 Histoplasmosis is a deep mycotic disease caused by the dimorphic saprophytic fungus Histoplasma capsulatum.1 Two strains, H. capsulatum var. capsulatum and var. duboisii, are considered variants of the same species, but are clinically recognized as distinct pathological entities, termed Classic histoplasmosis and African histoplasmosis, respectively. See Table 1.
Histoplasmosis is a deep mycotic disease caused by the dimorphic saprophytic fungus Histoplasma capsulatum.1 Two strains, H. capsulatum var. capsulatum and var. duboisii, are considered variants of the same species, but are clinically recognized as distinct pathological entities, termed Classic histoplasmosis and African histoplasmosis, respectively. See Table 1.
This review will focus on the classic form, also known as small-form histoplasmosis. Like other deep mycotic infections, it may occur in variants of the three forms: primary cutaneous, primary pulmonary and disseminated histoplasmosis (DH). Rarely, primary cutaneous disease results from direct inoculation with contaminated material, while inhalation of spores more commonly cause a primary pulmonary infection that may progress to disseminated disease in susceptible individuals. Most infected patients remain asymptomatic; however, severe and disseminated disease is commonly seen in immunocompromised populations and warrants prompt diagnosis and treatment to prevent debilitating and fatal disease.
Epidemiology
H. capsulatum is an environmental saprophyte isolated from soil contaminated with bat or bird excreta, such as is found in caves and bird roosts and barns. It is seen worldwide, with an estimated 200,000 new cases diagnosed annually in the United States.2 In the United States, the largest endemic concentration is in the central eastern states, specifically the Ohio and Mississippi river valleys, where 80% to 90% of residents are asymptomatically infected and have positive skin tests for histoplasmin.2-5
The organism enters the body via inhalation of spores and grows within cells of the reticuloendothelial system.1 It can cause epidemics of respiratory infections in healthy persons exposed to spore-laden environments during activities such as exploring caves or cleaning bird barns. Disseminated disease was a very rare occurrence prior to the HIV epidemic, with an incidence of around one disseminated case in 50,000 infections.2 Currently, the AIDS-related incidence of DH is 0.5% to 2.7% in non-endemic areas and can reach up to 10% in endemic areas.6 In addition to HIV, DH is seen in patients with other predisposing conditions affecting the cellular immune system, like lymphoma and transplant recipients.3,6-7 With the advent of biologics like infliximab and other immunosuppressive medications, reactivation of latent pulmonary histoplasmosis has been reported and must be considered when patients develop symptoms in such clinical settings.2,8
Clinical Presentation

 A wide variety of cutaneous manifestations are seen in histoplasmosis, including reactive immune reactions to the primary infection, lesions caused by infectious spread to the skin in disseminated disease, or primary lesions from direct inoculation. See Tables 2 and 3. Symptoms range from asymptomatic and subclinical disease occurring in normal healthy hosts, to severe and fulminating variants seen more commonly in the elderly and immunocompromised.9
A wide variety of cutaneous manifestations are seen in histoplasmosis, including reactive immune reactions to the primary infection, lesions caused by infectious spread to the skin in disseminated disease, or primary lesions from direct inoculation. See Tables 2 and 3. Symptoms range from asymptomatic and subclinical disease occurring in normal healthy hosts, to severe and fulminating variants seen more commonly in the elderly and immunocompromised.9
In 1985, disseminated histoplasmosis was added to the list of opportunistic diseases associated with AIDS.10 Moreover, it is important to keep in mind that AIDS-related cases may initially present as DH with various cutaneous lesions. Cutaneous lesions in disseminated infection have been reported in 6% to 25% of AIDS patients, and are also seen in patients without AIDS.2,7 See Table 3. A common presentation in AIDS patients is a maculopapoular eruption involving the face, trunk and extremities, with ulceration observed in more advanced lesions.7 Compared to cutaneous lesions, mucosal lesions are more commonly seen in DH, occurring in up to half of all cases (30% to 60%).2,11 These lesions may initially present as painless papular swellings that progress to persistent, large, irregular ulcerations and may involve the nasal, gastrointestinal, genital, or, more commonly, oral mucosae (Figures 1 and 2, below).4,11

 Figure 1 (right): Large papular oral lesion of the dorsum tongue showing white discoloration with surrounding erythema, seen in disseminated histoplasmosis.
Figure 1 (right): Large papular oral lesion of the dorsum tongue showing white discoloration with surrounding erythema, seen in disseminated histoplasmosis.
Figure 2 (left): Ulcerative genital lesions involving the vulva and penis showing necrosis and heaped-up margins, seen in disseminated histoplasmosis.
Source: Graham Library of Digital Images, Wake Forest University Department of Dermatology
© 2009 Wake Forest University Dermatology
Histopathology

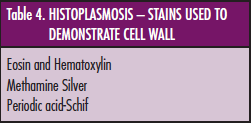
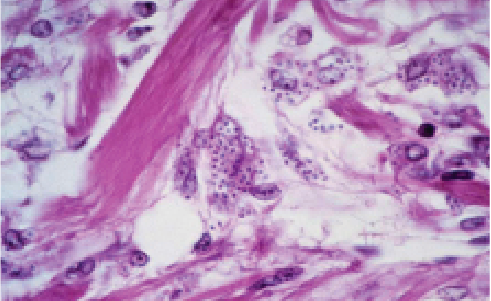
 H. capsulatum var. capsulatum is a small yeast that is 2 µm to 4 µm in diameter. In contrast to its name, it lacks a true capsule and has a ‘pseudocapsule’ with a cell wall that stains strongly with methenamine silver and other stains.1-4 See Table 4. It is an intracellular parasite and is generally found within the cytoplasm of histiocytes, with a halo-like clear space separating the fungal cell wall from the macrophage cytoplasm (Figure 3). The yeast form is found in tissues and the spores divide with narrow-based, unequal budding.2,4
H. capsulatum var. capsulatum is a small yeast that is 2 µm to 4 µm in diameter. In contrast to its name, it lacks a true capsule and has a ‘pseudocapsule’ with a cell wall that stains strongly with methenamine silver and other stains.1-4 See Table 4. It is an intracellular parasite and is generally found within the cytoplasm of histiocytes, with a halo-like clear space separating the fungal cell wall from the macrophage cytoplasm (Figure 3). The yeast form is found in tissues and the spores divide with narrow-based, unequal budding.2,4
Histological sections of primary cutaneous and disseminated cutaneous lesions generally reveal a mixed lymphohistiocytic dermal infiltrate with parasitized histiocytes that can usually be seen with eosin and hematoxylin stains. The extent of inflammation in disseminated disease is variable, depending on the clinical presentation, but usually consists of a granulomatous infiltrate, often with leukocytoclastic vasculitis with variable foci of necrosis.2,4 This infiltrate may extend to the subcutaneous tissue in lesions of Histoplasma panniculitis.
Differential Diagnosis
The cutaneous lesions seen in histoplasmosis are generally non-specific, with no pathognomonic features. Due to the variable morphology, the differential diagnosis is broad. The maculopapular eruption must be distinguished from other diffuse cutaneous phenomena seen in AIDS patients, including bacterial and pityrosporum folliculitis, miliaria and other opportunistic infections.
Histologically, H. capsulatum must be differentiated from other deep mycotic parasites, including P. marneffei and small forms of Blastomyces and Cryptococcus. Other diseases caused by intracellular organisms must be included in the differential, such as leishmaniasis, Chagas’ disease, rhinoscleroma and granuloma inguinale.1,4,12 The infectious pathogens in these diseases do not stain with PAS, which can be helpful when deciphering and establishing the diagnosis of histoplasmosis.
Diagnostic Tests
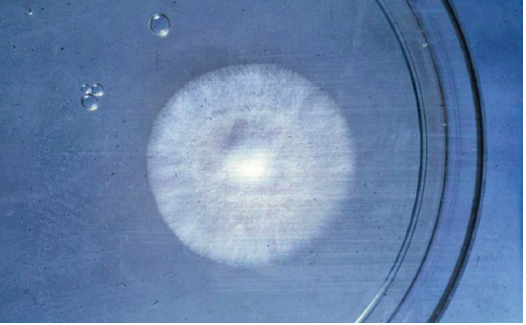
Biopsy of suspicious skin lesions revealing abundant intracellular spores is a benchmark diagnostic tool in establishing the diagnosis of histoplasmosis.1-3 Identification of the organism may be confirmed with a fungal culture. It grows as white, cottony colonies at room temperature on Sabouraud’s glucose agar over several weeks (Figure 4, below, left).2,3 The mycelial phase (Figure 5, below, right) of the growth cycle is highly infectious and laboratories should be warned of the suspected diagnosis.13

 Figure 4 (left): Cottony, white colony of H. capsulatum var. capsulatum.
Figure 4 (left): Cottony, white colony of H. capsulatum var. capsulatum.
Figure 5 (right): The mycelial phase of H. capsulatum var. capsulatum with associated macro and microconidia.
Source: Graham Library of Digital Images, Wake Forest University Department of Dermatology
© 2009 Wake Forest University Dermatology
The intradermal histoplasmin skin test serves no role in diagnosis, but is used as an important tool in epidemiological analyses. An immunodiffusion assay can be used to demonstrate diffusing exoantigens and other precipitants, as the presence of antibodies to specific H and M antigens correlates with active or recent infection.3,4 Newly developed serological tests for circulating Histoplasma antigens are helpful adjunctive diagnostic tests in AIDS patients.3
Treatment
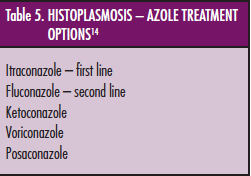
 Asymptomatic latent disease is commonly encountered and does not require treatment in healthy immunocompetent individuals. Since their introduction in the 1990s, systemic azole anti-mycotics are the treatment of choice and various therapeutic options are used depending on the clinical severity of the illness.14 See Table 5. Oral itraconazole, 200 mg to 400 mg daily, is a highly effective option for patients with unresolving acute illness and disseminated disease and is currently the first-line treatment with a target serum concentration of >=2 µg/mL.2-4,14
Asymptomatic latent disease is commonly encountered and does not require treatment in healthy immunocompetent individuals. Since their introduction in the 1990s, systemic azole anti-mycotics are the treatment of choice and various therapeutic options are used depending on the clinical severity of the illness.14 See Table 5. Oral itraconazole, 200 mg to 400 mg daily, is a highly effective option for patients with unresolving acute illness and disseminated disease and is currently the first-line treatment with a target serum concentration of >=2 µg/mL.2-4,14
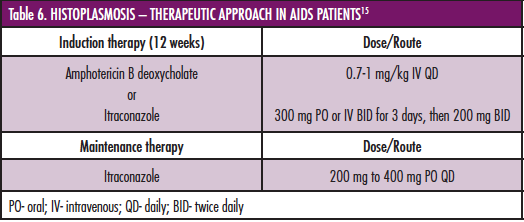
 Historically, intravenous amphotericin B was the only available option for treatment and is currently an effective alternative for severe and fulminant cases, with step-down azole treatment after clinical improvement. A similar cohort of medications is used in AIDS patients and involves a two-step therapeutic approach: induction and maintenance.6,7,15 See Table 6. Maintenance therapy may be discontinued after 12 months in patients who respond to highly affective antiretroviral therapy (HAART) and achieve a CD4+ count >=150 cell/µL, whereas patients who remain highly immunocompromised require lifelong maintenance.15
Historically, intravenous amphotericin B was the only available option for treatment and is currently an effective alternative for severe and fulminant cases, with step-down azole treatment after clinical improvement. A similar cohort of medications is used in AIDS patients and involves a two-step therapeutic approach: induction and maintenance.6,7,15 See Table 6. Maintenance therapy may be discontinued after 12 months in patients who respond to highly affective antiretroviral therapy (HAART) and achieve a CD4+ count >=150 cell/µL, whereas patients who remain highly immunocompromised require lifelong maintenance.15
Key Points
• Histoplasmosis is a deep cutaneous mycotic infection caused by the opportunistic dimorphic fungus Histoplasma capsulatum.
• Latent infection is a common occurrence in endemic populations, but cases of severe fulminant disease are seen in patients with a compromised cellular immune system.
• Cutaneous infection is generally part of a systemic process and lesions range from ulcerative mucosal lesions to a diffuse maculopapular eruption.
• Histological examination reveals the yeast form of the organism as numerous intracellular spores in a granulomatous dermal infiltrate and is often associated with leukocytoclastic vasculitis.
• Routine H&E, GME or PAS staining reveals narrow-based, unequal budding yeasts.
• Fungal culture, serology and molecular methods are adjunctive tests that may be used to confirm the diagnosis after visualization of organisms by direct microscopic examination.
• The first-line treatment is oral itraconazole 200 mg to 400 mg daily. Amphotericin B is an effective alternative for initial treatment in severe disseminated disease, after which azole antifungals are used as maintenance therapy.
Ms. Narahari is with the Center for Dermatology Research and the Department of Dermatology at Wake Forest University School of Medicine in Winston-Salem, NC. Dr. Feldman is with the Center for Dermatology Research and the Departments of Dermatology, Pathology and Public Health Sciences at Wake Forest University School of Medicine in Winston-Salem, NC.
Disclosure: The Center for Dermatology Research is supported by an unrestricted educational grant from Galderma Laboratories, L.P.
 Histoplasmosis is a deep mycotic disease caused by the dimorphic saprophytic fungus Histoplasma capsulatum.1 Two strains, H. capsulatum var. capsulatum and var. duboisii, are considered variants of the same species, but are clinically recognized as distinct pathological entities, termed Classic histoplasmosis and African histoplasmosis, respectively. See Table 1.
Histoplasmosis is a deep mycotic disease caused by the dimorphic saprophytic fungus Histoplasma capsulatum.1 Two strains, H. capsulatum var. capsulatum and var. duboisii, are considered variants of the same species, but are clinically recognized as distinct pathological entities, termed Classic histoplasmosis and African histoplasmosis, respectively. See Table 1.
This review will focus on the classic form, also known as small-form histoplasmosis. Like other deep mycotic infections, it may occur in variants of the three forms: primary cutaneous, primary pulmonary and disseminated histoplasmosis (DH). Rarely, primary cutaneous disease results from direct inoculation with contaminated material, while inhalation of spores more commonly cause a primary pulmonary infection that may progress to disseminated disease in susceptible individuals. Most infected patients remain asymptomatic; however, severe and disseminated disease is commonly seen in immunocompromised populations and warrants prompt diagnosis and treatment to prevent debilitating and fatal disease.
Epidemiology
H. capsulatum is an environmental saprophyte isolated from soil contaminated with bat or bird excreta, such as is found in caves and bird roosts and barns. It is seen worldwide, with an estimated 200,000 new cases diagnosed annually in the United States.2 In the United States, the largest endemic concentration is in the central eastern states, specifically the Ohio and Mississippi river valleys, where 80% to 90% of residents are asymptomatically infected and have positive skin tests for histoplasmin.2-5
The organism enters the body via inhalation of spores and grows within cells of the reticuloendothelial system.1 It can cause epidemics of respiratory infections in healthy persons exposed to spore-laden environments during activities such as exploring caves or cleaning bird barns. Disseminated disease was a very rare occurrence prior to the HIV epidemic, with an incidence of around one disseminated case in 50,000 infections.2 Currently, the AIDS-related incidence of DH is 0.5% to 2.7% in non-endemic areas and can reach up to 10% in endemic areas.6 In addition to HIV, DH is seen in patients with other predisposing conditions affecting the cellular immune system, like lymphoma and transplant recipients.3,6-7 With the advent of biologics like infliximab and other immunosuppressive medications, reactivation of latent pulmonary histoplasmosis has been reported and must be considered when patients develop symptoms in such clinical settings.2,8
Clinical Presentation

 A wide variety of cutaneous manifestations are seen in histoplasmosis, including reactive immune reactions to the primary infection, lesions caused by infectious spread to the skin in disseminated disease, or primary lesions from direct inoculation. See Tables 2 and 3. Symptoms range from asymptomatic and subclinical disease occurring in normal healthy hosts, to severe and fulminating variants seen more commonly in the elderly and immunocompromised.9
A wide variety of cutaneous manifestations are seen in histoplasmosis, including reactive immune reactions to the primary infection, lesions caused by infectious spread to the skin in disseminated disease, or primary lesions from direct inoculation. See Tables 2 and 3. Symptoms range from asymptomatic and subclinical disease occurring in normal healthy hosts, to severe and fulminating variants seen more commonly in the elderly and immunocompromised.9
In 1985, disseminated histoplasmosis was added to the list of opportunistic diseases associated with AIDS.10 Moreover, it is important to keep in mind that AIDS-related cases may initially present as DH with various cutaneous lesions. Cutaneous lesions in disseminated infection have been reported in 6% to 25% of AIDS patients, and are also seen in patients without AIDS.2,7 See Table 3. A common presentation in AIDS patients is a maculopapoular eruption involving the face, trunk and extremities, with ulceration observed in more advanced lesions.7 Compared to cutaneous lesions, mucosal lesions are more commonly seen in DH, occurring in up to half of all cases (30% to 60%).2,11 These lesions may initially present as painless papular swellings that progress to persistent, large, irregular ulcerations and may involve the nasal, gastrointestinal, genital, or, more commonly, oral mucosae (Figures 1 and 2, below).4,11

 Figure 1 (right): Large papular oral lesion of the dorsum tongue showing white discoloration with surrounding erythema, seen in disseminated histoplasmosis.
Figure 1 (right): Large papular oral lesion of the dorsum tongue showing white discoloration with surrounding erythema, seen in disseminated histoplasmosis.
Figure 2 (left): Ulcerative genital lesions involving the vulva and penis showing necrosis and heaped-up margins, seen in disseminated histoplasmosis.
Source: Graham Library of Digital Images, Wake Forest University Department of Dermatology
© 2009 Wake Forest University Dermatology
Histopathology

 H. capsulatum var. capsulatum is a small yeast that is 2 µm to 4 µm in diameter. In contrast to its name, it lacks a true capsule and has a ‘pseudocapsule’ with a cell wall that stains strongly with methenamine silver and other stains.1-4 See Table 4. It is an intracellular parasite and is generally found within the cytoplasm of histiocytes, with a halo-like clear space separating the fungal cell wall from the macrophage cytoplasm (Figure 3). The yeast form is found in tissues and the spores divide with narrow-based, unequal budding.2,4
H. capsulatum var. capsulatum is a small yeast that is 2 µm to 4 µm in diameter. In contrast to its name, it lacks a true capsule and has a ‘pseudocapsule’ with a cell wall that stains strongly with methenamine silver and other stains.1-4 See Table 4. It is an intracellular parasite and is generally found within the cytoplasm of histiocytes, with a halo-like clear space separating the fungal cell wall from the macrophage cytoplasm (Figure 3). The yeast form is found in tissues and the spores divide with narrow-based, unequal budding.2,4
Histological sections of primary cutaneous and disseminated cutaneous lesions generally reveal a mixed lymphohistiocytic dermal infiltrate with parasitized histiocytes that can usually be seen with eosin and hematoxylin stains. The extent of inflammation in disseminated disease is variable, depending on the clinical presentation, but usually consists of a granulomatous infiltrate, often with leukocytoclastic vasculitis with variable foci of necrosis.2,4 This infiltrate may extend to the subcutaneous tissue in lesions of Histoplasma panniculitis.
Differential Diagnosis
The cutaneous lesions seen in histoplasmosis are generally non-specific, with no pathognomonic features. Due to the variable morphology, the differential diagnosis is broad. The maculopapular eruption must be distinguished from other diffuse cutaneous phenomena seen in AIDS patients, including bacterial and pityrosporum folliculitis, miliaria and other opportunistic infections.
Histologically, H. capsulatum must be differentiated from other deep mycotic parasites, including P. marneffei and small forms of Blastomyces and Cryptococcus. Other diseases caused by intracellular organisms must be included in the differential, such as leishmaniasis, Chagas’ disease, rhinoscleroma and granuloma inguinale.1,4,12 The infectious pathogens in these diseases do not stain with PAS, which can be helpful when deciphering and establishing the diagnosis of histoplasmosis.
Diagnostic Tests
Biopsy of suspicious skin lesions revealing abundant intracellular spores is a benchmark diagnostic tool in establishing the diagnosis of histoplasmosis.1-3 Identification of the organism may be confirmed with a fungal culture. It grows as white, cottony colonies at room temperature on Sabouraud’s glucose agar over several weeks (Figure 4, below, left).2,3 The mycelial phase (Figure 5, below, right) of the growth cycle is highly infectious and laboratories should be warned of the suspected diagnosis.13

 Figure 4 (left): Cottony, white colony of H. capsulatum var. capsulatum.
Figure 4 (left): Cottony, white colony of H. capsulatum var. capsulatum.
Figure 5 (right): The mycelial phase of H. capsulatum var. capsulatum with associated macro and microconidia.
Source: Graham Library of Digital Images, Wake Forest University Department of Dermatology
© 2009 Wake Forest University Dermatology
The intradermal histoplasmin skin test serves no role in diagnosis, but is used as an important tool in epidemiological analyses. An immunodiffusion assay can be used to demonstrate diffusing exoantigens and other precipitants, as the presence of antibodies to specific H and M antigens correlates with active or recent infection.3,4 Newly developed serological tests for circulating Histoplasma antigens are helpful adjunctive diagnostic tests in AIDS patients.3
Treatment
 Asymptomatic latent disease is commonly encountered and does not require treatment in healthy immunocompetent individuals. Since their introduction in the 1990s, systemic azole anti-mycotics are the treatment of choice and various therapeutic options are used depending on the clinical severity of the illness.14 See Table 5. Oral itraconazole, 200 mg to 400 mg daily, is a highly effective option for patients with unresolving acute illness and disseminated disease and is currently the first-line treatment with a target serum concentration of >=2 µg/mL.2-4,14
Asymptomatic latent disease is commonly encountered and does not require treatment in healthy immunocompetent individuals. Since their introduction in the 1990s, systemic azole anti-mycotics are the treatment of choice and various therapeutic options are used depending on the clinical severity of the illness.14 See Table 5. Oral itraconazole, 200 mg to 400 mg daily, is a highly effective option for patients with unresolving acute illness and disseminated disease and is currently the first-line treatment with a target serum concentration of >=2 µg/mL.2-4,14
 Historically, intravenous amphotericin B was the only available option for treatment and is currently an effective alternative for severe and fulminant cases, with step-down azole treatment after clinical improvement. A similar cohort of medications is used in AIDS patients and involves a two-step therapeutic approach: induction and maintenance.6,7,15 See Table 6. Maintenance therapy may be discontinued after 12 months in patients who respond to highly affective antiretroviral therapy (HAART) and achieve a CD4+ count >=150 cell/µL, whereas patients who remain highly immunocompromised require lifelong maintenance.15
Historically, intravenous amphotericin B was the only available option for treatment and is currently an effective alternative for severe and fulminant cases, with step-down azole treatment after clinical improvement. A similar cohort of medications is used in AIDS patients and involves a two-step therapeutic approach: induction and maintenance.6,7,15 See Table 6. Maintenance therapy may be discontinued after 12 months in patients who respond to highly affective antiretroviral therapy (HAART) and achieve a CD4+ count >=150 cell/µL, whereas patients who remain highly immunocompromised require lifelong maintenance.15
Key Points
• Histoplasmosis is a deep cutaneous mycotic infection caused by the opportunistic dimorphic fungus Histoplasma capsulatum.
• Latent infection is a common occurrence in endemic populations, but cases of severe fulminant disease are seen in patients with a compromised cellular immune system.
• Cutaneous infection is generally part of a systemic process and lesions range from ulcerative mucosal lesions to a diffuse maculopapular eruption.
• Histological examination reveals the yeast form of the organism as numerous intracellular spores in a granulomatous dermal infiltrate and is often associated with leukocytoclastic vasculitis.
• Routine H&E, GME or PAS staining reveals narrow-based, unequal budding yeasts.
• Fungal culture, serology and molecular methods are adjunctive tests that may be used to confirm the diagnosis after visualization of organisms by direct microscopic examination.
• The first-line treatment is oral itraconazole 200 mg to 400 mg daily. Amphotericin B is an effective alternative for initial treatment in severe disseminated disease, after which azole antifungals are used as maintenance therapy.
Ms. Narahari is with the Center for Dermatology Research and the Department of Dermatology at Wake Forest University School of Medicine in Winston-Salem, NC. Dr. Feldman is with the Center for Dermatology Research and the Departments of Dermatology, Pathology and Public Health Sciences at Wake Forest University School of Medicine in Winston-Salem, NC.
Disclosure: The Center for Dermatology Research is supported by an unrestricted educational grant from Galderma Laboratories, L.P.
Histoplasmosis is a deep mycotic disease caused by the dimorphic saprophytic fungus Histoplasma capsulatum.1 Two strains, H. capsulatum var. capsulatum and var. duboisii, are considered variants of the same species, but are clinically recognized as distinct pathological entities, termed Classic histoplasmosis and African histoplasmosis, respectively. See Table 1.
This review will focus on the classic form, also known as small-form histoplasmosis. Like other deep mycotic infections, it may occur in variants of the three forms: primary cutaneous, primary pulmonary and disseminated histoplasmosis (DH). Rarely, primary cutaneous disease results from direct inoculation with contaminated material, while inhalation of spores more commonly cause a primary pulmonary infection that may progress to disseminated disease in susceptible individuals. Most infected patients remain asymptomatic; however, severe and disseminated disease is commonly seen in immunocompromised populations and warrants prompt diagnosis and treatment to prevent debilitating and fatal disease.
Epidemiology
H. capsulatum is an environmental saprophyte isolated from soil contaminated with bat or bird excreta, such as is found in caves and bird roosts and barns. It is seen worldwide, with an estimated 200,000 new cases diagnosed annually in the United States.2 In the United States, the largest endemic concentration is in the central eastern states, specifically the Ohio and Mississippi river valleys, where 80% to 90% of residents are asymptomatically infected and have positive skin tests for histoplasmin.2-5
The organism enters the body via inhalation of spores and grows within cells of the reticuloendothelial system.1 It can cause epidemics of respiratory infections in healthy persons exposed to spore-laden environments during activities such as exploring caves or cleaning bird barns. Disseminated disease was a very rare occurrence prior to the HIV epidemic, with an incidence of around one disseminated case in 50,000 infections.2 Currently, the AIDS-related incidence of DH is 0.5% to 2.7% in non-endemic areas and can reach up to 10% in endemic areas.6 In addition to HIV, DH is seen in patients with other predisposing conditions affecting the cellular immune system, like lymphoma and transplant recipients.3,6-7 With the advent of biologics like infliximab and other immunosuppressive medications, reactivation of latent pulmonary histoplasmosis has been reported and must be considered when patients develop symptoms in such clinical settings.2,8
Clinical Presentation
A wide variety of cutaneous manifestations are seen in histoplasmosis, including reactive immune reactions to the primary infection, lesions caused by infectious spread to the skin in disseminated disease, or primary lesions from direct inoculation. See Tables 2 and 3. Symptoms range from asymptomatic and subclinical disease occurring in normal healthy hosts, to severe and fulminating variants seen more commonly in the elderly and immunocompromised.9
In 1985, disseminated histoplasmosis was added to the list of opportunistic diseases associated with AIDS.10 Moreover, it is important to keep in mind that AIDS-related cases may initially present as DH with various cutaneous lesions. Cutaneous lesions in disseminated infection have been reported in 6% to 25% of AIDS patients, and are also seen in patients without AIDS.2,7 See Table 3. A common presentation in AIDS patients is a maculopapoular eruption involving the face, trunk and extremities, with ulceration observed in more advanced lesions.7 Compared to cutaneous lesions, mucosal lesions are more commonly seen in DH, occurring in up to half of all cases (30% to 60%).2,11 These lesions may initially present as painless papular swellings that progress to persistent, large, irregular ulcerations and may involve the nasal, gastrointestinal, genital, or, more commonly, oral mucosae (Figures 1 and 2, below).4,11
Figure 1 (right): Large papular oral lesion of the dorsum tongue showing white discoloration with surrounding erythema, seen in disseminated histoplasmosis.
Figure 2 (left): Ulcerative genital lesions involving the vulva and penis showing necrosis and heaped-up margins, seen in disseminated histoplasmosis.
Source: Graham Library of Digital Images, Wake Forest University Department of Dermatology
© 2009 Wake Forest University Dermatology
Histopathology
H. capsulatum var. capsulatum is a small yeast that is 2 µm to 4 µm in diameter. In contrast to its name, it lacks a true capsule and has a ‘pseudocapsule’ with a cell wall that stains strongly with methenamine silver and other stains.1-4 See Table 4. It is an intracellular parasite and is generally found within the cytoplasm of histiocytes, with a halo-like clear space separating the fungal cell wall from the macrophage cytoplasm (Figure 3). The yeast form is found in tissues and the spores divide with narrow-based, unequal budding.2,4
Histological sections of primary cutaneous and disseminated cutaneous lesions generally reveal a mixed lymphohistiocytic dermal infiltrate with parasitized histiocytes that can usually be seen with eosin and hematoxylin stains. The extent of inflammation in disseminated disease is variable, depending on the clinical presentation, but usually consists of a granulomatous infiltrate, often with leukocytoclastic vasculitis with variable foci of necrosis.2,4 This infiltrate may extend to the subcutaneous tissue in lesions of Histoplasma panniculitis.
Differential Diagnosis
The cutaneous lesions seen in histoplasmosis are generally non-specific, with no pathognomonic features. Due to the variable morphology, the differential diagnosis is broad. The maculopapular eruption must be distinguished from other diffuse cutaneous phenomena seen in AIDS patients, including bacterial and pityrosporum folliculitis, miliaria and other opportunistic infections.
Histologically, H. capsulatum must be differentiated from other deep mycotic parasites, including P. marneffei and small forms of Blastomyces and Cryptococcus. Other diseases caused by intracellular organisms must be included in the differential, such as leishmaniasis, Chagas’ disease, rhinoscleroma and granuloma inguinale.1,4,12 The infectious pathogens in these diseases do not stain with PAS, which can be helpful when deciphering and establishing the diagnosis of histoplasmosis.
Diagnostic Tests
Biopsy of suspicious skin lesions revealing abundant intracellular spores is a benchmark diagnostic tool in establishing the diagnosis of histoplasmosis.1-3 Identification of the organism may be confirmed with a fungal culture. It grows as white, cottony colonies at room temperature on Sabouraud’s glucose agar over several weeks (Figure 4, below, left).2,3 The mycelial phase (Figure 5, below, right) of the growth cycle is highly infectious and laboratories should be warned of the suspected diagnosis.13
Figure 4 (left): Cottony, white colony of H. capsulatum var. capsulatum.
Figure 5 (right): The mycelial phase of H. capsulatum var. capsulatum with associated macro and microconidia.
Source: Graham Library of Digital Images, Wake Forest University Department of Dermatology
© 2009 Wake Forest University Dermatology
The intradermal histoplasmin skin test serves no role in diagnosis, but is used as an important tool in epidemiological analyses. An immunodiffusion assay can be used to demonstrate diffusing exoantigens and other precipitants, as the presence of antibodies to specific H and M antigens correlates with active or recent infection.3,4 Newly developed serological tests for circulating Histoplasma antigens are helpful adjunctive diagnostic tests in AIDS patients.3
Treatment
Asymptomatic latent disease is commonly encountered and does not require treatment in healthy immunocompetent individuals. Since their introduction in the 1990s, systemic azole anti-mycotics are the treatment of choice and various therapeutic options are used depending on the clinical severity of the illness.14 See Table 5. Oral itraconazole, 200 mg to 400 mg daily, is a highly effective option for patients with unresolving acute illness and disseminated disease and is currently the first-line treatment with a target serum concentration of >=2 µg/mL.2-4,14
Historically, intravenous amphotericin B was the only available option for treatment and is currently an effective alternative for severe and fulminant cases, with step-down azole treatment after clinical improvement. A similar cohort of medications is used in AIDS patients and involves a two-step therapeutic approach: induction and maintenance.6,7,15 See Table 6. Maintenance therapy may be discontinued after 12 months in patients who respond to highly affective antiretroviral therapy (HAART) and achieve a CD4+ count >=150 cell/µL, whereas patients who remain highly immunocompromised require lifelong maintenance.15
Key Points
• Histoplasmosis is a deep cutaneous mycotic infection caused by the opportunistic dimorphic fungus Histoplasma capsulatum.
• Latent infection is a common occurrence in endemic populations, but cases of severe fulminant disease are seen in patients with a compromised cellular immune system.
• Cutaneous infection is generally part of a systemic process and lesions range from ulcerative mucosal lesions to a diffuse maculopapular eruption.
• Histological examination reveals the yeast form of the organism as numerous intracellular spores in a granulomatous dermal infiltrate and is often associated with leukocytoclastic vasculitis.
• Routine H&E, GME or PAS staining reveals narrow-based, unequal budding yeasts.
• Fungal culture, serology and molecular methods are adjunctive tests that may be used to confirm the diagnosis after visualization of organisms by direct microscopic examination.
• The first-line treatment is oral itraconazole 200 mg to 400 mg daily. Amphotericin B is an effective alternative for initial treatment in severe disseminated disease, after which azole antifungals are used as maintenance therapy.
Ms. Narahari is with the Center for Dermatology Research and the Department of Dermatology at Wake Forest University School of Medicine in Winston-Salem, NC. Dr. Feldman is with the Center for Dermatology Research and the Departments of Dermatology, Pathology and Public Health Sciences at Wake Forest University School of Medicine in Winston-Salem, NC.
Disclosure: The Center for Dermatology Research is supported by an unrestricted educational grant from Galderma Laboratories, L.P.









 Histoplasmosis is a deep mycotic disease caused by the dimorphic saprophytic fungus Histoplasma capsulatum.1 Two strains, H. capsulatum var. capsulatum and var. duboisii, are considered variants of the same species, but are clinically recognized as distinct pathological entities, termed Classic histoplasmosis and African histoplasmosis, respectively. See Table 1.
Histoplasmosis is a deep mycotic disease caused by the dimorphic saprophytic fungus Histoplasma capsulatum.1 Two strains, H. capsulatum var. capsulatum and var. duboisii, are considered variants of the same species, but are clinically recognized as distinct pathological entities, termed Classic histoplasmosis and African histoplasmosis, respectively. See Table 1.
 A wide variety of cutaneous manifestations are seen in histoplasmosis, including reactive immune reactions to the primary infection, lesions caused by infectious spread to the skin in disseminated disease, or primary lesions from direct inoculation. See Tables 2 and 3. Symptoms range from asymptomatic and subclinical disease occurring in normal healthy hosts, to severe and fulminating variants seen more commonly in the elderly and immunocompromised.9
A wide variety of cutaneous manifestations are seen in histoplasmosis, including reactive immune reactions to the primary infection, lesions caused by infectious spread to the skin in disseminated disease, or primary lesions from direct inoculation. See Tables 2 and 3. Symptoms range from asymptomatic and subclinical disease occurring in normal healthy hosts, to severe and fulminating variants seen more commonly in the elderly and immunocompromised.9
 Figure 1 (right): Large papular oral lesion of the dorsum tongue showing white discoloration with surrounding erythema, seen in disseminated histoplasmosis.
Figure 1 (right): Large papular oral lesion of the dorsum tongue showing white discoloration with surrounding erythema, seen in disseminated histoplasmosis.
 H. capsulatum var. capsulatum is a small yeast that is 2 µm to 4 µm in diameter. In contrast to its name, it lacks a true capsule and has a ‘pseudocapsule’ with a cell wall that stains strongly with methenamine silver and other stains.1-4 See Table 4. It is an intracellular parasite and is generally found within the cytoplasm of histiocytes, with a halo-like clear space separating the fungal cell wall from the macrophage cytoplasm (Figure 3). The yeast form is found in tissues and the spores divide with narrow-based, unequal budding.2,4
H. capsulatum var. capsulatum is a small yeast that is 2 µm to 4 µm in diameter. In contrast to its name, it lacks a true capsule and has a ‘pseudocapsule’ with a cell wall that stains strongly with methenamine silver and other stains.1-4 See Table 4. It is an intracellular parasite and is generally found within the cytoplasm of histiocytes, with a halo-like clear space separating the fungal cell wall from the macrophage cytoplasm (Figure 3). The yeast form is found in tissues and the spores divide with narrow-based, unequal budding.2,4
 Figure 4 (left): Cottony, white colony of H. capsulatum var. capsulatum.
Figure 4 (left): Cottony, white colony of H. capsulatum var. capsulatum. Asymptomatic latent disease is commonly encountered and does not require treatment in healthy immunocompetent individuals. Since their introduction in the 1990s, systemic azole anti-mycotics are the treatment of choice and various therapeutic options are used depending on the clinical severity of the illness.14 See Table 5. Oral itraconazole, 200 mg to 400 mg daily, is a highly effective option for patients with unresolving acute illness and disseminated disease and is currently the first-line treatment with a target serum concentration of >=2 µg/mL.2-4,14
Asymptomatic latent disease is commonly encountered and does not require treatment in healthy immunocompetent individuals. Since their introduction in the 1990s, systemic azole anti-mycotics are the treatment of choice and various therapeutic options are used depending on the clinical severity of the illness.14 See Table 5. Oral itraconazole, 200 mg to 400 mg daily, is a highly effective option for patients with unresolving acute illness and disseminated disease and is currently the first-line treatment with a target serum concentration of >=2 µg/mL.2-4,14 Historically, intravenous amphotericin B was the only available option for treatment and is currently an effective alternative for severe and fulminant cases, with step-down azole treatment after clinical improvement. A similar cohort of medications is used in AIDS patients and involves a two-step therapeutic approach: induction and maintenance.6,7,15 See Table 6. Maintenance therapy may be discontinued after 12 months in patients who respond to highly affective antiretroviral therapy (HAART) and achieve a CD4+ count >=150 cell/µL, whereas patients who remain highly immunocompromised require lifelong maintenance.15
Historically, intravenous amphotericin B was the only available option for treatment and is currently an effective alternative for severe and fulminant cases, with step-down azole treatment after clinical improvement. A similar cohort of medications is used in AIDS patients and involves a two-step therapeutic approach: induction and maintenance.6,7,15 See Table 6. Maintenance therapy may be discontinued after 12 months in patients who respond to highly affective antiretroviral therapy (HAART) and achieve a CD4+ count >=150 cell/µL, whereas patients who remain highly immunocompromised require lifelong maintenance.15







