

Transfemoral Implantation of the Acurate neo for the Treatment of Aortic Regurgitation
Abstract: Objectives. We report an international experience of transfemoral transcatheter aortic valve replacement (TAVR) using the self-expanding Acurate neo valve (Boston Scientific) in aortic regurgitation. Methods. This series comprises 20 patients with pure aortic regurgitation undergoing transfemoral TAVR with the Acurate neo prosthesis at nine centers in Europe and Israel. Results. Mean age was 79 ± 8 years and mean STS score was 8.3 ± 9.3%. Leaflet calcification was none/minimal in 19 patients (95%). Prosthesis size selection was based on perimeter-derived annular diameter, with a tendency to over-size in cases of borderline annuli. One patient required implantation of a second valve. Device success rate was 18/20 (90%). At discharge, aortic regurgitation was none in 14 patients (70%), mild in 5 patients (25%), and moderate in 1 patient (5%). Left ventricular end-diastolic diameter decreased from 58 ± 7 mm at baseline to 53 ± 7 mm before discharge (P<.001). At 30-day follow-up, there was no mortality, no stroke, and 3 patients (15%) had received a permanent pacemaker. New York Heart Association class had improved significantly compared to baseline (85% in class I/II compared to 15% at baseline; P<.001). Conclusions. In a selected patient population, transfemoral TAVR using the Acurate neo transcatheter heart valve was successful in treating aortic regurgitation, significantly reduced left ventricular dimensions, and improved clinical symptoms.
J INVASIVE CARDIOL 2018;30(9):329-333. Epub 2018 July 15.
Key words: aortic regurgitation, degenerative valve, femoral, transcatheter aortic valve implantation, transcatheter aortic valve replacement
Transcatheter aortic valve replacement (TAVR) is an established therapy for intermediate and high-risk patients with severe aortic stenosis.1,2 In addition, TAVR has been performed off-label to treat patients with pure aortic regurgitation.3-8 While open-heart surgery clearly remains the gold standard for the treatment of aortic regurgitation, some high-risk patients may benefit from a less invasive, percutaneous procedure.
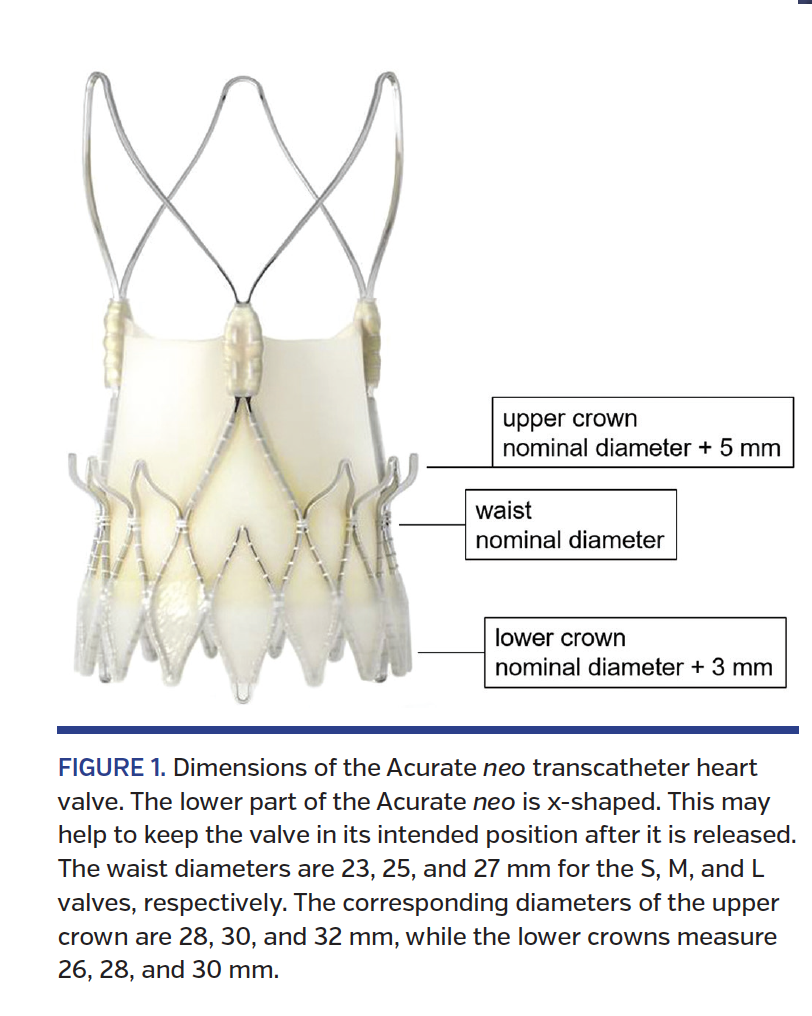
The self-expanding Acurate neo transfemoral system (Boston Scientific) received the CE mark in 2014 and has design features that may help to anchor the valve even in the absence of calcification.9-11 In particular, the lower part of the transcatheter heart valve (THV) has an x-shaped design with an upper crown 5 mm larger than the nominal THV diameter, which may help to anchor the prosthesis and prevent it from embolization into the left ventricle once released (Figure 1).
We report an international experience with transfemoral TAVR using the Acurate neo THV for the treatment of pure aortic regurgitation.
Methods
Study population and design. This is an independent, multicenter registry retrospectively including patients with severe aortic regurgitation treated with the Acurate neo THV via transfemoral access. Between May 2015 and July 2017, a total of 20 patients at nine centers in Europe and Israel were included. Data were collected and entered in the database by the respective centers and comprised data throughout the initial hospital stay and 30-day data including echocardiographic follow-up. All patients provided written informed consent for prospective data acquisition and follow-up examinations.
TAVR work-up and procedure. The Acurate neo THV device and its implantation have been described previously.9,10,12 In our series, potential TAVR candidates were discussed by an interdisciplinary heart team consisting of non-invasive cardiologists, interventional cardiologists, and cardiac surgeons. The decision of whether or not a patient would be suitable for percutaneous treatment with the Acurate neo THV was made by the local heart teams. All patients underwent electrocardiography-gated multidetector computed tomography for annular measurements. The valve size was chosen according to the annulus perimeter (a small “S” valve for annular perimeters <72 mm, a medium “M” valve for annular perimeters between 72 and 78 mm, or a large “L” valve if the perimeter was between 79 and 84 mm). In borderline cases, the larger valve was preferred. The patient with the largest annulus included in this series had a perimeter of 82 mm. Due to the absence of calcification, there was no predilation or postdilation required. Following TAVR, patients were monitored for 1-3 days, depending on the presence of a bundle-branch block or an atrioventricular block. All patients underwent echocardiographic follow-up prior to discharge and at 30-day follow-up.
Statistical analysis. Clinical endpoints were defined according to the updated definitions of the Valve Academic Research Consortium consensus document.13 If not otherwise indicated, data are presented as mean ± standard deviation for continuous variables and as numbers and frequencies for categorical variables. Paired continuous parametric variables were compared using the paired Student’s t-test. Paired categorical variables (New York Heart Association [NYHA] class) were compared using the Wilcoxon signed rank test. Statistical analyses were conducted with STATA version 13 (StataCorp) and tested using two-sided tests at a significance level of .05.
Results
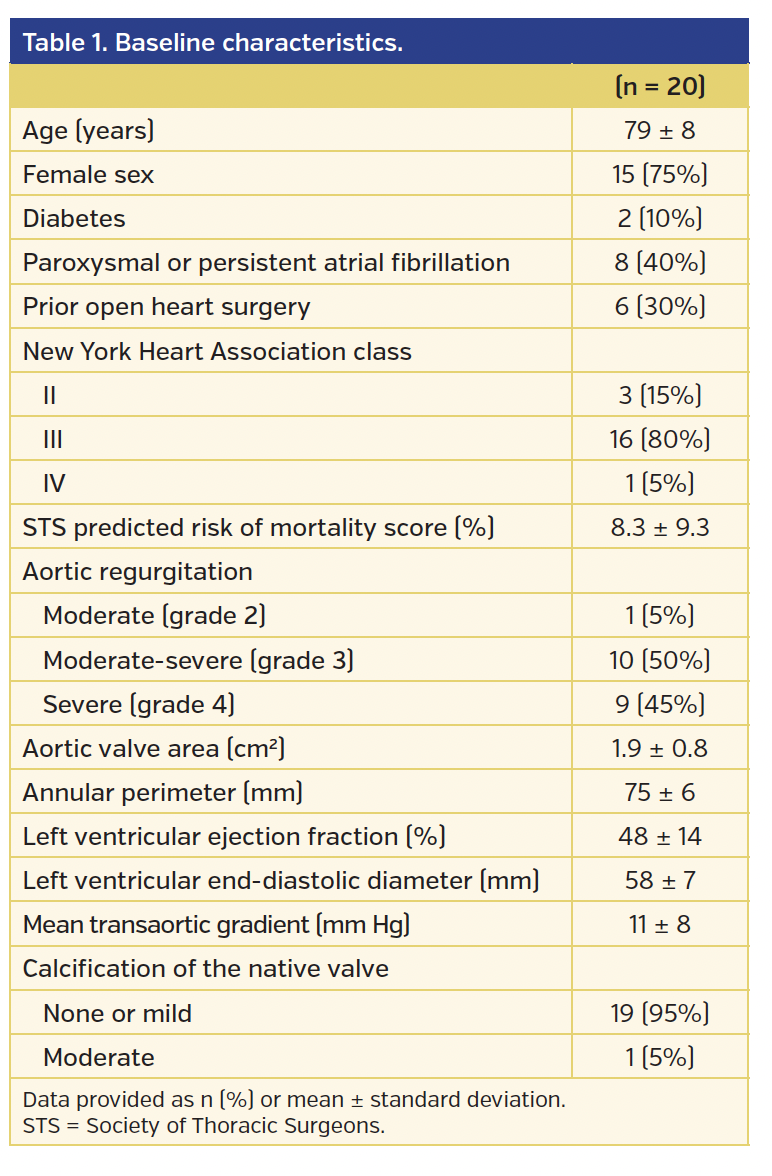
Twenty patients (15 women and 5 men; mean age, 79 ± 8 years) underwent transfemoral TAVR with the Acurate neo for the treatment of pure aortic regurgitation at nine centers in Europe and Israel (Figure 2). Mean STS predicted risk of mortality score was 8.3 ± 9.3% and 17 patients (85%) were in NYHA class III or IV. The underlying cause for regurgitation was leaflet degeneration in 13 patients (65%), prolapse in 6 patients (30%), and leaflet injury in 1 patient (5%). Leaflet calcification was none/minimal in 19 patients (95%), and 1 patient (5%) had moderate calcification. Baseline characteristics are summarized in Table 1.
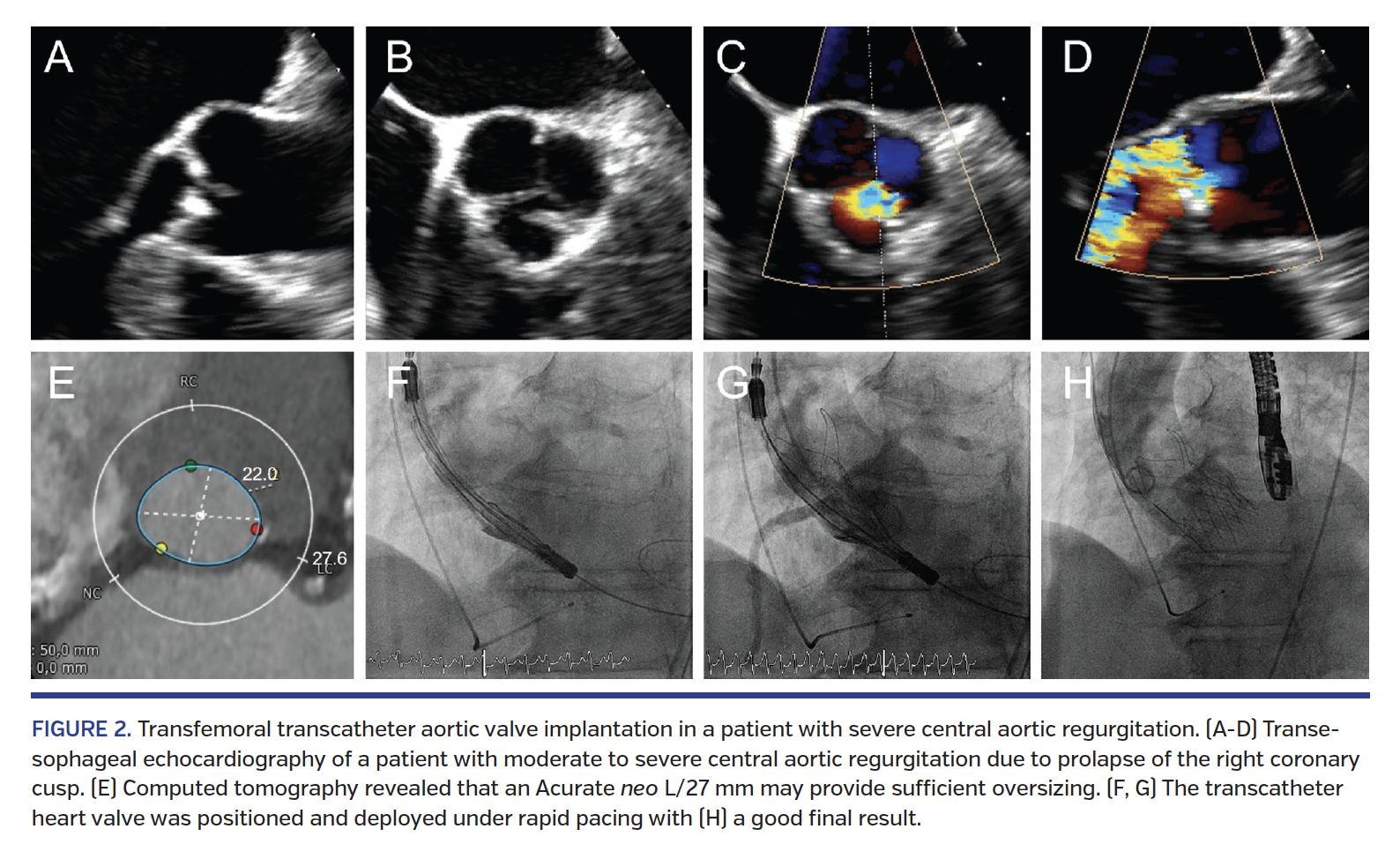
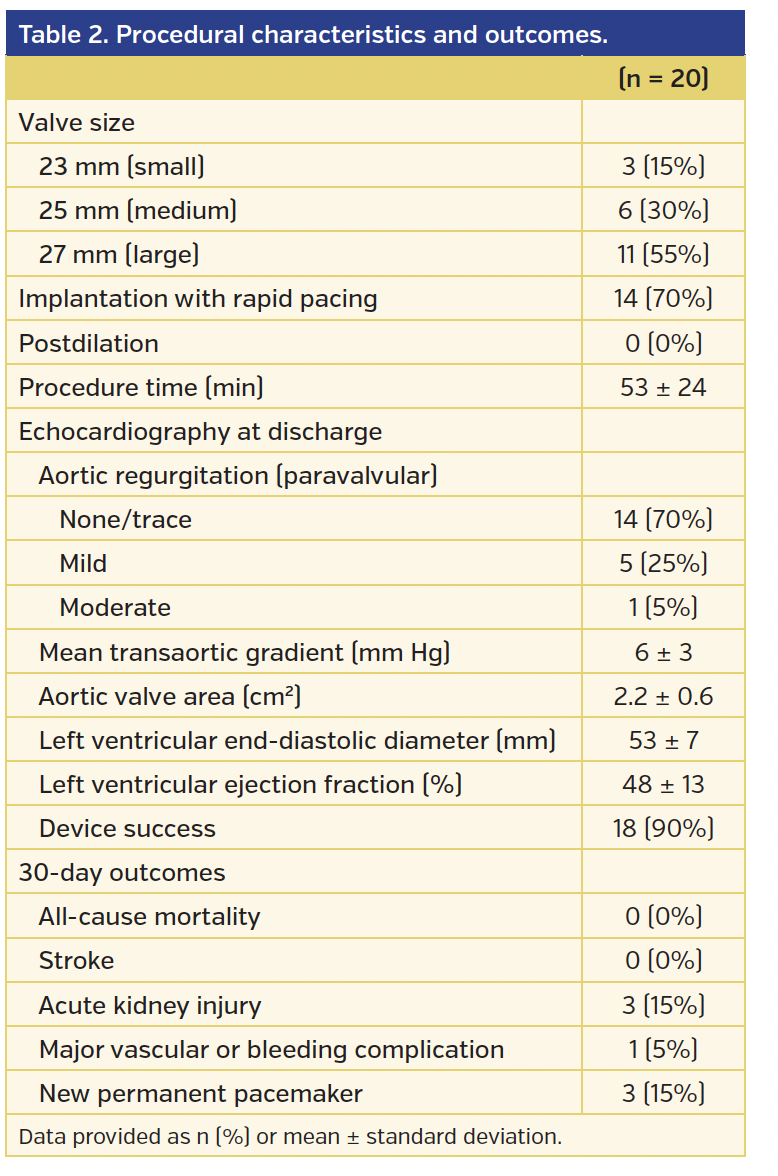
TAVR procedure. Procedural characteristics and outcomes are presented in Table 2. The mean perimeter-derived annular diameter was 24 ± 2 mm, the long-axis diameter was 26 ± 2 mm (range, 23-30 mm), and the short-axis diameter was 21 ± 2 mm (range, 18-25 mm). Valve size selection was based on the perimeter-derived annular diameter as measured by computed tomography, with a tendency to over-size in cases of borderline measurements resulting in a mean over-sizing of 9 ± 4% (compared to a nominal diameter of 23, 25, and 27 mm for the S, M, and L valves, respectively). No predilation was performed due to the absence of calcification. To achieve greater stability during release, valves were implanted with rapid pacing in 13 patients (70%). Targeted initial positioning was about 5 mm below the annular level and final implantation depth was 7 ± 4 mm. In 1 patient, implantation of a second THV (Sapien 3; Edwards Lifesciences) was required due to a too-low (ventricular) position of the Acurate neo prosthesis resulting in severe paravalvular regurgitation. Mean procedure duration (from puncture to access closure) was 53 ± 24 minutes.
Outcomes. Median hospitalization duration was 9 days (range, 6-14 days). Transthoracic echocardiography prior to discharge revealed no paravalvular regurgitation in 14 patients (70%), mild paravalvular regurgitation in 5 patients (25%), and moderate paravalvular regurgitation in 1 patient (5%; P<.001 compared to baseline). There was no transvalvular regurgitation. Mean transvalvular gradient was 6 ± 3 mm Hg (P=.01 compared to baseline). Left ventricular end-diastolic diameter decreased from 58 ± 7 mm at baseline to 53 ± 7 mm before discharge (P<.001), and left ventricular ejection fraction remained unchanged.
Up to 30 days of follow-up, no patient died and no stroke was observed, 3 patients (15%) had received a permanent pacemaker (all due to high-degree atrioventricular block), and 17 patients (85%) were in NYHA class I or II (P<.001 compared to baseline).
After a median follow-up of 124 days, there was no evidence of valve migration or dislodgment, and 2 patients (10%) had died.
Discussion
While surgery remains the gold standard for the treatment of severe aortic regurgitation, percutaneous alternatives are desirable for patients deemed at high surgical risk,14 as reflected by the high STS score in our series. Our results demonstrate that in selected patients, transfemoral TAVR with the Acurate neo for the treatment of aortic regurgitation is feasible, safe, and may result in excellent hemodynamic outcomes. Only 1 patient had more than mild residual aortic regurgitation, complication rates were low, and a significant reduction in left ventricular end-diastolic diameter (a decrease by 5 mm) was observed prior to discharge.
In this small series, 3 patients (15%) required implantation of a permanent pacemaker. While numbers are too low to allow a valid comparison, the reason for the higher pacemaker rate may be the absence of calcification at the valvular and annular level, resulting in more radial force applied to the subvalvular left ventricular septum and its underlying conduction system.
Patient selection and procedural considerations. During a quite long observation period, only 20 patients were included in this registry. The low patient numbers might be explained by the following factors. First, aortic regurgitation is not as frequent as aortic stenosis, and such patients are often younger and have a lower risk for open-heart surgery.15,16 Second, some patients may have concomitant dilation of the ascending aorta mandating open surgical treatment.3,17 Third, TAVR in patients with native-valve aortic regurgitation still represents an off-label indication. Fourth, not every patient with aortic regurgitation has a suitable anatomy, as such patients often have large annuli and sinuses. In the present study, the mean perimeter-derived annular diameter was 24 ± 2 mm, the long-axis diameter was 26 ± 2 mm, and the short-axis diameter was 21 ± 2 mm. This certainly represents a selected patient population. Indeed, there is currently no valve available that allows percutaneous treatment of annuli that are larger than 30 mm. The average degree of oversizing was 9 ± 4% (about 2 mm), which was more than in the SAVI-TF 1000 registry (5%; Möllmann et al, presented at EuroPCR 2016). This amount of over-sizing appears to provide a good safety margin for the treatment of patients without calcification with the Acurate neo, but should probably be higher with other valves.5
One patient with a low initial position of the Acurate neo required implantation of a second THV, suggesting that the target initial position of the prosthesis should be slightly higher than in patients with severe aortic stenosis, as the final stable position might be a few millimeters lower than the initial position.10 With the data available, we estimated that a targeted initial position of 5 mm below the annulus (instead of 7 mm, as suggested in patients with aortic stenosis) may be ideal. Furthermore, rapid pacing or semirapid pacing may be used to improve the stability of the valve during its release. On the other hand, a number of cases were successfully performed without rapid pacing, indicating that rapid pacing might not be essential. However, in the absence of calcification, there is always a risk for ventricular migration of the THV after it is released.
Comparison to other transcatheter heart valves. Most of the current THVs have been developed for patients with aortic stenosis and rely on calcification of the native valve annulus to anchor the over-sized THV. Hence, treating aortic regurgitation is a relative contraindication due to the absence of calcium.18 Some valves have been designed with a different anchoring (clasping) mechanism that does not rely on calcification of the native valve (JenaValve [JenaValve Technology, Inc]; Engager [Medtronic, Inc]; and J-Valve [JieCheng Medical Technology Co]), but most of them are currently not available for transfemoral access.4,7,19 Recently, the first successful transfemoral implantation of the JenaValve was described in a patient with pure aortic regurgitation.20
In contrast to other devices, the Acurate neo has an x-shaped design that may help to anchor the valve even in the absence of calcification. The upper crown is 5 mm larger than the nominal THV diameter, serving as a “safety anchor” in case the valve is pushed toward the left ventricle after release (Figure 1). Furthermore, the Acurate neo remains very stable during the release process. This may improve accuracy of positioning and may result in a final THV position closer to the intended position.
Several registries of transfemoral TAVR for the treatment of aortic regurgitation have been published; most of the included patients were treated with the CoreValve.3-6,21 In general, patients were younger, device success was lower, and 30-day mortality was higher compared to TAVR for the treatment of severe aortic stenosis. Even in smaller annuli, the absence of calcification was associated with an increased risk for malpositioning or embolization, resulting in an increased rate of residual aortic regurgitation and/or need for a second THV implant.3
Wendt et al reported 8 patients undergoing transapical TAVR with the self-expanding Acurate TA device for the treatment of aortic regurgitation.18 Outcomes were very good, with no death, stroke, pacemaker implantation, or moderate-severe aortic regurgitation at 30 days post procedure. However, apart from the access route, there are important differences between the two systems. The frame of the transfemoral Acurate neo has a lower radial force than the transapical system.22 Furthermore, leaflet insertion of the Acurate neo is supraannular, compared to the intraannular leaflet insertion of the transapical system. As a consequence, the distribution of radial force during diastole may differ between the two valves.
In a recent review including 237 patients with aortic regurgitation treated with different TAVR devices, implantation of a second valve was required in 7% of patients, conversion to surgical aortic valve replacement was necessary in 2.5%, 30-day mortality rate was 7%, cerebrovascular events occurred in 0%, new permanent pacemakers were required in 11%, and moderate-severe aortic regurgitation was present in 9%.23 Sawaya et al reported outcomes after TAVR with different valves in 78 patients with native aortic valve regurgitation.8 Device success rate was 72%, 30-day mortality rate was 14%, stroke rate was 4%, and moderate or severe aortic regurgitation was present in 13% at 30 days. Recently, Yoon et al reported outcomes in 331 patients, with a device success rate of 74%, a 30-day mortality rate of 11%, and a stroke rate of 4%. In this registry, a total of 5 patients underwent implantation of an Acurate (but not an Acurate neo) THV.24
Study limitations. This is a predominantly retrospective study including a small number of patients. However, all patients treated with the Acurate neo THV for aortic regurgitation at the respective centers were included. There was no clinical event committee adjudication for clinical events and no echocardiographic core laboratory. The reported follow-up period is short and more data are needed before expanding indications to percutaneous treatment of aortic regurgitation with the Acurate neo THV; in particular, data on more patients, echocardiographic follow-up data, and long-term data are required.
Conclusion
In patients with aortic regurgitation and suitable anatomy, transfemoral TAVR with the Acurate neo THV was safe and successful in treating aortic regurgitation, significantly reduced left ventricular dimensions, and improved clinical symptoms.
References
1. Siontis GC, Praz F, Pilgrim T, et al. Transcatheter aortic valve implantation vs surgical aortic valve replacement for treatment of severe aortic stenosis: a meta-analysis of randomized trials. Eur Heart J. 2016;37:3503-3512. Epub 2016 Jul 7.
2. Reardon MJ, Van Mieghem NM, Popma JJ, et al. Surgical or transcatheter aortic-valve replacement in intermediate-risk patients. N Engl J Med. 2017;376:1321-1331.
3. Roy DA, Schaefer U, Guetta V, et al. Transcatheter aortic valve implantation for pure severe native aortic valve regurgitation. J Am Coll Cardiol. 2013;61:1577-1584.
4. Schlingloff F, Schafer U, Frerker C, Schmoeckel M, Bader R. Transcatheter aortic valve implantation of a second-generation valve for pure aortic regurgitation: procedural outcome, haemodynamic data and follow-up. Interact Cardiovasc Thorac Surg. 2014;19:388-393.
5. Testa L, Latib A, Rossi ML, et al. CoreValve implantation for severe aortic regurgitation: a multicentre registry. EuroIntervention. 2014;10:739-745.
6. Schofer J, Nietlispach F, Bijuklic K, et al. Transfemoral implantation of a fully repositionable and retrievable transcatheter valve for noncalcified pure aortic regurgitation. JACC Cardiovasc Interv. 2015;8:1842-1849.
7. Wei L, Liu H, Zhu L, et al. A new transcatheter aortic valve replacement system for predominant aortic regurgitation implantation of the J-valve and early outcome. JACC Cardiovasc Interv. 2015;8:1831-1841.
8. Sawaya FJ, Deutsch MA, Seiffert M, et al. Safety and efficacy of transcatheter aortic valve replacement in the treatment of pure aortic regurgitation in native valves and failing surgical bioprostheses: results from an international registry study. JACC Cardiovasc Interv. 2017;10:1048-1056.
9. Schafer U, Conradi L, Diemert P, et al. Symetis Acurate TAVR: review of the technology, developments and current data with this self-expanding transcatheter heart valve. Minerva Cardioangiol. 2015;63:359-369.
10. Toggweiler S, Biaggi P, Grunenfelder J, Reho I, Buhler I, Corti R. First-in-man transfemoral transcatheter aortic valve implantation with the Acurate neo for the treatment of aortic regurgitation. EuroIntervention. 2016;12:78.
11. Cerillo AG, Griese D, Berti S. Successful percutaneous implantation of Symetis Acurate neo transcatheter aortic bioprosthesis for the treatment of pure aortic regurgitation. Catheter Cardiovasc Interv. 2016;88:319-323.
12. Toggweiler S, Nissen H, Mogensen B, et al. Very low pacemaker rate following Acurate neo transcatheter heart valve implantation. EuroIntervention. 2017;13:1273-1280.
13. Kappetein AP, Head SJ, Genereux P, et al. Updated standardized endpoint definitions for transcatheter aortic valve implantation: the Valve Academic Research Consortium-2 consensus document. J Am Coll Cardiol. 2012;60:1438-1454.
14. Webb JG, Htun N. Transcatheter options for the treatment of noncalcified aortic regurgitation. JACC Cardiovasc Interv. 2015;8:1850-1853.
15. Dujardin KS, Enriquez-Sarano M, Schaff HV, Bailey KR, Seward JB, Tajik AJ. Mortality and morbidity of aortic regurgitation in clinical practice. A long-term follow-up study. Circulation. 1999;99:1851-1857.
16. Iung B, Baron G, Butchart EG, et al. A prospective survey of patients with valvular heart disease in Europe: the Euro Heart Survey on Valvular Heart Disease. Eur Heart J. 2003;24:1231-1243.
17. Vahanian A, Alfieri O, Andreotti F, et al. Guidelines on the management of valvular heart disease (version 2012). Eur Heart J. 2012;33:2451-2496.
18. Wendt D, Kahlert P, Pasa S, et al. Transapical transcatheter aortic valve for severe aortic regurgitation: expanding the limits. JACC Cardiovasc Interv. 2014;7:1159-1167.
19. Zhu D, Wei L, Cheung A, et al. Treatment of pure aortic regurgitation using a second-generation transcatheter aortic valve implantation system. J Am Coll Cardiol. 2016;67:2803-2805.
20. Schafer U, Schirmer J, Niklas S, Harmel E, Deuschl F, Conradi L. First-in-human implantation of a novel transfemoral self-expanding transcatheter heart valve to treat pure aortic regurgitation. EuroIntervention. 2017;13:1296-1299.
21. Seiffert M, Bader R, Kappert U, et al. Initial German experience with transapical implantation of a second-generation transcatheter heart valve for the treatment of aortic regurgitation. JACC Cardiovasc Interv. 2014;7:1168-1174.
22. Hamm K, Reents W, Zacher M, et al. Transcatheter aortic valve implantation using the Acurate TA and Acurate neo valves: a four-year single-centre experience. EuroIntervention. 2017;13:53-59.
23. Franzone A, Piccolo R, Siontis GC, et al. Transcatheter aortic valve replacement for the treatment of pure native aortic valve regurgitation: a systematic review. JACC Cardiovasc Interv. 2016;9:2308-2317.
24. Yoon SH, Schmidt T, Bleiziffer S, et al. Transcatheter aortic valve replacement in pure native aortic valve regurgitation. J Am Coll Cardiol. 2017;70:2752-2763.
From the 1Heart Center Lucerne, Luzerner Kantonsspital, Lucerne, Switzerland; 2Interventional Cardiology Unit, G. Pasquinucci Hospital, Massa, Italy; 3Department of Cardiology, Kerckhoff Heart Center, Bad Nauheim, Germany; 4Heart Clinic Hirslanden, Zürich, Switzerland; 5Southwest Cardiothoracic Centre, Derriford Hospital, Plymouth, United Kingdom; 6Klinik and Poliklinik für Innere Medizin II, University of Regensburg Medical Center, Regensburg, Germany; 7Department of Cardiology, Shaare Zedek Medical Center, Jerusalem, Israel; 8Department of Cardiology, University Hospital of Lausanne, Switzerland; and 9Karolinska University Hospital, Stockholm, Sweden.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Toggweiler reports proctor/consultant income from Boston Scientific and NVT; honoraria from Boston Scientific, NVT, Edwards Lifesciences, and Medtronic. Dr Cerillo reports proctor income from Boston Scientific. Dr Kim reports proctor income from Boston Scientific and St. Jude Medical. The remaining authors report no conflicts of interest regarding the content herein.
Manuscript submitted April 22, 2018 and accepted May 2, 2018.
Address for correspondence: Stefan Toggweiler, MD, Heart Center Lucerne, Cardiology, Spitalstrasse, 6000 Luzern, Switzerland. Email: stefan.toggweiler@luks.ch













