


What Caused This Linear Erythematous Reaction?
PATIENT PRESENTATION

 A 32-year-old Caucasian female presented with a pruritic, burning rash that began while she was on vacation in San Francisco, CA one week earlier. Her husband was not similarly affected. She thought it was related to the hotel where they were staying, but the rash continued to worsen after changing hotels and upon returning home. She went to the emergency room, where she received an injection of epinephrine, IV steroid and famotidine and prescriptions for oral famotidine and prednisone (60 mg for 5 days). Other than long-term fluoxetine for depression, the patient was healthy with no new medication history. On physical examination, there were multiple linear red/purple urticarial streaks in primarily reachable areas of the upper and lower back, abdomen, waistline and breasts. She demonstrated only mild dermatographism with slight erythema but no wheals upon stroking the skin. A punch biopsy was obtained from a lesion on the upper back.
A 32-year-old Caucasian female presented with a pruritic, burning rash that began while she was on vacation in San Francisco, CA one week earlier. Her husband was not similarly affected. She thought it was related to the hotel where they were staying, but the rash continued to worsen after changing hotels and upon returning home. She went to the emergency room, where she received an injection of epinephrine, IV steroid and famotidine and prescriptions for oral famotidine and prednisone (60 mg for 5 days). Other than long-term fluoxetine for depression, the patient was healthy with no new medication history. On physical examination, there were multiple linear red/purple urticarial streaks in primarily reachable areas of the upper and lower back, abdomen, waistline and breasts. She demonstrated only mild dermatographism with slight erythema but no wheals upon stroking the skin. A punch biopsy was obtained from a lesion on the upper back.
WHAT IS YOUR DIAGNOSIS?
DIAGNOSIS: SHIITAKE DERMATITIS
Following only button mushrooms (Agaricus bisporus), shiitake mushrooms are the second most consumed mushrooms worldwide.1-3 However, despite their widespread consumption, the dermatitis associated with ingestion is a rather rare occurrence. The characteristic linear reaction is elicited by the consumption of, and, in rare instances, contact with, the mushroom Lentinus edodes. This popular mushroom is consumed in profound quantities throughout the world, yet the associated dermatitis has been predominately described in Japan with only isolated cases elsewhere.
Clinical Presentation
 There have been roughly 100 case reports involving shiitake dermatitis, each with a rather characteristic pattern of inflammation that principally involves the upper extremities, abdomen and neck.4-6 The dermatitis has a classic pattern of papulovesicles in a linear arrangement in association with severely pruritic, erythematous papules.2-3,5-7 This eczematous reaction typically appears 1-2 days following the consumption of unprepared mushrooms, peaks in 5-8 days and usually resolves in about 2 weeks. An analogous reaction has also been described as a result of physical contact with the mushroom, suggesting the reaction may be due to a type IV hypersensitivity response. Kopp et al described a case of shiitake dermatitis accompanied by fever, conjunctival injection and malaise, which had not been described in previous case reports.6
There have been roughly 100 case reports involving shiitake dermatitis, each with a rather characteristic pattern of inflammation that principally involves the upper extremities, abdomen and neck.4-6 The dermatitis has a classic pattern of papulovesicles in a linear arrangement in association with severely pruritic, erythematous papules.2-3,5-7 This eczematous reaction typically appears 1-2 days following the consumption of unprepared mushrooms, peaks in 5-8 days and usually resolves in about 2 weeks. An analogous reaction has also been described as a result of physical contact with the mushroom, suggesting the reaction may be due to a type IV hypersensitivity response. Kopp et al described a case of shiitake dermatitis accompanied by fever, conjunctival injection and malaise, which had not been described in previous case reports.6
Differential Diagnosis
The main differential diagnosis for shiitake dermatitis is other hypersensitivity reactions, including drug eruptions, dermatographism or other types of urticaria, and contact dermatitis. Drug eruptions have a wide range of presentations. Interestingly, a linear pattern of inflammation and pruritus identical to that of shiitake dermatitis has been described in approximately 20% of patients receiving the chemotherapeutic agent bleomycin.3,8 This finding suggests that lentinan, a polysaccharide of shiitake, may be a catalyst for the systemic reaction seen with shiitake dermatitis, as its antineoplastic and immunomodulating properties are employed as adjuvant therapy with typical chemotherapeutic agents, including bleomycin.8 Dermatographism describes histamine release due to stroking of the skin, causing an exaggerated wheal response. This most often creates one or more linear streaks and may leave a flagellated appearance after a bout of intense scratching. However, patients with shiitake dermatitis do not demonstrate significant dermatographism when eliciting this response is attempted.
Etiology
 Preparation of the mushroom is important in the development of the reaction. Ingestion of or contact with raw or half-cooked mushrooms triggers the reaction, while fully cooked or boiled shiitake do not. Kopp et al described examinations in which prick-to-prick and scratch testing with raw mushrooms incited characteristic inflammation, while similar testing with cooked mushrooms failed to elicit a response.6 This finding has lead to the argument that the causative agent, lentinan, may be a thermolabile constituent of shiitake.5 Some cases have occurred in patients who had significant external physical contact with the mushroom prior to developing the reaction.6 Due to the widespread consumption and low incidence of the associated dermatitis, it has been proposed that a reaction is elicited only in sensitized patients, implicating a type IV hypersensitivity reaction.6 However, Nakamura et al illustrated that skin prick testing with shiitake in consumption cases did not elicit an immune response, leading to the belief that lentinan may induce a toxic, as opposed to allergic, reaction in dermal capillaries.2 While it is apparent that sensitivity and preparation of the mushroom influence the development of the dermatitis to some extent, Hanada et al have suggested that photosensitivity may also play a role.5
Preparation of the mushroom is important in the development of the reaction. Ingestion of or contact with raw or half-cooked mushrooms triggers the reaction, while fully cooked or boiled shiitake do not. Kopp et al described examinations in which prick-to-prick and scratch testing with raw mushrooms incited characteristic inflammation, while similar testing with cooked mushrooms failed to elicit a response.6 This finding has lead to the argument that the causative agent, lentinan, may be a thermolabile constituent of shiitake.5 Some cases have occurred in patients who had significant external physical contact with the mushroom prior to developing the reaction.6 Due to the widespread consumption and low incidence of the associated dermatitis, it has been proposed that a reaction is elicited only in sensitized patients, implicating a type IV hypersensitivity reaction.6 However, Nakamura et al illustrated that skin prick testing with shiitake in consumption cases did not elicit an immune response, leading to the belief that lentinan may induce a toxic, as opposed to allergic, reaction in dermal capillaries.2 While it is apparent that sensitivity and preparation of the mushroom influence the development of the dermatitis to some extent, Hanada et al have suggested that photosensitivity may also play a role.5
Diagnosis
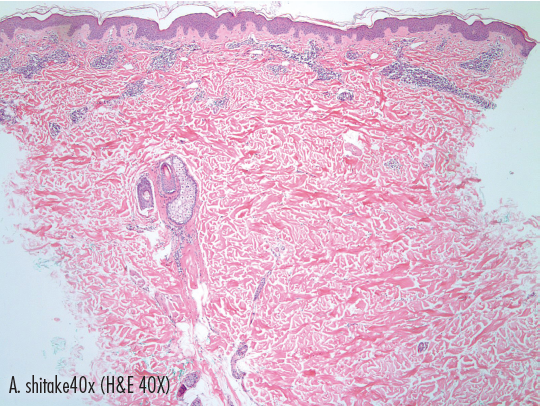
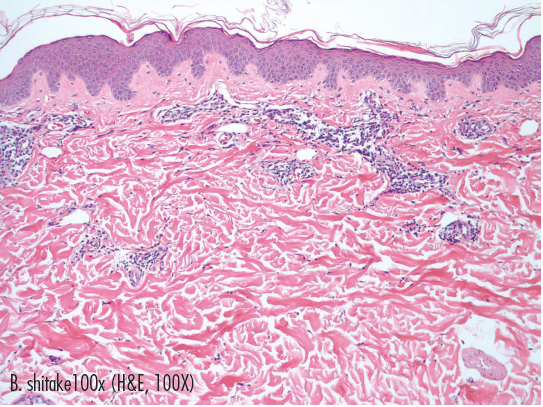 The diagnosis of shiitake dermatitis is supported primarily by its self-limited presentation, which involves the classic linear pattern of papulovesicles that appear 1-2 days after the consumption of raw or half-cooked shiitake. Histological examination illustrates a nonspecific capillary vasodilation leading to dermal edema with lymphocytic and eosinophilic infiltration and variable spongiosis.3,6 Prick-to-prick skin testing yields acceptable results in contact sensitivity cases, although studies by Nakamura et al did not support prick-to-prick testing in cases involving ingestion of shiitake.2
The diagnosis of shiitake dermatitis is supported primarily by its self-limited presentation, which involves the classic linear pattern of papulovesicles that appear 1-2 days after the consumption of raw or half-cooked shiitake. Histological examination illustrates a nonspecific capillary vasodilation leading to dermal edema with lymphocytic and eosinophilic infiltration and variable spongiosis.3,6 Prick-to-prick skin testing yields acceptable results in contact sensitivity cases, although studies by Nakamura et al did not support prick-to-prick testing in cases involving ingestion of shiitake.2
Our Patient
Histology of the upper back biopsy suggested no abnormalities of the epidermis. In the dermis, there was perivascular infiltration, primarily of lymphocytes with some neutrophils and rare eosinophils present as well. The overall picture was consistent with a toxic dermatitis or urticarial reaction. We were aware of the unique flagellate appearance of shiitake and bleomycin dermatitis, and, upon questioning, the patient admitted eating mushrooms while on vacation the day prior to the development of the rash. Our suspicions were confirmed when she had a second occurrence of the reaction 7 months later after eating fried rice from a Chinese restaurant chain. She had been told there were no mushrooms in the rice prior to ordering, but, after the rash recurred, the head chef confirmed the presence of shiitake mushrooms in the fried rice. At the time of the second occurrence, the patient reported a mild sore throat but no dyspnea. She was given prescriptions for a tapering dose of prednisone, 40 mg to 10 mg over 16 days, hydroxyzine 10 mg every 6 hours as needed for itch, and fexofenadine 180 mg daily to use until the rash resolved. An Epipen was also prescribed in case her throat symptoms worsened or any dyspnea developed. An evaluation by an allergist for further testing was recommended. The patient was instructed to be vigilant in her avoidance of shiitake mushrooms, and to date we are unaware of any further episodes.
Michael Dreifke is a fourth-year medical student at the University of Toledo College of Medicine in Toledo, OH.
Nina Rettig is a physician assistant practicing dermatology at Renaissance Dermatology in Toledo, OH.
Mounir Boutros is a board-certified dermatologist at Renaissance Dermatology in Toledo, OH.
David Mehregan is a board-certified dermatologist at Wayne State University in Dearborn, MI and dermatopathologist at Pinkus Dermatopathology Laboratory in Monroe, MI.
Darius Mehregan is a board-certified dermatologist and the Herman Pinkus Chairman at Wayne State University in Dearborn, MI and dermatopathologist at Pinkus Dermatopathology Laboratory in Monroe, MI.
Disclosure: The authors have no conflicts of interest to report.








