


"Measurement Monday": One Facility’s Approach to Standardizing Skin Impairment Documentation
Abstract
Accurate, timely wound assessment and documentation is fundamental to nursing practice. A 2005 retrospective chart audit (N = 54) at a rural, 238-bed tertiary care facility in Northeastern Pennsylvania (average daily census 175 to 180) found that complete wound assessment documentation (including measurements) was lacking in 59% of patient charts. The purpose of this quality improvement initiative, led by the Wound Ostomy Continence Nurse (WOCN), was to evaluate and improve nursing assessment and documentation of impaired skin (pressure ulcers, skin tears, open surgical wounds, diabetic ulcers, and venous stasis ulcers).
A review of the literature confirmed the importance of consistency, which led to the hospital-wide implementation of education programs and “Measurement Monday.” Using AHCPR guidelines of care for pressure ulcers and beginning in January 2006 all wounds were assessed and measured every Monday and the proportion of incomplete charts declined to 38%. Following addition of a wound documentation tool in 2007, the proportion of incomplete records was 14.8%. This quality improvement initiative improved the quality and consistency of wound assessment/measurement and documentation.
Please address correspondence to: Suzanne Stewart, MS, RN, CWOCN, Robert Packer Hospital, Guthrie Healthcare, 1 Guthrie Square, Sayre, PA 18840; email: stewart_suzanne@guthrie.org.
As many as 3 million people suffer from pressure ulcers in the United States; costs can be as high as $3.6 billion.1,2 Consistent, complete, and accurate wound assessment/measurement and documentation of compromised skin integrity, wound size, treatments, and healing progression are an important part of nursing practice.2-5 Accurate and timely wound assessments, including measurements, are needed to help determine the best treatment plan for patients with impaired skin such as pressure ulcers, skin tears, open surgical wounds, diabetic ulcers, and venous stasis ulcers. Measurements, as included in the initial wound assessment of impaired skin, provide baseline data for tracking treatment outcomes.2-7 Evidence in a patient’s record related to accurate and timely assessments, treatments, and documentation support that a patient has received care and may answer questions related to internal quality investigation or possible litigation.7-10 In order to ensure accurate measurement comparison and evaluate healing over time, consistent assessment methods are necessary and reliable observations must be documented.5,7-12
 Routine patient record monitoring at a rural, 238-bed tertiary care facility in Northeastern Pennsylvania revealed a lack of consistency with regard to documentation of the wound assessment/measurement process. The purpose of this quality improvement initiative, led by the Wound Ostomy Continence Nurse (WOCN), was to evaluate and improve nursing assessment and documentation of impaired skin.
Routine patient record monitoring at a rural, 238-bed tertiary care facility in Northeastern Pennsylvania revealed a lack of consistency with regard to documentation of the wound assessment/measurement process. The purpose of this quality improvement initiative, led by the Wound Ostomy Continence Nurse (WOCN), was to evaluate and improve nursing assessment and documentation of impaired skin.
Methods
Literature review. In the initial phase of this quality improvement project, best practices were retrieved from the Agency on Health Care Policy and Research’s (AHCPR, now the Agency for Healthcare Research and Quality, AHRQ)3 and the Wound, Ostomy and Continence Nurses Society’s2 pressure ulcer treatment guidelines. Additional literature was consulted later in the project — a literature review was conducted in October 2007 and then again in August 2008 using PUBMED (United States National Library of Medicine) and the Cumulative Index to Nursing and Allied Health Literature (CINAHL®) and the search terms wounds, documentation, wound tools, and wound assessment. The first review was conducted to look for a mnemonic. When none was found, a second review was conducted to search for other assessment and documentation strategies. Thus, the literature review was conducted to 1) determine if any particular phrases or mnemonics existed to standardize the wound assessment process, such as a regular day of the week; and 2) find the best evidence addressing the wound assessment process, including measurement and documentation. No date or language restrictions were imposed on the search. Five clinical studies, 10 review articles, two practice guidelines, and one patient safety guideline/study/review publication were used to guide wound documentation improvement efforts.
Standardization of wound assessment process and wound measurement techniques. One review of the literature described the need for and methods of accurate wound assessment, including a framework for practice and accurate, uniform terms for assessment and documentation and the use of a mnemonic phrase to facilitate the practice of consistent wound assessment.5 No studies related to the designation of a specific day of the week for impaired skin documentation were found.
Best evidence of the assessment process. The literature identified a lack of consistency in practice and documentation as areas of concern. Subjective measurements of the wound bed — including descriptions of drainage, tissue appearance, edema, wound edges, and the surrounding skin — also were found to contribute to wound assessment inconsistencies.5 The literature review underscored that quantitative measurement of wounds is necessary for consistent documentation and allows the practitioner to evaluate treatment effectiveness.
Studies describing different wound measurement techniques (eg, rulers, wound tracings or molds, and photographs) affirm that a standardized method of wound measurement is necessary to ensure consistent patient care. Langemo et al11 evaluated four ruler length-and-width measurement techniques using plaster-of-Paris models to determine the closest measurement of actual surface area of a wound, subsequently recommending that clinicians measuring the wounds using a ruler use the same technique each time. The authors also recommended the measurement technique of “longest head to toe and the widest width side to side, perpendicular to length.”
The literature also noted that initial assessments of impaired skin such as pressure ulcers or wounds should include documentation of the impairment, including location and wound measurements.12 These assessment details must be measured consistently and documented regularly in the chart. Recommendations for measurement frequency vary, from each dressing change to weekly assessments to deterioration of patient condition. Inconsistent assessments and failure to assess and document impaired skin on admission is common.13
Reports about the use of wound documentation tools and protocols such as the Pressure Ulcer Prevention Protocol Interventions (PUPPI )14 and Barber Measuring Tool15 have been published. No information about tools or protocols that included the use of a consistent day-of-the-week mnemonic to remind staff that wound measurement is due could be found in the literature.
Within the past decade, imaging has been used to enhance wound measurement documentation. Houghton et al16 evaluated the validity and reliability of wound photography and found wound photographs to be reliable when the photography was completed by persons who had adequate clinical experience in chronic wound care. Photography may be a valuable tool to record pressure ulcer assessment, treatment, and prevention progress, but should not be considered a substitute for the written, detailed record.17
Quality improvement initiative. Before starting the initiative, all hospital policies related to pressure ulcers were reviewed. Consistent with AHCPR guidelines,3 skin assessments and documentation were to be completed on admission and every 8 hours thereafter. When skin impairment is discovered, the policy called for complete wound assessment and documentation, including descriptions and measurement. Follow-up measurements are to be completed weekly or more often if the wound deteriorates.
Retrospective chart audits for documentation of wound size and measurements for impaired skin (eg, open surgical incisions, skin tears, pressure ulcers, or lower extremity ulcers) in late 2005 showed that wound assessment documentation lacked appropriate details and content was inconsistent among nurses. Chart review results were shared with staff and members of the Skin Wound Ostomy Team Council. Brainstorming sessions were conducted with council members to develop a process for staff nurses to standardize the wound assessment process throughout all hospital units.
The concept “Measurement Monday” — a designated day of the week on which all wounds were to be completely assessed and documented — was proposed by a registered nurse team member and implemented. Wound measurement documentation was of particular importance. Thus, every Monday, nurses were to assess and measure all wounds. Care partners often assisted the nurse with patient positioning. Wound measurements were to be obtained using disposable measuring guides and the longest length by widest width technique and results entered into the progress notes. Wound assessment on the other 6 days of the week were conducted for the purpose of wound monitoring without measurement (ie, color, drainage, improvement or not).
Between January and March 2006, Measurement Monday education was provided to nurses on medical/surgical and intensive care units and included instruction regarding the use of a documented pressure ulcer staging system3 and wound size measurement techniques. Additionally, nurses were required to demonstrate accurate wound assessment, including measurement, to a WOCN or skin team member.
Subsequent random follow-up chart audits of patients with known skin impairments were completed from April through June 2006. This review showed wound size documentation was better but documentation of additional nurse-documented parameters such as measurement needed improvement. The hospital’s Nursing Quality Council began to assist with the effort to ensure a consistent assessment process. A registered nurse from this group developed a documentation tool, The Weekly 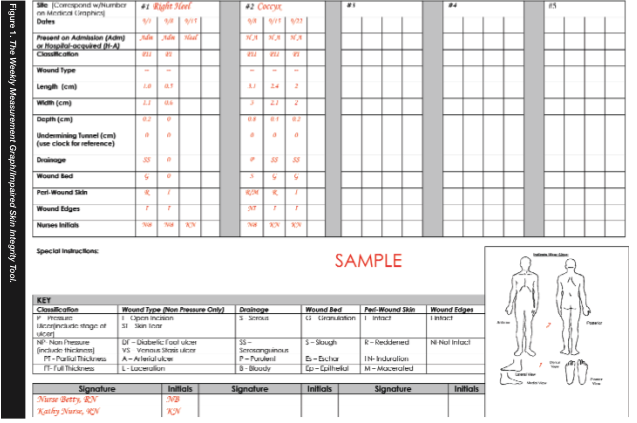 Measurement Graph/Impaired Skin Integrity Tool (see Figure 1), to ensure appropriate assessment data were recorded. The tool is used to document each skin impairment on a weekly basis, including details of the wound assessment/measurement. This instrument was introduced to the nursing staff throughout the hospital in January 2007, at which time a review of previous education also was provided. Additionally, ruler reminders with the Measurement Monday logo were distributed to the nursing units for placement on assignment boards next to names of patients requiring wound assessments.
Measurement Graph/Impaired Skin Integrity Tool (see Figure 1), to ensure appropriate assessment data were recorded. The tool is used to document each skin impairment on a weekly basis, including details of the wound assessment/measurement. This instrument was introduced to the nursing staff throughout the hospital in January 2007, at which time a review of previous education also was provided. Additionally, ruler reminders with the Measurement Monday logo were distributed to the nursing units for placement on assignment boards next to names of patients requiring wound assessments.
Random follow-up chart audits of patients with known skin impairments were again conducted between February and August 2007. In October 2007, the initiative was benchmarked against the literature to determine whether these efforts were consistent with the best evidence available.
Results
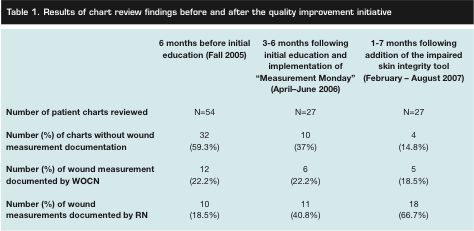
Average daily census at the facility over the course of the study was 175 to 180. Although the frequency of various wound etiologies was not recorded (the main focus of the reviews was on the presence and quality of wound assessment/measurement documentation), the overwhelming majority of the wounds reviewed were pressure ulcers. Other types of wounds included skin tears, open surgical wounds, and diabetic and venous stasis ulcers. On initial (baseline) chart review in late 2005, 32 out of 54 reviewed charts (59.3%) did not contain documentation of wound size measurements. Following initial education efforts and implementation of Measurement Monday in early 2006, chart reviews conducted from April through June 2006 showed that 38.5% of charts lacked wound size measurement documentation, a decrease of almost 21%. After implementing The Weekly Measurement Graph/Impaired Skin Integrity Tool in January 2007 and re-emphasizing prior education, follow-up chart reviews in February through August 2007 indicated further documentation improvements, with only 14.8% of charts lacking wound size measurement information (see Table 1).
 In addition to the improvement in chart audits, many nurses verbalized their satisfaction with the designated measurement day and The Weekly Measurement Graph/Impaired Skin Integrity Tool. The new form and processes allowed nursing staff to monitor wound progress more easily and saved nursing time when documenting. At every chart review point, the proportion of wound measurements recorded by the nurses, as opposed to the WOCN, increased.
In addition to the improvement in chart audits, many nurses verbalized their satisfaction with the designated measurement day and The Weekly Measurement Graph/Impaired Skin Integrity Tool. The new form and processes allowed nursing staff to monitor wound progress more easily and saved nursing time when documenting. At every chart review point, the proportion of wound measurements recorded by the nurses, as opposed to the WOCN, increased.
Discussion
No literature as yet exists to support use of a designated day of the week as a mnemonic for consistent wound assessment. The Measurement Monday process was found to help nurses be more consistent and efficient; anyone with a skin impairment is measured on Monday. This approach helped eliminate confusion regarding which patients needed to have skin/wound measurements completed.
The purpose of the Keast5 mnemonic was to provide nurses with a framework to recall what characteristics must be assessed in the management of chronic wounds. Although the Measurement Monday mnemonic did not provide such a system, The Weekly Measurement Graph/Impaired Skin Integrity Tool provided assessment prompts.
Current literature recommends the use of a consistent measurement technique. The Measurement Monday project did not endorse the use of any particular measurement tool, but the provision of rulers and documentation tool allowed for consistent documentation of linear measurement data. Langemo et al11 and Plassman et al18 support regular wound assessment, which includes the use of consistent measurement practices.
Approximately 6 months after the last chart audits, the authors’ facility transitioned to an electronic medical record (EMR). The weekly measurement tool was incorporated into the flowsheet documentation section of the new record. Although the appearance of the document changed, the same consistent assessment/measurement fields are available and a field to document wound exudate was added. No significant change in documentation compliance has been noted once staff became accustomed to the new EMR.
Implications for Practice and Research
Facilities facing the challenge of wound documentation might want to consider designating a specific day of the week for wound assessments and measurements. It also may be of benefit to match the number of initial chart audits and follow-up comparisons; a limitation of the Measurement Monday project was that the sample size of initial (54) and follow-up chart audits (27) differed.
This quality improvement initiative should be replicated on a larger scale and the reliability and validity of The Weekly Measurement Graph/Impaired Skin Integrity Tool need to be established. Future research also should include recording wound etiology to elucidate differences, if any, between different wound types. Replication of this initiative utilizing the EMR, as opposed to a paper tool, also would add value to the state of knowledge regarding impaired skin assessment/measurement documentation.
Conclusion
A rural tertiary care facility seeking to improve thoroughness and consistency of wound documentation embarked on a project that designated 1 day a week for wound assessment and record-keeping and implemented a weekly measurement tool. Chart reviews indicated that the proportion of incomplete records were reduced by almost 44.5%. Nurses expressed satisfaction with the new program. Measurement Monday warrants further study as a mnemonic that shows promise for lessening wound assessment/documentation challenges.
Acknowledgment
The authors acknowledge former skin team member Susan Lanzara for the idea of the “Measurement Monday.” They also thank other former skin team members: Molly Welch, Dawn Matteson, Deonna Kershner, Marylou Allen, Kathy Barrett-Corbett, Nellie Towers, and Pat Daniels for their work with the team and acknowledge all members of the Quality Council for their assistance, especially Melanie Nittenger for the development of The Weekly Measurement/Graph Impaired Skin Integrity Tool.
1. Lyder CH, Ayello EA. Pressure ulcers: a patient safety issue. In: Hughes RG (ed). Pressure Ulcers: A Patient Safety Issue. Rockville, MD: AHRQ Publication No. 08-0043;2008:Volume 1, 267–300.
2. Wound, Ostomy, and Continence Nurses Society. Guideline for Prevention and Management of Pressure Ulcers. Mt. Laurel, NJ: Wound, Ostomy, Continence Nurses Society;2003:3.
3. Bergstrom N, Bennett MA, Carlson CE, et al. Clinical Practice Guideline, No.15: Treatment of Pressure Ulcers. Rockville, MD. U.S. Department of Health and Human Services. Public Health Service, Agency for Health Care Policy and Research. 1994. AHCPR Publication No. 95-0652.
4. van Rijswijk L. The fundamentals of wound assessment. Ostomy Wound Manage. 1996;42(97):40–46.
5. Keast DH, Bowering CK, Evans AW, MacKean GL, Burrows C, D’Souza L. MEASURE: a proposed assessment framework for developing best practice recommendations for wound assessment. Wound Repair Regen. 2004;12(3):S1–S17.
6. Flanagan M. A practical framework for wound assessment 2: methods. Brit J Nur. 1997;6(1):6–11.
7. Russell L. The importance of wound documentation and classification. Brit J Nurs. 1999;8(20):1342–1354
8. Goldman RJ, Salcido R. More than one way to measure a wound: an overview of tools and techniques. Advances Skin Wound Care. 2002;15(5):236–243.
9. Hess CT. The art of skin and wound care documentation. Home Health Nurse. 2005;23(8):502–513.
10. Cuzzell J. Wound assessment and evaluation: wound assessment guidelines. Dermatol Nurs. 2002;14(4):265–266.
11. Langemo D, Anderson J, Hanson D, Hunter S, Thompson P. Measuring wound length, width, and area: which technique. Advances Skin Wound Care. 2008;21(1):42–45.
12. Brown G. Wound documentation. Advances Skin Wound Care. 2006;19(3):155–165.
13. O’Brien SP, Wind S, van Rijswijk L, Kerstein MD. Sequential biannual prevalence studies of pressure ulcers at Allegheny-Hahnemann University Hospital. Ostomy Wound Manage. 1998;44(3A suppl):78S– 88S.
14.Catania K, Huang C, James P, Ohr M, Madison M, Moran M. PUPPI: the pressure ulcer prevention protocol interventions. AJN. 2007;107(4):44–52.
15. Barber S. A clinically relevant wound assessment method to monitor healing progression. Ostomy Wound Manage. 2008;54(3):42–49.
16. Houghton PE, Kincaid CB, Campbell KE, Woodbury MG, Keast DH. Photographic assessment of the appearance of chronic pressure and leg ulcers. Ostomy Wound Manage. 2000;46(4):20–30.
17. Dufrene C. Photography as an adjunct in pressure ulcer documentation. Crit Care Nurs Quarterly. 2009;32(2):77–80.
18. Plassman P, Melhuish JM, Harding KG. Methods of measuring wound size: a comparative study. Ostomy Wound Manage. 1994;40(7):50–60.
