead of the iodinated contrast material. Ultrasound-guided femoral artery puncture could be used to reduce access-related complications.14
Conclusion
Our initial experience demonstrates the safety and reproducibility of contrast-free TAVR procedures using balloon-expandable valves. In addition, it significantly reduced the incidence of postoperative acute kidney injury in patients with severe nephropathy.
*Joint first authors.
From the 1Heart Center, Zentralklinik, Bad Berka, Germany; 2Department of Cardiothoracic Surgery, Cairo University, Giza, Egypt; 3Department of Cardiology, Minia University, Minia, Egypt; 4Department of Internal Medicine I, Division of Cardiology, Pneumology, Angiology and Intensive Medical Care, University Hospital Jena, Friedrich-Schiller-University Jena, Jena, Germany 5Department of Anesthesia, Zentralklinik, Bad Berka, Germany; and the 6Department of Cardiovascular Surgery, University Heart Center, Hamburg, Germany.
Funding: Dr Owais is the main investigator of the undergoing APACE TREAT S3 study, funded by Edwards Lifesciences.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted February 2, 2020 and accepted February 12, 2020.
Address for correspondence: Tamer Owais, MD, PhD, Department of Cardiac Surgery, Central Clinic Bad Berka, Robert-Koch Allee 9, 99437 Bad Berka, Germany. Email: tamerowaiss1976@yahoo.com
- Thyregod HG, Steinbrüchel DA, Ihlemann N, et al. Transcatheter versus surgical aortic valve replacement in patients with severe aortic valve stenosis: 1-year results from the all-comers NOTION randomized clinical trial. J Am Coll Cardiol. 2015;65:2184-2194.
- Yamamoto M, Hayashida K, Mouillet G, et al. Prognostic value of chronic kidney disease after transcatheter aortic valve implantation. J Am Coll Cardiol. 2013;62:869-877.
- Sinning J-M, Ghanem A, Steinhäuser I-I, et al. Renal function as predictor of mortality in patients after percutaneous transcatheter aortic valve implantation. JACC Cardiovasc Interv. 2010;3:1141-1149.
- Bagur R, Webb JG, Nietlispach F, et al. Acute kidney injury following transcatheter aortic valve implantation: predictive factors, prognostic value, and comparison with surgical aortic valve replacement. Eur Heart J. 2010;31:865-874.
- Perrin T, Descombes E, Cook S. Contrast-induced nephropathy in invasive cardiology. Swiss Med Wkly. 2012;142:w13608.
- Briguori C, Airoldi F, D’Andrea D, et al. Renal insufficiency following contrast media administration trial (REMEDIAL): a randomized comparison of 3 preventive strategies. Circulation. 2007;115:1211-1217.
- Ferrari E, Sulzer C, Marcucci C, et al. Transapical aortic valve implantation without angiography: proof of concept. Ann Thorac Surg. 2010;89:1925-1932.
- Bruschi G, Colombo P, De Marco F, Barosi A, Mauri S, Klugmann S. Self-expandable CoreValve implantation without contrast media. Asian Cardiovasc Thorac Ann. 2016;24:696-698.
- Latib A, Maisano F, Colombo A, et al. Transcatheter aortic valve implantation of the direct flow medical aortic valve with minimal or no contrast. Cardiovasc Revasc Med. 2014;15:252-257.
- Arrigo M, Maisano F, Haueis S, Binder RK, Taramasso M, Nietlispach F. Transcatheter aortic-valve implantation with one single minimal CM injection. Catheter Cardiovasc Interv. 2015;85:1248-1253.
- Leroux L, Dijos M, Dos Santos P. Successful transfemoral aortic Edwards Sapien bioprosthesis implantation without using iodinated contrast medium in a woman with severe allergy to contrast agent. Catheter Cardiovasc Interv. 2013;82:E947-E951.
- Chaturvedi A, Hobbs SK, Ling FS, Chaturvedi A, Knight P. MRI evaluation prior to transcatheter aortic valve implantation (TAVI): when to acquire and how to interpret. Insights Imaging. 2016;7:245-254.
- Bleakley C, Eskandari M, Monaghan M. 3D transoesophageal echocardiography in the TAVI sizing arena: should we do it and how do we do it? Echo Res Pract. 2017;4:R21-R32.
- Elbaz-Greener G, Zivkovic N, Arbel Y, Radhakrishnan S, Fremes SE, Wijeysundera HC. Use of two-dimensional ultrasonographically guided access to reduce access-related complications for transcatheter aortic valve replacement. Can J Cardiol. 2017;33:918-924.