

Transcollateral Approach for Percutaneous Revascularization of Complex Superficial Femoral Artery Chronic Total Occlusion
Download a PDF of this article.
ABSTRACT: Chronic total occlusions of the superficial femoral artery occur in approximately 40% of patients with symptomatic peripheral arterial disease. When antegrade revascularization fails or is not feasible, a retrograde approach should be considered. This is usually via the popliteal or tibial vessels. Alternatively, transcollateral revascularization has been reported. This report describes the use of transcollateral retrograde revascularization of the superficial femoral artery in two patients with failed antegrade crossing. Retrograde recanalization was achieved via a branch of the profunda femoris artery. Unlike previous reports that describe retrograde crossing and subsequent snaring of the wire, these cases were performed with retrograde passage of a low-profile balloon. Following retrograde balloon dilation, the vessel was rewired from an antegrade approach and the procedure was completed with complications.
J INVASIVE CARDIOL 2013;25(5):E96-E100
Key words: retrograde recanalization, superficial femoral artery
____________________________________________
Recent advances in endovascular techniques and procedures have resulted in recommending an initial percutaneous approach for TransAtlantic Inter-Society Consensus (TASC) class A and B lesions.1 Surgical revascularization remains the preferred treatment for longer lesions (class D) and some class C lesions depending on patient risk and operator experience.1 However, high rates of success have been demonstrated in endovascular treatment of class C and D lesions.2,3 Chronic total occlusion (CTO) of the superficial femoral artery (SFA) occurs in approximately 40% of patients with symptomatic peripheral arterial disease (PAD).4 Recanalization of these lesions may prove to be challenging, with true lumen crossing occurring 40%-60% of the time; in addition, procedure times can be lengthy and the patient may be subject to increased dye load.5 The advent of multiple crossing devices has allowed for decreasing crossing time as well as facilitating distal reentry. Alternative approaches include subintimal angioplasty or a retrograde approach utilizing either the popliteal, tibial or pedal artery for access. Transcollateral access has also been described for below-the-knee occlusive disease with limited reports for the SFA.6,7 This case describes transcollateral revascularization of the SFA by a different technique than previously reported.
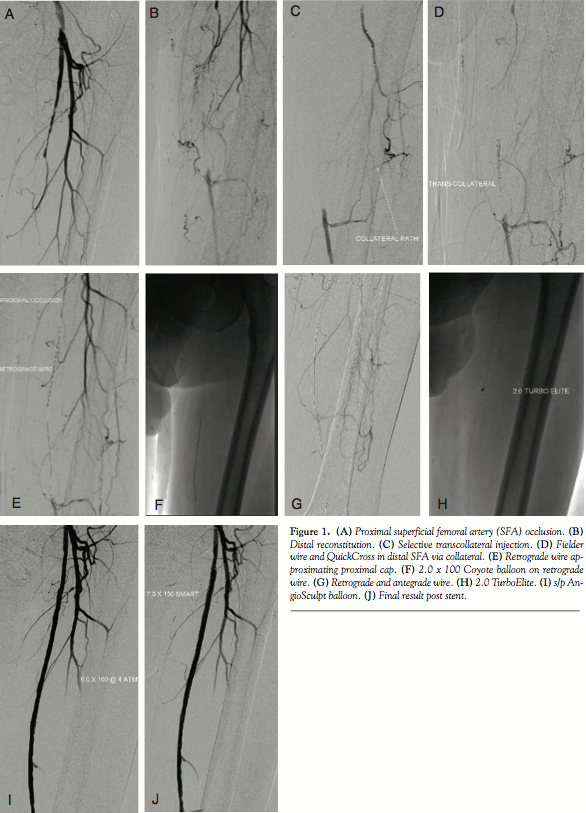 Case Report. A 65-year-old male presented with a history of atrial fibrillation, non-ischemic cardiomyopathy, tobacco abuse, hypertension and hypercholesterolemia. He had been complaining of progressive claudication. He was started on a trial of medical therapy including smoking cessation, cilostazol, and a walking program. The patient continued to smoke and despite medical therapy complained of lifestyle-limiting claudication. He underwent diagnostic angiography and was found to have high-grade stenosis of the right SFA and complete occlusion of the left SFA (Figures 1A and 1B) and two-vessel run-off with an occluded anterior tibial artery. He was referred for percutaneous revascularization of the left SFA.
Case Report. A 65-year-old male presented with a history of atrial fibrillation, non-ischemic cardiomyopathy, tobacco abuse, hypertension and hypercholesterolemia. He had been complaining of progressive claudication. He was started on a trial of medical therapy including smoking cessation, cilostazol, and a walking program. The patient continued to smoke and despite medical therapy complained of lifestyle-limiting claudication. He underwent diagnostic angiography and was found to have high-grade stenosis of the right SFA and complete occlusion of the left SFA (Figures 1A and 1B) and two-vessel run-off with an occluded anterior tibial artery. He was referred for percutaneous revascularization of the left SFA.
The right common femoral artery was accessed using a 4 Fr micropuncture kit (Cook Medical).The sheath was upsized to a 5 Fr Avanti sheath (Cordis Corporation); using a 5 Fr IMA catheter (Boston Scientific) and an exchange-length glidewire (Terumo Corporation), the catheter was advanced into the left common femoral. The sheath was then upsized to a 6 Fr, 45 cm Pinnacle destination sheath (Terumo Corporation) placed in the origin of the left SFA. After administration of heparin, an Asahi Miracle Bros 6 wire (Abbott) was advanced to the cap. A Wildcat catheter (Avinger) was then advanced over the wire distally. An attempt to engage the cap resulted in deflection of the Wildcat into the collateral. Several attempts were made using the back end of the wire advanced to the distal tip of the catheter to provide more support while utilizing the Wildcat in different modes. Repeated attempts resulted in advancement of the device into the collateral branch. Next, an angled 0.18˝ QuickCross Extreme (Spectranetics) was used with a Treasure 12 guidewire (Abbott). Multiple attempts were made to advance the Treasure 12 wire into the proximal cap. It was felt this might allow advancement of the Wildcat to the cap without concern of deflecting into the collateral. Unfortunately, the proximal cap could not be penetrated secondary to the calcium as well as the angle and presence of a collateral. At this point, consideration was given to using an angled glidewire and QuickCross catheter and attempt a subintimal approach or bring the patient back for popliteal access. After further examination of the angiograms and angulated views (ipsilateral 20°), it was felt that there was an adequate collateral to attempt transcollateral passage of a wire. The destination sheath was withdrawn into the left common femoral and the wire was advanced into the collateral utilizing a Runthrough wire (Terumo Corporation) and a Finecross catheter (Terumo). Due to poor visualization of the catheter, the Finecross was exchanged for a 0.14˝ QuickCross and the wire was exchanged for a 300 cm Asahi Fielder wire (Abbott). Selective injection was then performed of the collateral through the QuickCross (Figure 1C). The Fielder wire was negotiated through the collateral and into the distal lumen of the SFA (Figure 1D). The 0.14˝ QuickCross was then advanced into the SFA in a retrograde manner and the wire was changed to an Asahi Confienza wire (Abbott). The wire was advanced in a retrograde manner through the calcified lesion to the proximal cap (Figure 1E). The cap could not be penetrated despite attempts with several wires (Confienza, Cross-It, Pilot 300). At this time, the 0.14˝ QuickCross was exchanged for an 0.18˝ QuickCross through the collateral in a retrograde manner. The wire was then changed to a Treasure 12 wire, which easily penetrated the cap. The wire was then advanced into the left common femoral artery and exchanged for a Runthrough wire. Several attempts were made to rewire the sheath or rewire an angled catheter. This was in order to externalize the wire and proceed with revascularization. These attempts were unsuccessful. Multiple attempts were made to snare the wire by utilizing a 2.0 mm loop snare (eV3). This also was unsuccessful. At this point a 2.0 x 100 Coyote balloon (Boston Scientific) was advanced via the collateral into the lesion in a retrograde manner. The vessel was dilated at 6 atm for 20 seconds (Figure 1F). At this point, a Fielder wire was easily advanced in an antegrade manner into the tibioperoneal vessel and then exchanged for a RunThrough wire (Figure 1G). A 2.0 TurboElite Laser fiber (Spectranetics ) was then utilized to debulk and modify the plaque as well as facilitate balloon delivery (Figure 1H). The lesion was predilated with a 6.0 x 100 AngioSculpt scoring balloon at 4 atm x 2 minutes (Figure 1I). This was performed in an overlapping manner. This was then followed by placement of a 7.0 x 150 SMART stent (Cordis), which was postdilated with a 7.0 x 100 Sterling balloon (Boston Scientific) at 4 atm (Figure 1J). Final angiography demonstrated brisk flow without embolization, perforation, or dissection. The sheath was withdrawn and a Mynk closure (AccessClosure) was performed of the right groin. The patient was discharged home the following morning without incident.
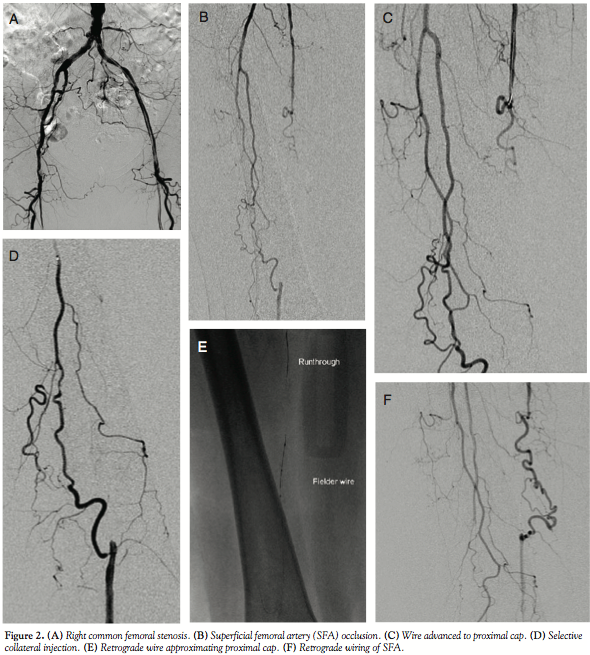 Case 2. An 83-year-old female presented with a history of coronary bypass, left aortofemoral bypass, bilateral carotid endarterectomy, right subclavian bypass, cerebral vascular accident, percutaneous coronary intervention (PCI) of native circumflex, hypertension, hypercholesterolemia, continued tobacco abuse, and claudication. The patient developed an ulceration on the hallux of the right foot and had a known ankle-brachial index of 0.45 on the right lower extremity. Angiography revealed a high-grade stenosis of the right common femoral and occlusion of the SFA (Figures 2A and 2B). She was referred for percutaneous revascularization.
Case 2. An 83-year-old female presented with a history of coronary bypass, left aortofemoral bypass, bilateral carotid endarterectomy, right subclavian bypass, cerebral vascular accident, percutaneous coronary intervention (PCI) of native circumflex, hypertension, hypercholesterolemia, continued tobacco abuse, and claudication. The patient developed an ulceration on the hallux of the right foot and had a known ankle-brachial index of 0.45 on the right lower extremity. Angiography revealed a high-grade stenosis of the right common femoral and occlusion of the SFA (Figures 2A and 2B). She was referred for percutaneous revascularization.
The left groin was accessed with a 4 Fr micropuncture kit (Cook) and upsized to a 5 Fr femoral sheath (Cordis). An Omni catheter was used to cross over to the left side and the sheath was exchanged for a 45 cm, 6 Fr destination sheath (Terumo) placed in the right common femoral artery. Heparin was administered and a Runthrough wire (Terumo) was advanced to the SFA occlusion (Figure 2C). The occlusion involves the take-off of a collateral and there was no “beak” to advance the wire into or for directing a crossing device. Rather than risk a subintimal passage, an additional Runthrough wire was advanced into the profunda with a 0.14˝ QuickCross catheter (Spectranetics). The collateral pathway was engaged (Figure 2D) and the wire was exchanged for a Fielder wire (Abbott). The Fielder, with the support of the QuickCross, was advanced through the collateral into the distal SFA via the retrograde approach (Figure 2E). The wire was then exchanged for an Asahi Confianza wire (Abbott), which was used to wire the SFA in a retrograde manner  (Figure 2F). Given the previous experience from case 1, a 2.0 x 40 Coyote balloon (Boston Scientific) was advanced via the collateral rather than attempting to snare the wire from above (Figure 2G). Following predilation via retrograde approach (Figure 2H), a Runthrough wire was easily advance distally from the antegrade approach (Figure 2I). The vessel was then predilated with a 3.0 x 120 VascTrak balloon (Bard). Intravascular ultrasound (IVUS; Volcano Corporation) was then performed to size the vessel, which was a 4.0 mm vessel with evidence of calcification and diffuse disease. The vessel was dilated with a 4.0 x 150 Coyote at 4 atm for 3 minutes. There was one area of focal calcification that did not yield with balloon inflation; this was addressed with a 3.0 x 20 AngioSculpt (Angioscore) at 22 atm followed by low-pressure inflation with the 4.0 x 150 Coyote.
(Figure 2F). Given the previous experience from case 1, a 2.0 x 40 Coyote balloon (Boston Scientific) was advanced via the collateral rather than attempting to snare the wire from above (Figure 2G). Following predilation via retrograde approach (Figure 2H), a Runthrough wire was easily advance distally from the antegrade approach (Figure 2I). The vessel was then predilated with a 3.0 x 120 VascTrak balloon (Bard). Intravascular ultrasound (IVUS; Volcano Corporation) was then performed to size the vessel, which was a 4.0 mm vessel with evidence of calcification and diffuse disease. The vessel was dilated with a 4.0 x 150 Coyote at 4 atm for 3 minutes. There was one area of focal calcification that did not yield with balloon inflation; this was addressed with a 3.0 x 20 AngioSculpt (Angioscore) at 22 atm followed by low-pressure inflation with the 4.0 x 150 Coyote.
There was a small dissection noted that was covered with a 5.0 x 40 EverFlex self-expanding stent (EV3) (Figure 2J). IVUS had revealed that the common femoral artery was approximately 6 mm; therefore, balloon dilation was performed with a 6.0 x 20 AngioSculpt. Final IVUS revealed a 5 mm lumen in the CFA with no gradient measured with the sheath; therefore, no stent was placed (Figure 2K). Final angiography revealed good flow to the foot without evidence of embolization or perforation. The left groin was closed with a Mynx closure device. The patient was discharged without incident.
Discussion. Endovascular treatment of chronically occluded infrainguinal vessels is a reasonable alternative to conventional bypass with good success rates and low perioperative morbidity and mortality.3 CTOs are commonly encountered in the SFA. There are various endovascular approaches to recanalize the vessel including the use of subintimal angioplasty, blunt catheter dissection, laser atherectomy, specialty crossing tools, and retrograde recanalization via the popliteal or tibioperoneal vessels.
A major limitation of endovascular revascularization is failure of true lumen crossing. Subintimal crossing is acceptable, but may result in failure to reenter distally even with the assistance of reentry devices.8 There are currently several crossing devices (Crosser, Wildcat, TruePath, Front Runner) available to facilitate crossing complex total occlusions. The principle is to remain intraluminal (true lumen) or create a controlled subintimal track with the use of a reentry catheter to complete the crossing. Success with these devices will vary with operator experience and these devices may not be available in every facility. Failure to cross is usually due to several reasons, ie, inability to keep the wire luminal, heavy calcification, and the presence of collaterals at the site of occlusion.
If the antegrade approach is unsuccessful, it may become necessary to obtain retrograde access, usually via the popliteal artery. However, if femoral access is already obtained and anticoagulation administered, then it becomes difficult to “flip” the patient from the supine position. Alternatively, one could bring the patient back for planned popliteal access. Also, patients with atherosclerotic disease of the popliteal artery may not be suitable for this approach. The transpedal and tibioperoneal vessels may serve as alternative access points; however, the small lumen of these vessels may make access difficult. Potential complications include perforation, dissection, and acute closure of the vessel. If there are inadequate collaterals or further revascularization is not feasible, the consequences could prove significant.
Transcollateral revascularization is an alternative approach to failed antegrade access. Proposed hypotheses for success via this route include: (1) existence of channels with crossable stump at the distal end of the occlusion; and (2) different pathology at the distal occlusion with a softer distal cap.9,10 It has been reported for coronary arteries11 as well as infrapopliteal arteries12 with limited reports for recanalization of the SFA.6,7 In contrast to previous case reports that involve snaring of the transcollateral wire to complete the procedure, we advanced a balloon through the collateral to dilate the vessel in a retrograde manner. Retrograde passage of the balloon and dilatation of the SFA allowed antegrade passage of a guidewire and successful revascularization without additional access or subintimal angioplasty.
In lesions with unfavorable angiographic findings (occlusion at a collateral, calcium), the transcollateral should be considered if antegrade access is unsuccessful. This approach is minimally invasive, the patient is not required to be repositioned, and additional access is not necessary. It obviates the need to place the patient in the prone position for popliteal access and thereby avoid any potential bleeding complications associated with that access site. The transcollateral wire may serve to “open” the artery via retrograde passage, or be used as a roadmap for an antegrade wire or a reentry technique. This approach may be of benefit when there is a proximal occlusion without a visible stump, a collateral at the site of the occlusion, failure to penetrate the proximal cap, or when the antegrade approach has resulted in a dissection.
Potential complications of this procedure would include perforation or loss of the collateral. Compromise of a collateral could possibly result in limb ischemia depending on the size of the collateral and the extent of collateralization. In the event this occurs, surgical bail-out may be required to prevent limb loss if the collateral is not recanalized. Use of a floppy-tip wire to navigate the collateral may minimize this risk. The wire can then be switched to a CTO wire in the reconstituted vessel through a support catheter. In addition, low-profile peripheral balloons (Amphirion, Coyote) or coronary balloons, support catheter (QuickCross), microcatheter (Corsair, Finecross, Tornus), and exchange-length guidewires are needed. The microcatheters have a low crossing profile comparable to the peripheral balloons, 0.017˝ (Coyote, Amphirion); however, they have the advantage of added support. The Corsair has the lowest crossing profile of the available microcatheters. It consists of 8 thin wires wound with 2 larger wires and was originally designed as a collateral channel dilator.
This technique appears technically plausible in patients who may have unfavorable anatomy for antegrade crossing, are not suitable for popliteal or transpedal access, or there is concern about extending a subintimal track into a “no stent” zone. The major limitation of this technique is absence of an adequate collateral for wiring as well as angulation and kinking of the collateral. Given the advent of newer crossing devices and techniques, this approach may be limited to a secondary approach in which conventional crossing has failed. Caution should be used when applying this technique in a claudicant (vs limb salvage), as there is the potential risk of causing acute limb ischemia if there is compromise of the collateral.
In conclusion, the transcollateral technique should be part of the interventionalist’s repertoire and considered either electively (antegrade access fails) or urgently (antegrade access is complicated by dissection or perforation or retrograde access is not feasible). Angulated views and selective injection (via profunda) may minimize overlap and allow better visualization of the transcollateral path. Use of low-profile balloons, support catheters, and a variety of exchange-length guidewires may increase the success of this approach.
References
- Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, Fowkes FG. Intersociety consensus for the management of peripheral arterial disease (TASC II). J Vasc Surg. 2007;45(Suppl S):S5-S67.
- Conrad MF, Cambria RP, Stone DH, B, et al. Intermediate result of percutaneous endovascular therapy of femoropopliteal occlusive disease: a contemporary series. J Vasc Surg. 2006;44(4):762-769.
- Rabellino M, Zander T, Baldi S, et al. Clinical follow-up in endovascular treatment for TASC C-D lesions in femoro-popliteal segment. Cathet Cardiovasc Interv. 2009;73(5):701-705.
- Boguszewski A, Torey J, Pai R, et al. Intraluminal recanalization of SFA CTOs. Endovascular Today. 2010;9:33-38.
- Bolia A, Miles KA, Brennan J, et al. Percutaneous transluminal angioplasty of occlusions of the femoral and popliteal arteries by subintimal dissection. Cardiovasc Intervent Radiol. 1990;13(6):357-363.
- Urasawa K, Sato K, Koshida R, Honma Y. Transcollateral angioplasty for the treatment of long chronic total occlusions of superficial femoral arteries: a novel wiring technique. J Cardiovasc Surg (Torino). 2011 Jul 28 (Epub ahead of print).
- Zander T, Gonzalez G, De Alba L, Rivero O, Maynar M. Transcollateral approach for percutaneous revascularization of complex superficial femoral artery and tibioperoneal trunk occlusions. J Vasc Interv Radiol. 2012;23(5):691-695.
- Bausback Y, Botsios S, Flux J, et al. Outback catheter for femoropopliteal occlusions: immediate and long-term results. J Endovasc Ther. 2011;18(1):13-21.
- Ozawa N. A new understanding of chronic total occlusion from a novel PCI technique that involves a retrograde approach to the right coronary artery via a septal branch and passing of the guidewire to a guiding catheter on the other side of the lesion. Catheter Cardiovasc Interv. 2006;68(6):907-913.
- Rosenmann D, Meerkin D, Almagor Y. Retrograde dilatation of chronic total occlusionstrans-collateral vessel in three patients. Catheter Cardiovasc Interv. 2006;67(2):250-253.
- Saito S. Different strategies of retrograde approach in coronary angioplasty for chronic total occlusion. Catheter Cardiovasc Interv. 2008;71(1):8-19.
- Fusaro M, Agostoni P, Biondi-Zoccai G. ‘‘Trans-collateral" angioplasty for a challenging chronic total occlusion of the tib- ial vessels: a novel approach to percutaneous revascularization in critical lower limb ischemia. Catheter Cardiovasc Interv. 2008;71(2):268-272.
__________________________________________
From the Department of Cardiology, Winter Haven Hospital, Winter Haven, Florida.
Disclosure: The author has completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Tai is on the speaker’s bureau for Terumo, Spectranetics, and Boston Scientific (radial, laser and rotational atherectomy, respectively).
Manuscript submitted October 9, 2012, provisional acceptance given October 29, 2012, final version accepted November 26, 2012.
Address for correspondence: Zaheed Tai, DO, FACC, FSCAI, 635 First Street North, Winter Haven, FL 33881. Email: zaheedtai@gmail.com










